
Abstract
Introduction
The optimal surgical management of sylvian arachnoid cysts is debated. We present our experience in children who were treated endoscopically, focusing on the limits and complications of this approach.
Materials and methods
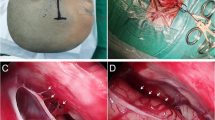
Seventeen children with a temporo-sylvian arachnoid cyst have been treated using a purely temporal endoscopic approach.
Results
In all but one case, the recognition of anatomical landmarks was obtained at the insertion of the endoscope. In one child, the orientation and opening of the basal cisterns were more difficult due to the thickness and opacity of the membranes. Nevertheless, it was possible to perform the cysto-cisternostomy endoscopically in all children with several stomies in 13. In one child, a venous bleeding occurred. There were no other intraoperative complications. There were no postoperative cerebrospinal fluid leaks. In two patients, a symptomatic subdural collection developed which required a transient subdural-peritoneal shunt. No subdural collection was noted on a delayed follow-up (mean, 23 months). Preoperative symptoms related to the mass effect exerted by the cyst resolved in all children. Two children presented a recurrence, 12 and 20 months after endoscopic surgery, respectively. At the redo-endoscopy, the stomies were found to be closed. Their reopening resulted in the disappearance of the symptoms.
Conclusions
An endoscopic approach can be used safely in the management of sylvian arachnoid cysts. An effective opening of the deep arachnoid membranes into the basal cisterns could be performed in all patients with the resolution of the preoperative symptoms. However, the long-term efficacy of the stoma needs to be assessed.



Similar content being viewed by others


References
Beems T, Grotenhuis JA (2004) Long-term complications and definition of failure of neuroendoscopic procedures. Childs Nerv Syst 20(11–12):868–877
Bright R (1831) Reports of medical cases selected with a view of illustrating the symptoms and cure of diseases by a reference to morbid anatomy. In: Longman, Rees, Orme, et al. (eds): Diseases of the brain and nervous system, vol 2. Highley, London, pp 593–660
Cappabianca P, Cinalli G, Gangemi M, Brunori A, Cavallo LM, de Divitiis E, Decq P, Delitala A, Di Rocco F, Frazee J, Godano U, Grotenhuis A, Longatti P, Mascari C, Nishihara T, Oi S, Rekate H, Schroeder HW, Souweidane MM, Spennato P, Tamburrini G, Teo C, Warf B, Zymberg ST (2008) Application of neuroendoscopy to intraventricular lesions. Neurosurgery 62(2):575–597
Cinalli G, Spennato P, Ruggiero C, Aliberti F, Trischitta V, Buonocore MC, Cianciulli E, Maggi G (2007) Complications following endoscopic intracranial procedures in children. Childs Nerv Syst 23(6):633–644
Di Rocco F, Luedemann W, Oi S (2009) Complications of neuroendoscopy. J Hydrocephalus 1(1):15–20
Di Rocco F, Yoshino M, Oi S (2005) Neuroendoscopic transventricular ventriculocystostomy in treatment for intracranial cysts. J Neurosurg. 103(1 Suppl):54–60
Donaldson JW, Edwards-Brown M, Luerssen TG (2000) Arachnoid cyst rupture with concurrent subdural hygroma. Pediatr Neurosurg 32(3):137–139
Fewel ME, Levy ML, McComb JG (1996) Surgical treatment of 95 children with 102 intracranial arachnoid cysts. Pediatr Neurosurg 25(4):165–173
Gelabert-González M, Fernández-Villa J, Cutrín-Prieto J, Garcìa Allut A, Martínez-Rumbo R (2002) Arachnoid cyst rupture with subdural hygroma: report of three cases and literature review. Childs Nerv Syst 18(11):609–613
Greenfield JP, Souweidane MM (2005) Endoscopic management of intracranial cysts. Neurosurg Focus 19(6):E7 15
Hopf NJ, Perneczky A (1998) Endoscopic neurosurgery and endoscope-assisted microneurosurgery for the treatment of intracranial cysts. Neurosurgery 43(6):1330–1336
Kabil MS, Shahinian HK (2007) Fully endoscopic supraorbital resection of congenital middle cranial fossa arachnoid cysts: report of 2 cases. Pediatr Neurosurg 43(4):316–322
Levy ML, Wang M, Aryan HE, Yoo K, Meltzer H (2003) Microsurgical keyhole approach for middle fossa arachnoid cyst fenestration. Neurosurgery 53(5):1138–1144
Oertel JM, Baldauf J, Schroeder HW, Gaab MR (2009) Endoscopic cystoventriculostomy for treatment of paraxial arachnoid cysts. J Neurosurg 110(4):792–799
Sato H, Sato N, Katayama S, Tamaki N, Matsumoto S (1991) Effective shunt-independent treatment for primary middle fossa arachnoid cyst. Childs Nerv Syst 7(7):375–381
Schroeder HW, Oertel J, Gaab MR (2004) Incidence of complications in neuroendoscopic surgery. Childs Nerv Syst 20(11–12):878–883
Tamburrini G, Caldarelli M, Massimi L, Santini P, Di Rocco C (2003) Subdural hygroma: an unwanted result of Sylvian arachnoid cyst marsupialization. Childs Nerv Syst 19(3):159–165
Tamburrini G, Dal Fabbro M, Di Rocco C (2008) Sylvian fissure arachnoid cysts: a survey on their diagnostic workout and practical management. Childs Nerv Syst 24(5):593–604
Tamburrini G, D'Angelo L, Paternoster G, Massimi L, Caldarelli M, Di Rocco C (2007) Endoscopic management of intra and paraventricular CSF cysts. Childs Nerv Syst 23(6):645–651
Zada G, Krieger MD, McNatt SA, Bowen I, McComb JG (2007) Pathogenesis and treatment of intracranial arachnoid cysts in pediatric patients younger than 2 years of age. Neurosurg Focus 22(2):E1
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Di Rocco, F., R. James, S., Roujeau, T. et al. Limits of endoscopic treatment of sylvian arachnoid cysts in children. Childs Nerv Syst 26, 155–162 (2010). https://doi.org/10.1007/s00381-009-0977-5
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-009-0977-5