










Anzeige
Erschienen in:
25.06.2022 | Clinical Conundrum
Clinical Conundrum: Dysphagia Associated with Sleep Disorders
Erschienen in: Dysphagia | Ausgabe 2/2023
Einloggen, um Zugang zu erhaltenExcerpt
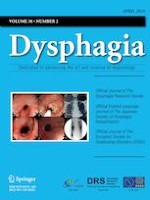
A 71-year-old woman presented at our dysphagia clinic with a history of progressive swallowing impairment and weight loss (9 kg) over the previous 2 years. She complained of post-deglutitory feeling of food stuck in her throat and severe sialorrhea. Three years before presentation, she started to experience nocturnal crisis of cough and dyspnea, which worsened and were accompanied by the presence of laryngeal stridor over the course of one year. She was then diagnosed with obstructive sleep apnea syndrome (OSAS) and started continuous positive airway pressure therapy (CPAP). When she came to our clinic, we performed a formal Fiberoptic Endoscopic Evaluation of Swallowing (FEES), that highlighted mild dysphagia for solid consistencies with residue in the valleculae, suggesting a possible reduced pharyngeal contractility with no other signs of dysphagia (Fig. 1). Considering the coexisting dysphagia, laryngeal stridor and sleep disorders, which raised the suspect of a bulbar involvement, we referred the patient to the neurologist of our neurodegenerative disease center.
Fig. 1
Aspiration of liquid (white-dyed water) with tracheal and laryngeal residues; pooling at the level of pyriform sinus is also present bilaterally
× ![]()
…