
Abstract
Objective
Acetabular fractures pose a great surgical challenge for orthopedic trauma surgeons. We believe that the Stoppa approach with an iliac window extension, previously described as a modified Stoppa approach is adequate for the majority of acetabular fractures excluding those with predominant posterior wall involvement. In this paper we will present our experience in using the Stoppa approach, its indications, preparations, the detailed surgical approach, complications and the different tips used in this relatively modern approach.
Indications
All simple and combined fracture types that involve the anterior column of the pelvis including the quadrilateral plate.
Contraindications
Posterior wall or extensive posterior column involvement. Transverse and T-fractures with mainly posterior displacement.
Surgical technique
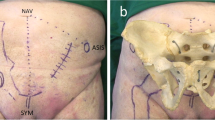
Suprapubic, intrapelvic approach, extending from the symphysis pubis anteriorly to the sacroiliac joint posteriorly. Superficial landmarks are identical to the Pfannenstiel approach, the rectus abdominis muscles are longitudinally dissected, the symphysis pubis is exposed and a sub-periosteal deep surgical dissection is carried out along the anterior column and the quadrilateral plate, and posteriorly toward the greater sciatic notch and the sacroiliac joint.
Results
In a 5-year review of 60 acetabular fractures that underwent open reduction and internal fixation using the modified Stoppa approach, there were 36% anterior column fractures, 28% both-column fractures, the rest being anterior column with posterior hemi transverse fractures, transverse and T-fractures. Any extension of the fracture to the iliac wing necessitated an additional lateral window (93% of cases). In cases with posterior displacement, an additional approach was utilized to address a posterior wall fracture. All fractures healed within 12 weeks. Mean Merle d’Aubigné score was 15.22. Postoperative radiological evaluation revealed anatomical reduction in 54% of the patients, satisfactory in 43%, and unsatisfactory in 3% of the patients. Overall there were 15 minor and major complications
Zusammenfassung
Operationsziel
Azetabulumfrakturen stellen eine große chirurgische Herausforderung für Orthopäden und Unfallchirurgen dar. Unserer Meinung nach ist der Stoppa-Zugang mit Erweiterung durch ein iliakales Fenster, zuvor als modifizierter Stoppa-Zugang beschrieben, für die Mehrzahl der Azetabulumfrakturen geeignet, außer bei vorherrschender Beteiligung der hinteren Wand. In diesem Artikel präsentieren wir unsere Erfahrungen mit dem Zugang nach Stoppa, seine Indikationen, Präparationsverfahren, das detaillierte chirurgische Vorgehen, Komplikationen und verschiedene Tipps, die bei diesem relativ neuen Ansatz zum Einsatz kommen.
Indikationen
Sämtliche einfachen und kombinierten Frakturtypen, an denen der vordere Pfeiler des Beckens einschließlich der quadrilateralen Fläche beteiligt ist.
Kontraindikationen
Beteiligung der Hinterwand oder ausgedehnte Beteiligung des hinteren Pfeilers. Quer- und T-Frakturen mit überwiegend hinterer Dislokation.
Operationstechnik
Suprapubischer, intrapelviner Zugang, der sich vorn von der Symphyse bis hinten zum Sakroiliakalgelenk erstreckt. Orientierungspunkte an der Oberfläche identisch wie beim Pfannenstiel-Zugang, Längsdurchtrennung der Fasern des M. rectus abdominis, Darstellung der Symphyse und tiefe subperiostale chirurgische Dissektion entlang des vorderen Pfeilers und der quadrilateralen Fläche sowie hinten in Richtung Incisura ischiadica major und Sakroiliakalgelenk.
Ergebnisse
In einer 5-Jahres-Übersicht über 60 Azetabulumfrakturen mit offener Reposition und interner Osteosynthese über einen modifizierten Stoppa-Zugang lagen in 36% der Fälle Frakturen des vorderen Pfeilers vor, in 28% 2-Pfeiler-Frakturen, in den übrigen Fällen Frakturen des vorderen Pfeilers mit hinterer Hemiquerfraktur, Quer- und T-Frakturen. Bei Ausdehnung der Fraktur bis zur Darmbeinschaufel war ein zusätzliches laterales Fenster erforderlich (93% der Fälle). In Fällen mit hinterer Dislokation wurde ein zusätzlicher Zugang zur Versorgung einer Hinterwandfraktur verwendet. Alle Frakturen heilten innerhalb von 12 Wochen. Der Score nach Merle d’Aubigné lag im Mittel bei 15,22. Die postoperative radiologische Evaluation ergab bei 54% der Patienten eine anatomische Reposition, zufriedenstellend war die Reposition bei 43% und nicht zufriedenstellend bei 3%. Insgesamt gab es 15 kleinere und größere Komplikationen.














Similar content being viewed by others


References
Anderson RC, O’Toole RV, Nascone JW et al (2010) Modified Stoppa approach for acetabular fractures with anterior and posterior column displacement: quantification of radiographic reduction and analysis of interobserver variability. J Orthop Trauma 24:271–278
Bray TJ, Esser M, Fulkenson L (1987) Osteotomy of the trochanter in open reduction an internal fixation of acetabular fractures. J Bone Joint Surg 69:711–717
Cole JD, Bolhofner BR (1994) Acetabular fracture fixation via a modified Stoppa limited intrapelvic approach. Description of operative technique and preliminary treatment results. Clin Orthop 305:112–123
Darmanis S, Lewis A, Mansoor A (2007) Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat 20:433–439
Fishmann AJ, Greeno RA, Brooks LR, Matta JM (1994) Prevention of deep vein thrombosis and pulmonary embolism in the acetabular and pelvic fracture surgery. Clin Orthop Relat Res 305:133–137
Goulet JA, Bray TJ (1989) Complex acetabular fractures. Clin Orthop Relat Res 240:9–20
Helfet DL, Borrelli J, DiPasquale T, Sanders R (1992) Stabilization of acetabular fractures in elderly patients. J Bone Joint Surg Am 74:753–765
Guy P, Al-Otaibi M, Harvey E, Helmy N (2010) The ‘safe zone’ for extra-articular screw placement during intra-pelvic acetabular surgery. J Orthop Trauma 24:279–283
Helfet DL, Schmeling GJ (1994) Management of the complex acetabular fractures through single nonextensile exposures. Clin Orthop Relat Res 305:58–68 (Review)
Jakob M, Droeser R, Zobrist R et al (2006) A less invasive anterior intrapelvic approach for the treatment of acetabular fractures and pelvic ring injuries. J Trauma 60:1364–1370
Johnson EE, Eckardt JJ, Letournel E (1987) Extrinsic femoral artery occlusion following internal fixation of an acetabular fracture: a case report. Clin Orthop Relat Res 217:209–213
Judet R, Judet J, Letournel E (1964) Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am 46:1615–1646
Kebaish AS, Roy A, Rennie W (1991) Displaced acetabular fractures. Long-term follow-up. J Trauma 31:1539–1542
Kloen P, Siebenrock KA, Ganz R (2002) Modification of the ilioinguinal approach. J Orthop Trauma 16:586–593
Letournel E (1961) Les fractures du cotyle, etude d’une serie de 75 cas. J de Chirurgie 82:47–87 [French]
Letournel E (1980) Acetabulum fractures: classification and management. Clin Orthop Relat Res 151:81–106
Letournel E (1993) The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 292:62–76 (Review)
Letournel E, Judet R (1993) Fractures of the acetabulum, 2nd. edn. Springer Verlag, New York
Letournel E (1994) Fractures of the acetabulum. A study of a series of 75 cases. 1961. Clin Orthop Relat Res 305:5–9
Mast J, Jakob R, Ganz R (1989) Planning and reduction techniques in fracture surgery. Springer Verlag, Berlin
Matta JM (1994) Operative treatment of acetabular fractures through the ilioinguinal approach. A 10-year perspective. Clin Orthop Relat Res 305:10–19
Matta JM (1986) Operative indications and choice of surgical approach for fractures of the acetabulum. Tech Orthop 1:13–22
Matta JM (2006) Operative treatment of acetabular fractures through the ilioinguinal approach. A 10-year perspective. J Orthop Trauma 20(Suppl 1):20–29
Mears DC (1999) Surgical treatment of acetabular fractures in elderly patients with osteoportic bone. J Am Acad Orthop Surg 7:128–141 (Review)
Mears DC, Rubash HE (1985) Fractures of the acetabulum. Hip 1985:95–113
Montgomery KD, Geerts WH, Potter HG, Helfet DL (1997) Practical management of venous thromboembolism following pelvic fractures. Orthop Clin North Am 28:397–404 (Review)
Ponsen KJ, Joosse P, Schigt A et al (2006) Internal fracture fixation using the Stoppa approach in pelvic ring and acetabular fractures: technical aspects and operative results. J Trauma 61:662–667
Probe R, Reeve R, Lindsey RW (1992) Femoral artery thrombosis after open reduction of an acetabular fracture. Clin Orthop Relat Res 283:258–260
Qureshi AA, Archdeacon MT, Jenkins MA et al (2004) Infrapectineal plating for acetabular fractures: a technical adjunct to internal fixation. J Orthop Trauma 18:175–178
Reinert CM, Bosse MJ, Poka A et al (1988) A modified extensile exposure for the treatment of complex or malunited acetabular fractures. J Bone Joint Surg Am 70:329–337
Routt ML, Swiontkowski MF (1990) Operative treatment of complex acetabular fractures. Combined anterior and posterior exposures during the same procedure. J Bone Joint Surg Am 72:897–904
Sagi HC, Afsari A, Dziadosz D (2010) The anterior intra-pelvic (Modified Rives-Stoppa) approach for fixation of acetabular fractures. J Orthop Trauma 24:263–270
Stoppa RE, Rives JL, Warlaumont CR et al (1984) The use of Dacron in the repair of hernias of the groin. Surg Clin North Am 64:269–285
Stoppa RE (1989) The treatment of complicated groin and incisional hernias. World J Surg 13:545–554
Tannast M, Siebenrock KA (2009) Die operative behandlung der azetabulum-T-Fraktur über eine chirurgische Hüftluxation oder einen Stoppa-Zugang. Oper Orthop Traumatol 21:251–269
Conflict of interest
On behalf of all authors, the corresponding author states that there are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khoury, A., Weill, Y. & Mosheiff, R. The Stoppa approach for acetabular fracture. Oper Orthop Traumatol 24, 439–448 (2012). https://doi.org/10.1007/s00064-011-0093-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00064-011-0093-z