
Abstract
Purpose
Due to the progressive aging of the surgical population, the proportion of patients with coronary artery disease (CAD) is likely to increase. The effects of the new inhalational anaesthetic sevoflurane must be determined in patients with known CAD.
Methods
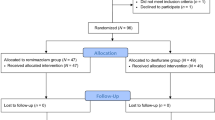
This multicentre, randomized, open-label study compared the haemodynamic and cardiovascular effects of sevoflurane and isoflurane with fentanyl in 284 ASA physical status II–IV patients undergoing elective coronary artery bypass graft (CABG).
Results
Satisfactory records were available in 272 patients, 139 sevoflurane (Group S) and 133 isoflurane (Group I). There were no differences between groups for demographic data except that more patients in Group S were taking preoperative beta-blockers (P = 0.03). The mean end-tidal MAC and MAC · hr requirements between groups were not different (Group S received 0.63 ± 0.02 MAC and 1.00 ± 0.05 MAC · hr while Group I received 0.58 ± 0.02 MAC and 0.92 ± 0.05 MAC · hr P = NS). The preCPB use of intravenous fentanyl was not different between groups. There was a similar decrease in haemodynamic variables in both groups after induction that persisted throughout the preCPB period. The incidence of preCPB myocardial ischaemia, adverse haemodynamic events and use of vasoactive drugs did not differ between groups. The incidence of postoperative myocardial infarction was 2.2% for Group S and Group I was 4.5% (P = NS). There were five postoperative deaths, one of which was attributed to a cardiac cause (Group I).
Conclusion
In patients undergoing elective CABG with low risk factors, either sevoflurane or isoflurane, combined with fentanyl, provided an acceptable preCPB haemodynamic profile and cardiac outcomes.
Résumé
Objectif
A cause du vieillissement de la population chirurgicale, une augmentation proportionnelle de patients souffrant de maladie coronarienne athérosclérotique (MCAS) est à prévoir. Les effets des nouveaux agents volatils anesthésiques, tels le desflurane et le sévoflurane, doivent être déterminés chez les patients ayant une MCAS.
Méthode
Cette étude ouverte, multicentrique, randomisée a comparé les effets hémodynamiques et cardio-vasculaires du sévoflurane et de l’isoflurane en association avec du fentanyl chez 284 patients ASA II–IV subissant une chirurgie de revascularisation myocardique (CABG).
Résultats
Un total de 272 patients évaluables ont servi à l’analyse dont 139 patients sévoflurane (Groupe S) et 133 patients isoflurane (Groupe I), Il n ’y avait pas de différence démographique entre les groupes à l’exception d’une utilisation préopératoire plus grande de bêta-bloqueurs dans le Groupe S (P = 0.03). La moyenne du MAC de fin d’expiration et le MAC·hr pour chacun des groupes étaient similaires (Groupe S a reçu 0.63 ± 0.02 MAC et 1.00 ± 0.05 MAC·hr tandis que le Groupe I a reçu 0.58 ± 0.02 MAC et 0.92 ± 0.05 MAC·hr; P = NS). L’utilisation du fentanyl préCEC était similaire. A la suite de l’induction et durant le maintien de l’anesthésie préCEC, une réduction similaire des paramètres hémodynamiques fut enregistrée. L’incidence d’ischémie myocardique préCEC, d’événements hémodynamiques adverses et l’utilisation d’agents vasoactifs étaient similaires. L’incidence d’infarctus du myocarde pour le Groupe S est de 2.2% et 4.5% pour le Groupe I (P = NS). Il y eut cinq décès postopératoires, dont un était attribué à une cause cardiaque (Groupe I).
Conclusion
Pour des patients à bas risque subissant une CABG, le sévoflurane et l’isoflurane, en association au fentanyl, procurent un profil hémodynamique préCEC et des résultats cardiaques acceptables.
Article PDF
Similar content being viewed by others


References
Mangano DT, Browner WS, Hollenberg M, et al. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. N Engl J Med 1990; 323: 1781–8.
Moffitt EA, Sethna DH. The coronary circulation and myocardial oxygenation in coronary artery disease: effects of anesthesia. Anesth Analg 1986; 65: 395–410.
Hoeft A, Sonntag H, Stephan H, Kettler D. The influence of anesthesia on myocardial oxygen utilization efficiency in patients undergoing coronary bypass surgery. Anesth Analg 1994; 78: 857–66.
Buffington CW, Romson JL, Levine A, Duttlinger NC, Huang AH. Isoflurane induces coronary steal in a canine model of chronic coronary occlusion. Anesthesiology 1987; 66:280–92.
Slogoff S, Keats AS, Dear WE, et al. Steal-prone coronary anatomy and myocardial ischemia associated with four primary anesthetic agents in humans. Anesth Analg 1991; 72: 22–7.
Miller DR, Wellwood M, Teasdale SJ, et al. Effects of anaesthetic induction on myocardial function and metabolism: a comparison of fentanyl, sufentanil and alfentanil. Can J Anaesth 1988; 35: 219–33.
Thomson IR, Putnins CL. Adverse effects of pancuronium during high-dose fentanyl anesthesia for coronary artery bypass grafting. Anesthesiology 1985; 62: 708–13.
Helman JD, Leung JM, Bellows WH, et al. The risk of myocardial ischemia in patients receiving desflurane versus sufentanil anesthesia for coronary artery bypass graft surgery. Anesthesiology 1992; 77: 47–62.
Weiskopf RB, Moore MA, Eger EI II, et al. Rapid increase in desflurane concentration is associated with greater transient cardiovascular stimulation than with rapid increase in isoflurane concentration in humans. Anesthesiology 1994; 80: 1035–45.
Eger EI II. New inhaled anesthetics. Anesthesiology 1994; 80: 906–22.
Frink EJ Jr, Malan TP, Atlas M, Dominguez LM, DiNardo JA, Brown BR Jr. Clinical comparison of sevoflurane and isoflurane in healthy patients. Anesth Analg 1992; 74: 241–5.
Frink EJ Jr, Malan TP Jr, Isner RJ, Brown EA, Morgan SE, Brown BR Jr. Renal concentrating function with prolonged sevoflurane or enflurane anesthesia in volunteers. Anesthesiology 1994; 80: 1019–25.
Harkin CP, Pagel PS, Kersten JR, Hettrick DA, Warltier DC. Direct negative inotropic and lusitropic effects of sevoflurane. Anesthesiology 1994; 81: 156–67.
Bernard J-M, Wouters PF, Doursout M-F, Florence B, Chelly JE, Merin RG. Effects of sevoflurane and isoflurane on cardiac and coronary dynamics in chronically instrumented dogs. Anesthesiology 1990; 72: 659–62.
Nakamura K, Toda H, Hatano Y, Mori K. Comparison of the direct effects of sevoflurane, isoflurane and halothane on isolated canine coronary arteries. Can J Anaesth 1993; 40:257–61.
Kersten JR, Brayer AP, Pagel PS, Tessmer JP, Warltier DC. Perfusion of ischemic myocardium during anesthesia with sevoflurane. Anesthesiology 1994; 81: 995–1004.
Larach DR, Schuler HG. Direct vasodilation by sevoflurane, isoflurane, and halothane alters coronary flow reserve in the isolated rat heart. Anesthesiology 1991; 75: 268–78.
Ramsay JG, DeLima LGR, Wynands JE, O’Connor JP, Ralley FE, Robbins GR. Pure opioid versus opioidvolatile anesthesia for coronary artery bypass graft surgery: a prospective, randomized, double-blind study. Anesth Analg 1994; 78: 867–75.
Slogoff S, Keats AS. Does perioperative myocardial ischemia lead to postoperative myocardial infarction? Anesthesiology 1985; 62: 107–14.
Mangano DT, Siliciano D, Hollenberg M, et al. Postoperative myocardial ischemia. Therapeutic trials using intensive analgesia following surgery. Anesthesiology 1992; 76: 342–53.
Priebe H-J. Isoflurane and coronary hemodynamics. Anesthesiology 1989; 71: 960–76.
Slogoff S, Keats AS. Randomized trial of primary anesthetic agents on outcome of coronary artery bypass operations. Anesthesiology 1989; 70: 179–88.
Tuman KJ, McCarthy RJ, Spiess BD, DaValle M, Dabir R, Ivankovich AD. Does choice of anesthetic agent significantly affect outcome after coronary artery surgery? Anesthesiology 1989; 70: 189–98.
Leung JM, Hollenberg M, O’Kelly BF, Kao A, Mangano DT, the SPI Research Group. Effects of steal-prone anatomy on intraoperative myocardial ischemia. J Am Coll Cardiol 1992; 20: 1205–12.
Pulley DD, Kirvassilis GV, Kelermenos N, et al. Regional and global myocardial circulatory and metabolic effects of isoflurane and halothane in patients with steal-prone coronary anatomy. Anesthesiology 1991; 75: 756–66.
Diana P, Tullock WC, Gorcsan J III, Ferson PF, Arvan S. Myocardial ischemia: a comparison between isoflurane and enflurane in coronary artery bypass patients. Anesth Analg 1993; 77: 221–6.
Mangano DT. Anesthetics, coronary artery disease, and outcome: unresolved controversies (Editorial). Anesthesiology 1989; 70: 175–78.
Leung JM, Goehner P, O’Kelly BF, et al. Isoflurane anesthesia and myocardial ischemia: comparative risk versus sufentanil anesthesia in patients undergoing coronary artery bypass graft surgery. Anesthesiology 1991; 74: 838–47.
Higgins TL, Estafanous FG, Loop FD, Beck GJ, Blum JM, Paranandi L. Stratification of morbidity and mortality outcome by preoperative risk factors in coronary artery bypass patients. A clinical severity score. JAMA 1992; 267: 2344–8.
Jain U. Myocardial infarction during coronary artery bypass surgery. J Cardiothorac Vasc Anesth 1992; 6: 612–23.
Wynands JE, Sheridan CA, Kelkar K. Coronary artery disease and anaesthesia (experience in 120 patients for revascularization of the heart). Can Anaesth Soc J 1967; 14: 382–98.
Hall RI. Anaesthesia for coronary artery surgery — a plea for a goal-directed approach. Can J Anaesth 1993; 40: 1178–94.
Tarnow J, Markschies-Hornung A, Schulte-Sasse U. Isoflurane improves the tolerance to pacing-induced myocardial ischemia. Anesthesiology 1986; 64: 147–56.
Davis RF, Sidi A. Effect of isoflurane on the extent of myocardial necrosis and on systemic hemodynamics, regional myocardial blood flow, and regional myocardial metabolism in dogs after coronary artery occlusion. Anesth Analg 1989; 69: 575–86.
Warltier DC, Al-Wathiqui MH, Kampine JP, Schmeling WT. Recovery of contractile function of stunned myocardium in chronically instrumented dogs is enhanced by halothane or isoflurane. Anesthesiology 1988; 69: 552–65.
Author information
Authors and Affiliations
Consortia
Additional information
This study was supported by a grant from Abbott Laboratories, Ltd, Chicago, IL.
Rights and permissions
About this article
Cite this article
Searle, N.R., Martineau, R.J., Conzen, P. et al. Comparison of sevoflurane/fentanyl and isoflurane/fentanyl during elective coronary artery bypass surgery. Can J Anaesth 43, 890–899 (1996). https://doi.org/10.1007/BF03011801
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011801