










Anzeige
Erschienen in:
01.11.2016 | Correspondence
Horner’s Syndrome in a Case of Granulocytic Sarcoma
Erschienen in: Indian Journal of Hematology and Blood Transfusion | Ausgabe 2/2017
Einloggen, um Zugang zu erhaltenExcerpt
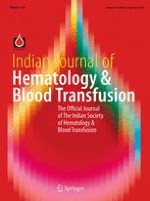
Horner’s syndrome is a unique neurological syndrome caused by interruption of the sympathetic supply to one half of the face including the ipsilateral eye. Irrespective of the location of the interruption of sympathetic pathway, Horner’s syndrome typically presents with a combination of ipsilateral miosis, partial ptosis and facial anhydrosis. It is primarily a clinical diagnosis which may be confirmed by pharmacological testing. Etiology can be broadly categorised depending upon the neuron involved (first, second or third order). A systematic approach to diagnostic evaluation of Horner’s syndrome is essential as the causes are heterogeneous and may range from benign to life threatening. We present a 50-years-old lady, with no previous comorbidities, who consulted a local physician for complaints of reduced sweating of right side of the face, drooping of right upper eyelid and right upper non anginal chest pain radiating to right upper limb. She also had low grade fever and easy fatigability for 15 days. Routine investigations revealed anemia (hemoglobin—8.5 g/dL), thrombocytopenia (23,000/mm3) and leucocytosis (total leucocyte count—22,900/mm3) with 29% blasts in peripheral smear. She was referred to our institute as a suspected case of acute leukemia. Physical examination at admission at our center revealed pallor. She was afebrile and her blood pressure was 120/84 mm of mercury and pulse rate of 102 per minute. She had right sided partial upper eyelid ptosis, miosis and apparent enophthalmos (Fig. 1). Rest of neurological examination was normal. The presence of ipsilateral hemifacial anhidrosis suggested extra-axial preganglionic right sided Horner’s syndrome. Rest of the systemic examination was unremarkable.
Fig. 1
Clinical photograph showing incomplete ptosis in the right eye, right pupil miosis (in comparison to right pupil) and enophthalmos of the right eye
× ![]()
…