
Abstract
Purpose
To evaluate the results of palliative pelvic exenteration in patients with gynecologic tumors.
Methods
A retrospective analysis was carried out in 13 patients from January 2000 to December 2007. The procedure was considered palliative because of distant metastatic disease or unresectable pelvic wall disease. Patients presented with bleeding, fistula, malodorous discharge or untreatable pain.
Result
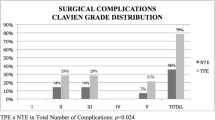
Overall complication rate was 38.4%. Mean follow-up time was 8 months. Actuarial 2 years overall survival was 15.4%. Six patients survived more than 5 months and three more than 12 months. All achieved symptoms control and favorable impact in quality of life. Two patients are with stable disease after 26 and 28 months.
Conclusions
Palliative exenteration is a procedure with high morbidity and mortality rates and should only be offered to highly selected patients. The role of exenterative surgery in relieving severe symptoms in patients with incurable disease is yet to be established.


Similar content being viewed by others


References
Höckel M, Dornhöfer N (2006) Pelvic exenteration for gynaecological tumours: achievements and unanswered questions. Lancet Oncol 7(10):837–847
Brunschwig A (1948) Complete excision of pelvic viscera for advanced carcinoma. Cancer 1:177–183
Berek JS, Howe C, Lagasse LD, Hacker NF (2005) Pelvic exenteration for recurrent gynaecologic malignancy: survival and morbidity analysis of the 45-year experience at UCLA. Gynecol Oncol 99(1):1539
Höckel M (2003) Laterally extended endopelvic resection—novel surgical treatment of locally recurrent cervical carcinoma involving the pelvic side wall. Gynecol Oncol 91:369–377
Houvenaeghel G, Moutardier V, Karsenty G, Bladou F, Lelong B, Buttarelli M et al (2004) Major complications of urinary diversion after pelvic exenteration for gynecologic malignancies: a 23-year mono-institutional experience in 124 patients. Gynecol Oncol 92:680–683
Ketcham AS, Deckers PJ, Sugarbaker EV, Hoye RC, Thomas LB, Smith RR (1970) Pelvic exenteration for carcinoma of the uterine cervix—a 15-year experience. Cancer 26(3):513–521
Lawhead RA, Clark DGC, Smith DH, Pierce VK, Lewis JL (1989) Pelvic exenteration for recurrent or persistent gynaecologic malignancies: a 10-year review of the Memorial-Sloan-Kettering Cancer Center experience (1972–1981). Gynecol Oncol 33:279–282
Magrina JF, Stanhope CR, Waever AL (1997) Pelvic exenterations: supralevator, infralevator, and with vulvectomy. Gynecol Oncol 64:130–135
Morley GW, Hopkins MP, Lindenauer SM, Roberts JA (1989) Pelvic exenteration, university of Michigan: 100 patients at 5 years. Obstet Gynecol 74:934–943
Saunders N (1995) Pelvic exenteration: by whom and for whom? Lancet 345:5–6
Sharma S, Odunsi K, Driscoll D, Lele S (2005) Pelvic exenteration for gynecological malignancies: twenty-year experience at Rosewell Park Cancer Institute. Int J Gynecol Cancer 15:475–482
Shingelton HM, Soong SJ, Gelder MS, Hatch KD, Baker VV, Austin JM (1989) Clinical and histopathologic factors predicting recurrence and survival after pelvic exenteration for cancer of the cervix. Obstet Gynecol 73:1027–1034
Stanhope CR, Symmonds RE (1985) Palliative exenteration—what, when, and why? Am J Obstet Gynecol 152:12–16
Symmonds RE, Pratt JH, Webb MJ (1975) Exenterative operations: experience with 198 patients. Am J Obstet Gynecol 121(7):907–918
Guimaraes GC, Ferreira FO, Rossi BM, Aguiar S Jr, Zequi SC, Bachega W, Nakagawa WT, Fonseca FP, Sarkis AS, Lopes A (2006) Double-barreled wet colostomy is a safe option for simultaneous urinary and fecal diversion. Analysis of 56 procedures from a single institution. J Surg Oncol 93(3):206–211
Lambrou NC, Pearson JM, Averette HE (2005) Pelvic exenteration of gynecologic malignancy: indications, and technical and reconstructive considerations. Surg Oncol Clin N Am 14:289–300
Rutledge FN, Smith JP, Wharton JT, O’Quinn AG (1977) Pelvic exenteration: analysis of 296 patients. Am J Obstet Gynecol 129:881–892
McCahill LE, Krouse R, Chu D, Juarez G, Uman G, Ferrell B et al (2002) Indications and use of palliative surgery–results of Society of Surgical Oncology survey. Ann Surg Oncol 9:104–112
Easson A (2005) Successful surgical palliation: how do we define it, and how do we measure it? Am Coll Surg 200:117–120
World Health Organization (WHO) (1990) Analgesic Ladder, Clinical Practice Guideline. No. 9, pp 41–45, http://www.who.int/cancer/palliative/en/
Hofmann B, Håheim LL, Søreide JA (2005) Ethics of palliative surgery in patients with cancer. Br J Surg 92(7):802–809
Dunn GP (2002) Surgical palliation in advanced disease: recent developments. Curr Oncol Rep 4:233–241
McCahill LE, Smith DD, Borneman T, Juarez G, Cullinane C, Chu DZJ (2003) A prospective evaluation of palliative outcomes for surgery of advanced malignancies. Ann Surg Oncol 10:654–663
Miner TJ, Jaques DP, Tavaf-Motamen H, Shriver C (1999) Decision making on surgical palliation based on patient outcome data. Am J Surg 177(2):150–154
Marnitz S, Kohler C, Muller M et al (2006) Indications for primary and secondary exenterations in patients with cervical cancer. Gynecol Oncol 103:1023–1030
Long HJ, Bundy BN, Grendys EC Jr, Benda JA, McMeekin DS, Sorosky J et al (2005) Randomized phase III trial of cisplatin with or without topotecan in carcinoma of the uterine cervix: a Gynecologic Oncology Group study. J Clin Oncol 23:4626–4633
Moore DH, Blessing JA, McQuellon RP, Thaler HT, Cella D, Benda J et al (2004) Phase III study of cisplatin with or without paclitaxel in stage IVB, recurrent, or persistent squamous cell carcinoma of the cervix: a Gynecologic Oncology Group study. J Clin Oncol 22(15):3113–3119
Tambaro R, Scambia G, DiMaio M, Pisano C, Barletta E, Iaffaioli VR, Pignata S (2004) The role of chemotherapy in locally advanced, metastatic and recurrent cervical cancer. Crit Rev Oncol Hematol 52:33–44
Tinker AV, Bhagat K, Swenerton KD, Hoskins PJ (2005) Carboplatin and paclitaxel for advanced and recurrent cervical carcinoma: the British Columbia Cancer Agency experience. Gynecol Oncol 98:54–58
Beachamp TL, Childress JF (2001) Principles of biomedical ethics. Oxford University Press, New York
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guimarães, G.C., Baiocchi, G., Ferreira, F.O. et al. Palliative pelvic exenteration for patients with gynecological malignancies. Arch Gynecol Obstet 283, 1107–1112 (2011). https://doi.org/10.1007/s00404-010-1544-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-010-1544-8