
Abstract
Purpose
The aim of this study was to investigate whether performing the late cardiac 123I-metaiodobenzylguanidine (MIBG) scan earlier than 4 h post-injection (p.i.) has relevant impact on the late heart to mediastinum ratio (H/M ratio) in patients with heart failure (HF).
Methods
Forty-nine patients with HF (median left ventricular ejection fraction of 31 %, 51 % ischaemic HF) referred for cardiac 123I-MIBG scintigraphy were scanned at 15 min (early) p.i. and at 1, 2, 3 and 4 h (late) p.i. of 123I-MIBG. Late H/M ratios were calculated and evaluated using a linear mixed model with the mean late H/M ratio at 4 h p.i. as a reference. A difference in late H/M ratios of more than 0.10 between the different acquisition times in comparison with the late H/M ratio at 4 h p.i. was considered as clinically relevant.
Results
Statistically significant mean differences were observed between the late H/M ratios at 1, 2 and 3 h p.i. compared with the late H/M ratio at 4 h p.i. (0.09, 0.05 and 0.02, respectively). However, the mean differences did not exceed the cut-off value of 0.10. On an individual patient level, compared to the late H/M ratio at 4 h p.i., the late H/M ratios at 1, 2 and 3 h p.i. differed more than 0.10 in 24 (50 %), 9 (19 %) and 2 (4 %) patients, respectively.
Conclusion
Variation in acquisition time of 123I-MIBG between 2 and 4 h p.i. does not lead to a clinically significant change in the late H/M ratio. An earlier acquisition time seems to be justified and may warrant a more time-efficient cardiac 123I-MIBG imaging protocol.
Similar content being viewed by others

Introduction
Heart failure (HF) is an increasing healthcare problem in the Western world [1]. Among other features, the pathophysiology of HF is characterized by a deregulated sympathetic nervous system [2]. 123I-Metaiodobenzylguanidine (MIBG) imaging is able to visualize cardiac sympathetic innervation by providing (semi-)quantitative information on the myocardial sympathetic activity [3]. Several studies have reported that cardiac 123I-MIBG uptake provides unique information for predicting prognosis and evaluating therapeutic effects in patients with HF [4–7]. The semi-quantitative parameter that is most used to analyse cardiac 123I-MIBG uptake is the heart to mediastinum ratio (H/M ratio) of the late planar image. The reported acquisition time for this so-called late scan varies considerably, but it is recommended 4 h after injection of 123I-MIBG [8]. A shorter time interval between the injection of 123I-MIBG and the late scan reduces waiting time and may facilitate clinical use. However, only a few studies have investigated the impact of variation in acquisition time after 123I-MIBG administration on the late H/M ratio [9, 10]. Therefore, the aim of this study was to investigate whether performing the late scan earlier than 4 h post-injection (p.i.) has relevant impact on the late H/M ratio in patients with HF.
Materials and methods
Patients
Fifty patients with HF from two centres (Leiden, The Netherlands and Pisa, Italy) clinically referred for cardiac 123I-MIBG scintigraphy between 2012 and 2015 were included. The inclusion criteria were symptoms of HF, New York Heart Association functional class II–IV and age between 18 and 74 years. Patients with severe shortness of breath who were unable to lie flat for several times under a gamma camera were excluded from this study. All patients were treated according to the European Society of Cardiology guidelines for the diagnosis and management of HF and therefore received optimal pharmacological therapy, revascularization and implantable defibrillator with or without cardiac resynchronization therapy (CRT) device when appropriate [11]. The study complied with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Leiden University Medical Center. Written informed consent was obtained from all patients.
123I-MIBG data acquisition
After thyroid blockade according to the local protocol and a resting period of 30 min, 185 MBq of 123I-MIBG (AdreView, GE Healthcare, Princeton, NJ, USA) was administrated as an intravenous bolus. Afterwards, 123I-MIBG planar imaging was performed in the supine position five times p.i.; the early acquisition was performed 15 min p.i. and the late acquisitions were performed at 1, 2, 3 and 4 h p.i. Planar images were acquired in the anterior view for 10 min with dual-head gamma cameras, a Siemens e.cam (Pisa, Italy) or a Toshiba GCA-7200/PI (Leiden, The Netherlands) and stored in a 256×256 matrix. All camera heads were provided with low-energy high-resolution collimators and the images were obtained with a 15 % energy window centred at the 159 keV photopeak of 123I.
Planar 123I-MIBG image analysis
All planar 123I-MIBG images were transferred to the Leiden University Medical Center for a centralized analysis. The images were semi-quantitatively analysed by calculating the H/M ratio using dedicated post-processing software on a Syngo-MI workstation (Siemens Medical Solutions, Malvern, PA, USA). Manually a polygonal region of interest (ROI) was drawn over the myocardium including the left cavity and a rectangular ROI was placed upon the upper half of the mediastinum using the following anatomical landmarks: the lung apex as upper border, the upper cardiac border and the medial contours of the lungs. The H/M ratio was calculated by dividing the mean count density (i.e. counts/pixel) within the cardiac ROI by the mean count density in the mediastinal ROI. The washout rate was expressed as a percentage of decrease in myocardial counts between early and late planar images with correction for background and physical decay of 123I. For this calculation the following formula was used: WRBKG corrected = [(He-Me)-(Hl-Ml x123I decay correction)]/(He-Me) × 100 [8]. In this formula H represents the mean count density in the cardiac ROI and M represents the mean count density in the mediastinal ROI in the early (e) and (l) late images.
Statistical analysis
Normally distributed variables were expressed as mean ± standard deviation and non-normally distributed variables as median and interquartile range (IQR). Categorical variables were given as absolute values and percentages. Patient characteristics and 123I-MIBG scintigraphy results of subgroup analyses were compared with the independent sample t test, the Mann-Whitney U test or the chi-square test when appropriate. The late H/M ratios at 1, 2 and 3 h p.i. were compared with the late H/M ratio at 4 h p.i. with a linear mixed model with a given fixed factor time. A mean difference in late H/M ratio of more than 0.10 between the (mean) different H/M ratios at 1, 2 and 3 h p.i. and the (mean) late H/M at 4 h p.i. was considered clinically relevant. This was assessed by evaluating whether the 95 % confidence intervals (CI) for the real differences in means of the late H/M ratios at 1, 2 and 3 h p.i., respectively, compared with the late H/M ratio at 4 h p.i. included the value 0.1. In the subgroup analysis, the influence of left ventricular ejection fraction on the differences in late H/M ratios between the ischaemic and non-ischaemic HF groups at 1, 3 and 4 h p.i. was assessed by performing multivariate logistic regression analyses including H/M ratio and left ventricular ejection fraction. The washout rates between 15 min and 1, 2 and 3 h p.i. were compared with the washout rate between 15 min and 4 h p.i. with a linear mixed model with a given fixed factor time. A paired t test power analysis demonstrated that a sample size of 49 patients achieved 90 % power to reject the null hypothesis that the test and standard are equivalent, thereby assuming an absolute difference of more than 0.10 with an estimated standard deviation of 0.20 with a significance level (alpha) of 0.01670. A two-sided p value <0.05 was considered statistically significant. All analyses were performed with SPSS software (Version 22.0, SPSS IBM Corp., Armonk, NY, USA).
Results
Patients
The study population comprised 49 patients with HF, because 1 patient withdrew his informed consent after the examination. The patient characteristics of the study population are depicted in Table 1. Seventy-six per cent (37/49) of the total study population was male with a mean age of 64 ± 9 years. The aetiology of HF was ischaemic in 51 % (25/49) of the patients. Patients with ischaemic HF had a statistically significantly lower left ventricular ejection fraction compared with patients with non-ischaemic HF, 28 % (IQR 23–35) versus 33 % (IQR 29–40) (p = 0.04), respectively, and antiplatelet or oral anticoagulant therapy was more frequent at 96 % (24/25) versus 75 % (18/24) (p = 0.04), respectively.
Planar 123I-MIBG image analysis
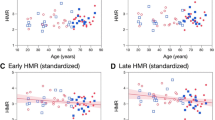
The results of the planar 123I-MIBG image analysis are shown in Table 2. Of the 49 patients, 1 patient did not have an acquisition 4 h p.i. In the total study population the late H/M ratio was 1.60 ± 0.18 at 1 h, 1.56 ± 0.19 at 2 h p.i. and 1.53 ± 0.19 at 3 h p.i. and differed all significantly from the late H/M ratio of 1.52 ± 0.20 at 4 h p.i. (p <0.001, p < 0.001 and p = 0.02, respectively). However, none of the mean differences between the late H/M ratios at 1, 2 and 3 h p.i. exceeded the predefined clinically relevant 0.10 difference with the late H/M ratio at 4 h p.i. (Fig. 1a). An example of a patient with only small differences between the late H/M ratios at 1, 2 and 3 h p.i. compared with the late H/M ratio at 4 h p.i. is depicted in Fig. 2. On an individual patient level, compared to the late H/M ratio at 4 h p.i., the late H/M ratios at 1, 2 and 3 h p.i. differed more than 0.10 in 24 (50 %), 9 (19 %) and 2 (4 %) patients, respectively (Fig. 1b).

Mean differences (a) and absolute differences (b) of each individual patient in the H/M ratios at 1, 2 and 3 h p.i. in comparison with H/M ratio at 4 h p.i. The mean difference with 95 % CI of H/M ratios of late 123I-MIBG images with acquisition at 1, 2 and 3 h p.i. in comparison with the H/M ratio of the late 123I-MIBG image at 4 h p.i. analysed with a linear mixed model (a). Each dot represents an absolute difference of each individual patient in the late H/M ratios at 1, 2 and 3 h p.i. compared with the late H/M ratio at 4 h p.i. (b). A mean difference in H/M ratio of more than 0.10 between the different acquisition times in comparison with the late H/M ratio at 4 h p.i. was considered clinically relevant

Example of a patient with ischaemic HF and planar acquisitions 1, 2, 3 and 4 h p.i., respectively
The H/M ratios of the early scan and the late scan performed at 1, 3 and 4 h p.i. were significantly higher in the non-ischaemic HF group in comparison with the ischaemic HF group (p = 0.03, p = 0.02, p = 0.03 and p = 0.03, respectively). When corrected for the left ventricular ejection fraction there was no independent association between the late H/M ratio at 1, 3 and 4 h p.i. and type of HF [odds ratio (OR) 0.09 (95 % CI 0.006–0.18), p = 0.07; OR 0.07 (95 % CI −0.027 to 0.17), p = 0.16 and OR 0.06 (95 %CI −0.03 to 0.16), p = 0.16, respectively]. Figure 3 shows the mean differences in late H/M ratios at 1, 2 and 3 h p.i. compared with the late H/M ratio at 4 h p.i. in both subgroups. Compared to the late H/M ratio at 4 h p.i., the mean late H/M ratios at 1 and 2 h p.i. were statistically significantly different in the ischaemic HF group (both p < 0.001) as well as in the non-ischaemic HF group (p < 0.001 and p = 0.005, respectively). In the non-ischaemic HF group only the mean late H/M ratio at 1 h p.i. exceeded the predefined clinically relevant 0.10 difference with the late H/M ratio 4 h p.i.

Mean differences of the late H/M ratios at 1, 2 and 3 h p.i. in comparison with the late H/M ratio at 4 h p.i. in the ischaemic HF and non-ischaemic HF subgroups. Mean difference with 95 % CI of H/M ratio of late 123I-MIBG images at 1, 2 and 3 h p.i. in comparison with H/M ratio of late 123I-MIBG image at 4 h p.i. analysed with a linear mixed model in the ischaemic HF (blue) and non-ischaemic HF (red) subgroups. A difference in H/M ratio of more than 0.10 between the different acquisition times in comparison with the late H/M ratio at 4 h was considered clinically relevant
The mean washout rate between the early scan and the late scans at 1, 2, 3 and 4 h p.i. increased from 11 ± 12 % to 21 ± 16 %, 29 ± 17 % and 34 ± 17 %. The mean washout rates between the early scan and the late scans at 1, 2 and 3 h p.i. differed all statistically significantly from the washout rate between the early and 4-h p.i. scan (all p <0.001). There was no statistically significant difference between the washout rates in the ischaemic HF and the non-ischaemic HF subgroups.
Discussion
The present study evaluated the impact of variations in acquisition time of planar 123I-MIBG scintigraphy on the late H/M ratio in patients with HF. There were statistically significant differences between the late H/M ratios at 1, 2 and 3 h p.i. compared with the late H/M ratio at 4 h p.i. However, compared with the late H/M ratio at 4 h p.i., the late H/M ratios at 1, 2 and 3 h p.i. did not exceed the predefined clinically relevant cut-off difference of 0.10.
The late H/M ratio is the most frequently used parameter to semi-quantitatively analyse the cardiac 123I-MIBG uptake in patients with HF [12]. The Cardiovascular Committee of the European Association of Nuclear Medicine and the European Council of Nuclear Cardiology recommend calculating the late H/M ratio from planar images at 4 h after receiving 123I-MIBG [8]. This recommendation is based on several studies [13–17]. First, Nakajo et al. investigated the appropriate time for cardiac radioiodine-labelled MIBG imaging [14]. This study demonstrated in rats that the accumulation of cardiac 131I-MIBG in adrenergic nerves reached a maximum plateau at 4 h p.i., while the accumulation of the tracer in other compartments rapidly decreased in a period of 6 h p.i. Second, the mechanism of myocardial uptake of 123I-MIBG in the presynaptic sympathetic nerve endings was elucidated by DeGrado et al. [15]. This group demonstrated that 123I-MIBG uptake was mainly between 1 and 7 min p.i. and depended primarily on both uptake-1 (the neuronal pathway via the norepinephrine transporter) as well as on uptake-2 (the extraneuronal pathway) activity. The clearance half-time of neuronal 123I-MIBG uptake (via uptake-1) was 112 min, in contrast to the much lower clearance half-time of extraneuronal 123I-MIBG uptake (uptake-2) of 22 min. Finally, Sisson et al. demonstrated that 123I-MIBG patterns in the heart were consistent with the concept that 123I-MIBG resides mostly in adrenergic neurons, mainly via the uptake-1 mechanism [16, 17]. This supports the hypothesis that the late H/M ratio at 4 h p.i. mainly represents the uptake, storage and release of 123I-MIBG in the myocardial vesicles at the nerve terminals, while accumulation in extraneuronal compartments is relatively low.
In the present study only small differences (≤0.10) were observed between the late H/M ratios at 1, 2 and 3 h p.i. compared with the commonly used late H/M ratio at 4 h p.i. Subgroup analysis between patients with ischaemic and non-ischaemic HF showed similar results. At the patient level, a high percentage of patients (50 %) exceeded a difference of 0.10 between the late H/M ratio at 1 h p.i. compared to the late H/M ratio at 4 h p.i. In contrast, between the late H/M ratio at 2 h p.i. and the late H/M ratio at 4 h p.i. the percentage of patients who exceeded a difference of 0.10 was much lower (19 %). In comparison with the late H/M ratios at 3 and 4 h p.i. only 4 % of the patients had a difference of more than 0.10. These results are in line with a previous investigation by Kline et al., who demonstrated a small difference in late heart to lung ratio in four healthy subjects between 1 and 2 h after administration of 74 MBq 123I-MIBG of approximately 1.3 versus 1.44 [3]. More recently, Giorgetti et al. reported the mean H/M ratios at different acquisition times in six pigs after administration of 54 ± 14 MBq 123I-MIBG using a cadmium zinc telluride camera. The mean H/M values ± SD, at 125 min, extrapolated to 176 and 240 min, were 4.33 ± 1.23 %, 3.95 ± 1.46 % and 3.63 ± 1.64 %, respectively. In addition, Okuda et al. demonstrated in 96 patients that the mean count density in the cardiac ROI and the mediastinum ROI at 3 h were highly correlated with the mean count density in the cardiac ROI and the mediastinum ROI at 4 h (r = 0.98, p < 0.0001 and r = 0.89, p < 0.0001) as well as the fact that there was only a small mean difference of 0.02 between the late H/M ratios at 3 and 4 h p.i. (1.88 ± 0.56 and 1.86 ± 0.57, respectively) [9]. Slow efflux of 123I-MIBG from the neuronal compartments can probably explain the small differences between late H/M ratios in the latter and the present study [13, 18].
The present results show that, at a group as well as at an individual patient level, the change in the late H/M ratios between 2 and 4 h p.i. is limited and probably not clinically relevant. Since the late H/M ratio has been proven to provide important information in predicting prognosis in HF patients [4], our results may have clinical implications by allowing a more flexible and/or shorter interval between the injection of 123I-MIBG and the acquisition time of the late scan for the determination of the late H/M ratio, especially in patients with HF.
With a shorter interval between the injection of 123I-MIBG and the “late” scan the washout rate will change. Previous studies have shown that the instant myocardial uptake of 123I-MIBG uptake normalized for blood pool activity is close to zero after 3 h [10]. Evaluating the washout rate at least 3 h after radiotracer injection is therefore recommended. However, Arimoto et al. demonstrated in 42 patients with HF a good correlation of the early washout rate between 5 and 15 min and the washout rate between 15 min and 3 h (r = 0.606, p < 0.0001) [19]. Moreover, the early washout rate provided prognostic information as well. In addition, Henderson et al. demonstrated that a washout rate recorded between 15 and 85 min showed a significant difference in 16 patients with non-ischaemic cardiomyopathy compared with 14 healthy volunteers: 28 ± 12 % and 6 ± 8 %, respectively (p < 0.001) [20]. Additional imaging was performed in a subset of patients (n = 8) at 4 h p.i. and 123I-MIBG retention appeared to be lower and showed greater disparity in the washout rate. In the present study, myocardial 123I-MIBG washout increased over time from 11 ± 12 % at 1 h p.i. to 34 ± 17 % at 4 h p.i. The mean washout rates between the early scan and the late scans at 1, 2 and 3 h p.i. differed all statistically significantly from the washout rate between the early and 4-h p.i. scan (all p <0.001).
Limitations
It should be addressed that although myocardial washout rates were corrected for 123I decay and mediastinal background, the myocardial washout rate can still be influenced by 123I-MIBG washout in surrounding lung and liver tissues [21]. Moreover, more research is needed before implementing the acquisition time at 2 h to avoid misclassification since the difference between the late H/M ratio at 2 h p.i. in comparison with 4 h p.i. at the patient level was not non-negligible.
Conclusion
Variation in acquisition time of 123I-MIBG between 2 and 4 h p.i. does not lead to a clinically significant change in the late H/M ratio. With the knowledge that the late H/M ratio is the best validated and most used prognostic parameter for cardiac sympathetic innervation in patients with HF, an earlier acquisition time seems to be justified and may warrant a more time-efficient cardiac 123I-MIBG imaging protocol.
References
Cowie MR, Mosterd A, Wood DA, Deckers JW, Poole-Wilson PA, Sutton GC, et al. The epidemiology of heart failure. Eur Heart J 1997;18(2):208–25.
Meredith IT, Eisenhofer G, Lambert GW, Dewar EM, Jennings GL, Esler MD. Cardiac sympathetic nervous activity in congestive heart failure. Evidence for increased neuronal norepinephrine release and preserved neuronal uptake. Circulation 1993;88(1):136–45.
Kline RC, Swanson DP, Wieland DM, Thrall JH, Gross MD, Pitt B, et al. Myocardial imaging in man with I-123 meta-iodobenzylguanidine. J Nucl Med 1981;22(2):129–32.
Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol 2010;55(20):2212–21. doi:10.1016/j.jacc.2010.01.014.
Arora R, Ferrick KJ, Nakata T, Kaplan RC, Rozengarten M, Latif F, et al. I-123 MIBG imaging and heart rate variability analysis to predict the need for an implantable cardioverter defibrillator. J Nucl Cardiol 2003;10(2):121–31. doi:10.1067/mnc.2003.2.
Kasama S, Toyama T, Kumakura H, Takayama Y, Ichikawa S, Suzuki T, et al. Spironolactone improves cardiac sympathetic nerve activity and symptoms in patients with congestive heart failure. J Nucl Med 2002;43(10):1279–85.
Boogers MJ, Borleffs CJ, Henneman MM, van Bommel RJ, van Ramshorst J, Boersma E, et al. Cardiac sympathetic denervation assessed with 123-iodine metaiodobenzylguanidine imaging predicts ventricular arrhythmias in implantable cardioverter-defibrillator patients. J Am Coll Cardiol 2010;55(24):2769–77. doi:10.1016/j.jacc.2009.12.066.
Flotats A, Carrió I, Agostini D, Le Guludec D, Marcassa C, Schäfers M, et al. Proposal for standardization of 123I-metaiodobenzylguanidine (MIBG) cardiac sympathetic imaging by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology. Eur J Nucl Med Mol Imaging 2010;37(9):1802–12. doi:10.1007/s00259-010-1491-4.
Okuda K, Nakajima K, Sugino S, Kirihara Y, Matsuo S, Taki J, et al. Development and validation of a direct-comparison method for cardiac 123I-metaiodobenzylguanidine washout rates derived from late 3-hour and 4-hour imaging. Eur J Nucl Med Mol Imaging. 2015. doi:10.1007/s00259-015-3173-8.
Giorgetti A, Burchielli S, Positano V, Kovalski G, Quaranta A, Genovesi D, et al. Dynamic 3D analysis of myocardial sympathetic innervation: an experimental study using 123I-MIBG and a CZT camera. J Nucl Med 2015;56(3):464–9. doi:10.2967/jnumed.114.143669.
McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 2012;33(14):1787–847. doi:10.1093/eurheartj/ehs104.
Verberne HJ, Brewster LM, Somsen GA, van Eck-Smit BL. Prognostic value of myocardial 123I-metaiodobenzylguanidine (MIBG) parameters in patients with heart failure: a systematic review. Eur Heart J 2008;29(9):1147–59. doi:10.1093/eurheartj/ehn113.
Nakajo M, Shimabukuro K, Miyaji N, Shimada J, Shirono K, Sakata H, et al. Rapid clearance of iodine-131 MIBG from the heart and liver of patients with adrenergic dysfunction and pheochromocytoma. J Nucl Med 1985;26(4):357–65.
Nakajo M, Shimabukuro K, Yoshimura H, Yonekura R, Nakabeppu Y, Tanoue P, et al. Iodine-131 metaiodobenzylguanidine intra- and extravesicular accumulation in the rat heart. J Nucl Med 1986;27(1):84–9.
DeGrado TR, Zalutsky MR, Vaidyanathan G. Uptake mechanisms of meta-[123I]iodobenzylguanidine in isolated rat heart. Nucl Med Biol 1995;22(1):1–12.
Sisson JC, Shapiro B, Meyers L, Mallette S, Mangner TJ, Wieland DM, et al. Metaiodobenzylguanidine to map scintigraphically the adrenergic nervous system in man. J Nucl Med 1987;28(10):1625–36.
Dae MW, De Marco T, Botvinick EH, O’Connell JW, Hattner RS, Huberty JP, et al. Scintigraphic assessment of MIBG uptake in globally denervated human and canine hearts--implications for clinical studies. J Nucl Med 1992;33(8):1444–50.
Arbab AS, Koizumi K, Takano H, Uchiyama G, Arai T, Mera K. Parameters of dynamic and static iodine-123-MIBG cardiac imaging. J Nucl Med 1995;36(6):962–8.
Arimoto T, Takeishi Y, Fukui A, Tachibana H, Nozaki N, Hirono O, et al. Dynamic 123I-MIBG SPECT reflects sympathetic nervous integrity and predicts clinical outcome in patients with chronic heart failure. Ann Nucl Med 2004;18(2):145–50.
Henderson EB, Kahn JK, Corbett JR, Jansen DE, Pippin JJ, Kulkarni P, et al. Abnormal I-123 metaiodobenzylguanidine myocardial washout and distribution may reflect myocardial adrenergic derangement in patients with congestive cardiomyopathy. Circulation 1988;78(5 Pt 1):1192–9.
Verberne HJ, Somsen GA, Povinec P, van Eck-Smit BL, Jacobson AF. Impact of mediastinal, liver and lung (123)I-metaiodobenzylguanidine ( (123)I-MIBG) washout on calculated (123)I-MIBG myocardial washout. Eur J Nucl Med Mol Imaging 2009;36(8):1322–8. doi:10.1007/s00259-009-1093-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The Department of Cardiology received research grants from Biotronik, Medtronic, Boston Scientific Corporation, St. Jude Medical, Lantheus Medical Imaging and GE Healthcare.
Conflicts of interest
None.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Dimitriu-Leen, A.C., Gimelli, A., al Younis, I. et al. The impact of acquisition time of planar cardiac 123I-MIBG imaging on the late heart to mediastinum ratio. Eur J Nucl Med Mol Imaging 43, 326–332 (2016). https://doi.org/10.1007/s00259-015-3220-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-015-3220-5