
Abstract
Background
Current protocols for functional MR urography (fMRU) require long scan times, limiting its widespread use.
Objective
Our goal was to use pre-defined criteria to reduce the number of sequences and thus the examination time without compromising the morphological and functional results.
Materials and methods
The standard fMRU protocol in our department consists of eight sequences, including a 17-min dynamic post-contrast scan. Ninety-nine children and young adults (43 male, 56 female, mean age 7 years) were evaluated with this protocol. Each sequence was retrospectively analyzed for its utility and factors that affect its duration.
Results
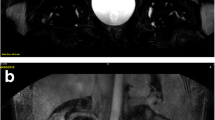
Mean scan time to perform the eight sequences, without including the variable time between sequences, was 40.5 min. Five sequences were categorized as essential: (1) sagittal T2 for planning the oblique coronal plane, (2) axial T2 with fat saturation for the assessment of corticomedullary differentiation and parenchymal thickness, (3) coronal 3-D T2 with fat saturation for multiplanar and 3-D reconstructions, (4) pre-contrast coronal T1 with fat saturation to ensure an appropriate scan prior to injecting the contrast material and (5) the coronal post-contrast dynamic series. Functional information was obtained after 8 min of dynamic imaging in the majority of children. The coronal fat-saturated T2, coronal T1, and post-contrast sagittal fat-saturated T1 sequences did not provide additional information. Because of the effects of pelvicalyceal dilation and ureteropelvic angle on the renal transit time, prone position is recommended, at least in children with high-grade pelvicalyceal dilation.
Conclusion
Comprehensive fMRU requires approximately 19 min for sequence acquisition. Allowing for time between sequences and motion correction, the total study time can be reduced to about 30 min. Four pre-contrast sequences and a shortened post-contrast dynamic scan, optimally with the child in prone position, are sufficient.





Similar content being viewed by others


References
Grattan-Smith JD, Jones RA (2006) MR urography in children. Pediatr Radiol 36:1119–1132, quiz 1228–1229
Ehammer T, Riccabona M, Maier E (2011) High resolution MR for evaluation of lower urogenital tract malformations in infants and children: feasibility and preliminary experiences. Eur J Radiol 78:388–393
Darge K, Anupindi SA, Jaramillo D (2011) MR imaging of the abdomen and pelvis in infants, children, and adolescents. Radiology 261:12–29
Khrichenko D, Darge K (2010) Functional analysis in MR urography—made simple. Pediatr Radiol 40:182–199
Rohrschneider WK, Haufe S, Wiesel M et al (2002) Functional and morphologic evaluation of congenital urinary tract dilatation by using combined static-dynamic MR urography: findings in kidneys with a single collecting system. Radiology 224:683–694
McDaniel BB, Jones RA, Scherz H et al (2005) Dynamic contrast-enhanced MR urography in the evaluation of pediatric hydronephrosis: part 2, anatomic and functional assessment of uteropelvic junction obstruction. AJR Am J Roentgenol 185:1608–1614
Perez-Brayfield MR, Kirsch AJ, Jones RA et al (2003) A prospective study comparing ultrasound, nuclear scintigraphy and dynamic contrast enhanced magnetic resonance imaging in the evaluation of hydronephrosis. J Urol 170:1330–1334
Grattan-Smith JD, Little SB, Jones RA (2008) MR urography in children: how we do it. Pediatr Radiol 38:S3–17
Fernbach SK, Maizels M, Conway JJ (1993) Ultrasound grading of hydronephrosis: introduction to the system used by the society for fetal urology. Pediatr Radiol 23:478–480
Riccabona M, Avni FE, Blickman JG et al (2008) Imaging recommendations in paediatric uroradiology: minutes of the ESPR workgroup session on urinary tract infection, fetal hydronephrosis, urinary tract ultrasonography and voiding cystourethrography, Barcelona, Spain, June 2007. Pediatr Radiol 38:138–145
Smith ADMD (2012) Smith’s textbook of endourology. Wiley-Blackwell, Chichester
Grattan-Smith JD, Little SB, Jones RA (2008) MR urography evaluation of obstructive uropathy. Pediatr Radiol 38:S49–69
Darge K, Higgins M, Hwang TJ et al (2013) Magnetic resonance and computed tomography in pediatric urology: an imaging overview for current and future daily practice. Radiol Clin North Am 51:583–598
Koff SA, Binkovitz L, Coley B et al (2005) Renal pelvis volume during diuresis in children with hydronephrosis: implications for diagnosing obstruction with diuretic renography. J Urol 174:303–307
Piepsz A (2007) Antenatally detected hydronephrosis. Sem Nucl Med 37:249–260
Koff SA (2003) The beneficial and protective effects of hydronephrosis. APMIS 2003:7–12
Cerwinka WH, Grattan-Smith JD, Jones RA et al (2014) Comparison of magnetic resonance urography to dimercaptosuccinic acid scan for the identification of renal parenchyma defects in children with vesicoureteral reflux. J Pediatr Urol 10:344–351
Fineman LD, LaBrecque MA, Shih MC et al (2006) Prone positioning can be safely performed in critically ill infants and children. Pediatr Crit Care Med 7:413–422
Kornecki A, Frndova H, Coates AL et al (2001) 4A randomized trial of prolonged prone positioning in children with acute respiratory failure. Chest 119:211–218
Mullett R, Belfield JC, Vinjamuri S (2012) Calyceal diverticulum—a mimic of different pathologies on multiple imaging modalities. J Radiol Case Rep 6:10–17
Conflicts of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Delgado, J., Bedoya, M.A., Adeb, M. et al. Optimizing functional MR urography: prime time for a 30-minutes-or-less fMRU. Pediatr Radiol 45, 1333–1343 (2015). https://doi.org/10.1007/s00247-015-3324-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-015-3324-x