
Abstract
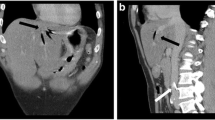
A patient is presented who failed to regain consciousness after an apparently uneventful nine-hour revision of a total hip replacement. There were no clinically important haemodynamic changes during the operation, and oxygen saturation, capnography and acid base balance were normal throughout. Postop CT of the head showed a large left MCA infarct with midline shift. At autopsy, the patient was found to have a previously unsuspected patent foramen ovale, and a venous embolus in the left internal carotid artery, which probably had originated from the periprostatic venous plexus with a large infarct in the distribution of the left anterior and middle cérébral arteries. The authors conclude that massive paradoxical venous emboli can occur during surgery with minimal haemodynamic changes.
Résumé
Un patient qui ne s’est pas réveillé après une révision d’un remplacement total de la hanche de neuf heures sans complication apparente est présenté. Il n’y avail aucune altération hémodynamique ciinique importante durant l’opération el la saturation d’oxygène, la capnographie et l’équilibre acide base furent normaux à travers la procedure. Un CT scan cérébral en postop a démontré un grand infarctus de l’artère cérébral moyenne gauche avec un déplacement de la ligne médiane. A l’autopsie, on trouva un foramen oval non suspecte et une embolie veineuse dans l’artère carotide interne gauche probalement provenant du plexus veineux périprostatique avec un large infarctus dans le territoire de distribution des artères cérébrales moyenne et antérieure gauche. Les auteurs concluent quune embolie veineuse paradoxale massive peut survenir lors de la chirurgie avec des altérations hémodynamiques minimes.
Article PDF
Similar content being viewed by others


References
Denlinger JK. Prolonged emergence and failure to regain consciousness. In: Orkin FK, Cooperman LH (Eds.). Complications in Ancsthcsiology. Philadelphia: J.B. Lippincott Company, 1983; 368–99.
Oliver SR, Cucchiara RF, Warner MA, Muir JJ. Unexpected focal neurological deficit on emergence from anesthesia: a report of three cases. Anesthesiology 1987; 67: 823–6.
Buckland RW, Manners JM. Venous air embolism during ncurosurgery: a comparison of various methods of detection in man. Anaesthcsia 1976; 31: 633–43.
Gronert GA, Messick JM, Cucchiara RF, Michenfetder JD. Paradoxical air cmbolism from a patent foramen ovalc. Ancsthesiology 1979; 50: 548–9.
Root B, Levy MN, Pollack S, Mortimer L, Kalindi P. Gas embolism death after laparoscopy delayed by “trapping” in portal circulation. Ancsth Analg 1978; 57: 232–7.
Schwartz SI. Principles of Surgery. Singapore. McGraw Hill Book Co. 1989; 470–2.
Jones HR, Caplan LR, Come PL, Swinton JrNW, Breslin DJ. Cerebral emboli of paradoxical origin. Ann Neurol 1983; 13: 314–9.
Ropper AH, Wechsler LR, Wilson LS. Carotid fruit and the risk of stroke in elective surgery. N Engl J Med 1982; 307: 1388–90.
Hart RG, Easton JD. Management of cervical bruits and carotid stenosis in prcopcrative patients. Stroke 1983; 14: 290–7.
Lechat P, Mas JL, Lascault G et al. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med 1988; 318: 1148–53.
Mohr JP. Cryptogenic stroke. N Engl J Med 1988; 318: 1197–38.
Webster MWI, Chancellor AM, Smith HJ, Swift DL, Sharpe DN, Bass NM. Patent foramen ovale in young stroke patients. Lancet 1988; 2: 11–2.
Thompson T, Evans W. Paradoxical Embolism. Q J Med 1930; 23: 135–50.
Meister SG, Grossman W, Dexter L, Dalen JE. Paradoxical embolism: diagnosis during life. Am J Med 1972; 53: 292–8.
Bitler J, Johnson MR, Adams JrHP, Kerber RE, Toffol GJ, Butler MJ. Echocardiographic evaluation of young adults with nonhemorrhagic cerebral infarction. Stroke 1986; 17: 608–12.
Cheng T. Paradoxical Embolism. A diagnostic challenge and its detection during life. Circulation 1976; 53: 565–8.
Rosenow EC III,Osmundson PJ, Brown JL. Pulmonary embolism. Mayo Clin Proc 1981; 56: 161–78.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Liu, S., Holley, H.S., Stulberg, S.D. et al. Failure to awaken after general anaesthesia secondary to paradoxical venous embolus. Can J Anaesth 38, 335–337 (1991). https://doi.org/10.1007/BF03007624
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03007624