
Summary
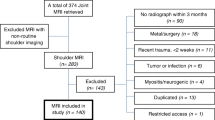
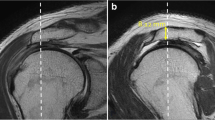
Based on a retrospective study of 179 MRI records covering four populations (patients presenting with impingement without known injury (n=90), post-traumatic shoulder pain (n=28), instability or dislocation (n=36) and controls (n=25)), morphologic criteria are suggested to define presumedly normal arches and arches compatible with subacromial impingement. The subacromial arch is presumed normal or without impingement if the sagittal and frontal views show it to be parallel to the humeral head, and/or if there is a fatty layer interposed between the arch and the supraspinatus m. The arch is presumed “aggressive” or actually capable of giving rise to impingement if, in either the sagittal or frontal view, there is a zone of narrowing of the subacromial passage with an impression of the arch on the supraspinatus tendon or tendinous thinning at this level or just lateral to this narrowed zone. Based on these criteria, study of the 179 MRI records demonstrated a significant difference of distribution of the arches in the four populations. “Aggressive” arches were found in 45.5% of patients with impingement, 25% of patients with posttraumatic pain, 8.9% of patients with an acute or recurrent dislocation and 12% of controls. Conversely, a presumedly normal arch was found in 56% of the controls, 55% of patients with dislocation, 25% of posttraumatic painful shoulders and only 5.5% of patients with clinical impingement. Subacromial impingement may be due to the type 3 acromial dysplasia described by Bigliani or to a thickening of the coracoacromial ligament at its acromial attachment. This study was supplemented by 15 anatomic dissections which confirmed the regularity of attachment of the coracoacromial ligament at the inferior aspect of the acromion along its lateral border.
Résumé
A partir de la lecture rétrospective de 179 dossiers d'IRM représentant quatre populations (patients présentant un conflit sans traumatisme reconnu (n=90), une douleur d'épaule post-traumatique (n=28), une instabilité ou une luxation (n=36) et sujets témoins (n=25)), les auteurs proposent des critères morphologiques pour définir des voûtes présumées normales et des voûtes susceptibles de rendre compte d'un conflit sous acromial. La voûte sous acromiale est présumée “normale” ou non conflictuelle si, sur les vues sagittales et frontales, elle apparait parallèle à la tête humérale et/ou il existe un liseré graisseux qui s'interpose entre la voûte et le m. supra-épineux. La voûte sous acromiale est présumée agressive ou susceptible de rendre compte d'un conflit si, sur l'une des vues sagittale ou frontale, il est observé une zone de rétrécissement du défilé sous acromial avec une empreinte de la voûte sur le tendon du m. supra-épineux ou un amincissement tendineux au niveau ou juste en dehors de cette zone de rétrécissement. A partir de ces critères, la lecture des 179 dossiers d'IRM permet de mettre en évidence une différence significative de répartition des voûtes dans les quatre populations. Les voûtes agressives s'observent chez 45.5 % des patients présentant un conflit, 25 % des patients pr%esentant une douleur au décours d'un traumatisme, 8.9 % des sujets examinés au décours d'une luxation aigue ou récidivante et 12 % des sujets témoins. A l'inverse, la voûte présumée normale est retrouvée chez 56 % des sujets témoins, 55 % des patients examinés pour une luxation, 25 % des douleurs d'épaule post traumatique et seulement 5.5 % des patients présentant un conflit clinique. Le conflit sous acromial peut être le fait d'une dysplasie acromiale de type 3 décrit par Bigliani ou d'un épaississement du ligament au niveau de son insertion acromiale. Ce travail est complété par 15 dissections anatomiques qui confirment la constance de l'insertion du ligament coraco-acromial sur la face inférieure de l'acromion le long de son bord latéral.
Similar content being viewed by others

References
Bigliani LU, Norris TR, Fisher et al (1983) The relationship between unfused acromial epiphysis and subacromial impingement lesions. Orthop Trans 7: 138
Bigliani LU, Morrison DS, April EW (1986) The morphology of the acromion and its relationship to rotator cuff tears (abstract). Orthop Trans 10: 228
Brodie GC (1889–1890) Note on the transverse-humeral, coracoacromial, and coracohumeral ligaments. J Anat Physiol 24: 247–252
Cayotte JL, Loesher JP, Jandeaux AM (1966) La voûte acromio-coracoïdienne et les mouvements de l'articulation scapulo-humérale. Arch Anat Pathol 14: 96–97
Cornejo RH (1936) Sur la signification et la fonction du ligament acromio-coracoïdien. Ann Anat Pathol 13: 383–393
Gagey N, Idy-Peretti I, Gagey O, Mazas F (1991) Apport de l'IRM dans le bilan pré-opératoire de la coiffe des rotateurs. Rev Chir Orthop 8: 521–529
Gerber G, Terrier F, Ganz R (1985) The role of the coracoid process in the chronic impingement syndrome. J Bone Joint Surg [Br] 67: 703–708
Goldwaith JE (1909) Anatomic and mechanical study of the shoulder joint explaining painful shoulder, recurrent dislocations and brachial neuralgias and neuritis. Am J Orth Surg 6: 579–606
Warwick R, Williams PL (1973) Gray's Anatomy, 35th edn. Longman, p 424
Jobe CM (1990) Gross anatomy of the shoulder. In: Rockwood CA, Matson FA (eds) The Shoulder, tome I, Saunders, Philadelphia, p 45
Liberson F (1937) Os acromial, a contested anomaly. J Bone Surg 19: 683–689
Morestin (1894) Acromion formant un os isolé. Bull Soc Anat Paris 681
Neer CS (1972) Anterior acromioplasty for the chronic impingement syndrome in the shoulder. Preliminary report. J Bone Joint Surg [Am] 54: 41–50
Neer CS (1983) Impingement lesions. Clin Orthop 173: 70–77
Paturet G (1951) Traité d'Anatomie Humaine. Membre supérieur et inférieur, tome 2. Masson, Paris, p 15
Renoux S, Monet J, Pupin P et al (1986) Preliminary note on biometric data relating to the human coraco-acromial arch. Surg Radiol Anat 8: 189–195
Testut L, Latarget V (1948) Traité d'Anatomie Humaine. Ostéologie arthrologie et myologie, tome I. Doin, p 563
Vallois HV (1926) Arthrologie. In: Poirier P, Charpy A (eds) Traité d'anatomie humaine, tome I, fasc. 2, 4th ed. Masson, Paris, p 133
Vallois HV (1932) Omoplate humain. Bull Mem Soc Anat Paris 3, VIII: 139
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Gagey, N., Ravaud, E. & Lassau, J. Anatomy of the acromial arch: correlation of anatomy and magnetic resonance imaging. Surg Radiol Anat 15, 63–70 (1993). https://doi.org/10.1007/BF01629865
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01629865