










Anzeige
Erschienen in:
14.12.2015 | Letter to the Editors
Rupture of sinus of Valsalva aneurysm into the left ventricle after dissecting through the interventricular septum mimicking aortic regurgitation
Erschienen in: Clinical Research in Cardiology | Ausgabe 6/2016
Einloggen, um Zugang zu erhaltenExcerpt
Sirs: A 21-year-old male presented with history of progressively worsening effort dyspnea of 2-year duration. There was no history of chest trauma, tearing chest or back pain, prolonged fever or joint pains prior to the onset of symptoms. He was diagnosed to have severe AR at the local hospital and managed medically for 2 years, till worsening symptoms and left ventricular dysfunction prompted referral to our center. At admission, the pulse rate was 72 per minute and right arm blood pressure was 140/70 mmHg. The jugular venous pressure was not raised. He had a long early diastolic murmur heard best over the third left intercostal space. The remainder of the physical examination was unremarkable. The hemogram and white blood cell count were normal. The electrocardiogram indicated sinus rhythm with prolonged PR interval. Chest X-ray showed gross cardiomegaly and pulmonary venous congestion (Fig. 1a). Transthoracic echocardiogram revealed aneurysm of right SoV that had dissected through the IVS and ruptured into the LV cavity (Fig. 1b–e and supplementary video clip 1–4). The LV was dilated with global hypokinesia and LV ejection fraction was 31 %. Aortic valve morphology was normal with trivial AR. Right heart catheterization showed the absence of oxygen step-up and pulmonary artery pressure 38/20 (mean 28) mmHg. Aortic root angiography showed dense opacification of the LV with normal coronary arteries, but could not reliably distinguish between aortic valve pathology and ruptured SoV aneurysm into the LV. Left ventricular end-diastolic pressure was 16 mm Hg. In light of these findings, the patient was specifically questioned and a history of sudden-onset chest pain and dyspnea while lifting a heavy weight 2 years ago was elicited. At subsequent surgery, the aortic root was found to be dilated with right SoV aneurysm that had dissected through the IVS and egressed into the LV; the aortic valve was tricuspid and appeared competent. The defect in the right aortic sinus was successfully repaired with a Dacron patch. The postoperative period was uneventful, and the patient was discharged from the hospital 8 days after surgery. Six months later the patient was symptomatically improved, though cardiomegaly and left ventricular dysfunction (ejection fraction 30 %) remained unchanged despite treatment with angiotensin-converting enzyme inhibitor, digoxin and diuretic.
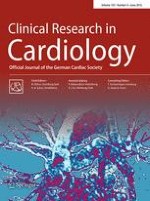
Fig. 1
a Preoperative chest X-ray. b–e Paired two-dimensional echocardiographic images without (left image) and with (right image) color flow mapping in b, c parasternal long-axis view, d modified 5-chamber view and e short-axis view showing ruptured aneurysm with flow arising from the right sinus of Valsalva (white arrows) and traversing the interventricular septum (asterisks) to egress into the left ventricle (yellow arrows). Ao aorta, LA left atrium, LV left ventricle, RV right ventricle
× ![]()
…