
Summary
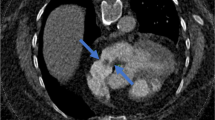
This prospective study investigates the frequency of patent foramen ovale (PFO), venous air embolism (VAE) and paradoxical air embolism (PAE) by transoesophageal echocardiography (TOE) in neurosurgical patients operated on in the sitting position. The risk of PAE after exclusion of PFO is assessed. A PFO was identified by pre-operative TOE and VAE and PAE by continuous intra-operative TOE. Sixty-two patients were divided into two groups, 22 patients were studied in group 1 (posterior fossa surgery) and group 2 (cervical surgery) contained 40 patients.
Pre-operative TOE demonstrated a PFO in 5 of the 22 patients in group 1 (23%). Patients with proven PFO were excluded from the sitting position. Two further patients of this group (12% of 17 patients), in whom a PFO had been excluded pre-operatively, nevertheless had PAE, air occurring in all cavities of the heart. In group 2 the incidence of PFO was 4 out of 40 patients (10%). No PAE was observed in this group. Three morphological types of VAE with different haemodynamic and ventilation changes were demonstrated. VAE was observed in 76% of all posterior fossa operations and in 25% of cervical laminectomies. We conclude that a pre-operative search for PFO is mandatory considering its incidence of 23% in group 1 and of 10% in group 2, and the risk of PAE. If a PFO is detected, the sitting position should be avoided. A residual risk for PAE remains despite exclusion of PFO because the reliability of TOE is limited. TOE is the method of choice for detecting VAE and PAE.
Similar content being viewed by others

References
Adornato DC, Gildenberg PL, Ferrario CM, Smart J, Frost EAM (1978) Pathophysiology of intravenous air embolism. Anesthesiology 49: 120–127
Black S, Ockert DB, Oliver WC, Cucchiara RF (1988) Outcome following posterior fossa craniotomy in patients in the sitting or horizontal position. Anesthesiology 69: 49–56
Black S, Muzzi D, Nishimura R, Cucchiara RF (1990) Pre-operative and intra-operative echocardiography to detect right-to-left shunt in patients undergoing neurosurgical procedures in the sitting position. Anesthesiology 72: 436–438
Cucchiara RF, Seward JB, Nishimura RA, Nugent M, Faust RJ (1985) Identification of patent foramen ovale during sitting position craniotomy by transesophageal echocardiography with positive airway pressure. Anesthesiology 63: 107–109
Durant TM, Long J, Oppenheimer MJ (1947) Pulmonary (venous) air embolism. Am Heart J 33: 269–281
Guggiari M, Lechat PH, Garen-Colonne C, Fusciardi J, Viars P (1988) Early detection of patent foramen ovale by two-dimensional contrast echocardiography for prevention of paradoxical air embolism during sitting position. Anesth Analg 67: 192–194
Furuya H, Okumura F (1984) Detection of paradoxical air embolism by transesophageal echocardiography. Anesthesiology 60: 374–377
Hagen PT, Scholz DG, Edwards WD (1984) Incidence and size of patent foramen ovale during the first ten decades of life: an autopsy study of 965 normal hearts. Mayo Clinic Proc 59: 17–20
Hey O, Fischer F, Reinery G, Steingass U, Knorre D (1983) Erkennung und Verhütung von Luftembolien während neuro-chirurgischer Eingriffe in sitzender Position. In: Ahnefeld FW, Bergmann H, Burri C, Dick W, Halmaghi M, Hossli G, Reulen HJ, Rügheimer E (eds) Anästhesie in der Neurochirurgie. Springer, Berlin Heidelberg New York Tokio, pp 197–209
Lynch JJ, Schuchard GH, Gross CM, Wann LS (1984) Prevalence of right-to-left atrial shunting in the healthy population: detection by Valsava manoeuver contrast echocardiography. Am J Cardiology 53: 1478–1480
Matjasko J, Petrozza P, Cohen M (1985) Anesthesia and surgery in the seated position: analysis of 554 cases. Neurosurgery 17: 695–702
Perkins NA, Bedford RF (1984) Hemodynamic consequences of PEEP in seated neurosurgical patients-implications for paradoxical air embolism. Anesth Analg 63: 429–432
Sato S, Toya S, Ohira T, Mine T, Greig NH (1986) Echocardiographic detention and treatment of intra-operative air embolism. J Neurosurg 64: 440–444
Standefer M, Bay JW, Trusso R (1984) The sitting position in neurosurgery: a retrospective analysis of 488 cases. Neurosurgery 14: 649–658
Zasslow MA, Pearl RG, Larson CP, Silverberg G, Shuer LF (1988) PEEP does not effect atrial-right atrial pressure difference in neurosurgical patients. Anesthesiology 68: 760–763
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Papadopoulos, G., Kuhly, P., Brock, M. et al. Venous and paradoxical air embolism in the sitting position. A prospective study with transoesophageal echocardiography. Acta neurochir 126, 140–143 (1994). https://doi.org/10.1007/BF01476424
Issue Date:
DOI: https://doi.org/10.1007/BF01476424