
Abstract
Background
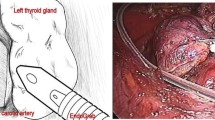
In thyroid surgery, intra-operative neuromonitoring of the recurrent laryngeal nerve (RLN) and vagal nerve (VN) are performed as an adjunct to the gold standard of optical visualisation of the RLN, to avoid injury of the RLN, and subsequently paralysis of the vocal cords. Intermittent RLN neuromonitoring diminished the temporary RLN palsy rate, but continuous neuromonitoring could have to potential of avoiding any damage. Since no study evaluated continuous vagal stimulation before, the objective of this study was to evaluate continuous neuromonitoring in a clinical setting, to assess its’ value in predicting vocal cord injury.
Methods
A single centre prospective study was performed from September 2010 till February 2012, including 100 consecutive thyroidectomies with continuous VN stimulation using an S-shaped electrode.
Results
In this study, 100 thyroidectomies (80 total thyroidectomies and 20 hemi-thyroidectomies) were analysed. On 180 nerves at risk (NAR), there were four RLN palsies (2.2 %), of which only one definitive. In the cases with temporary palsies, an intra-operative diminution of the amplitude occurred, recovering partially with release of traction. Loss of signal was seen in all four cases, with an abrupt loss of signal in the definitive one. The RLN function remained intact in the other 176 NAR.
Conclusion
Continuous neuromonitoring of the VN is accurate and precise in predicting vocal cord palsy. It is of tremendous importance that the vagal electrode is a-traumatic and gives a stable signal. The exact parameters regarding “warning signs” have yet to be determined, but amplitude changes seem to play a major role.



Similar content being viewed by others


References
Abadin SS, Kaplan EL, Angelos P (2010) Malpractice litigation after thyroid surgery: the role of recurrent laryngeal nerve injuries, 1989–2009. Surgery 148(4):718–722. doi:10.1016/j.surg.2010.07.019, discussion 722–713
Barczynski M, Konturek A, Cichon S (2009) Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg 96(3):240–246. doi:10.1002/bjs.6417
Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, Hsieh MC, Wu CW (2010) Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg 34(2):223–229. doi:10.1007/s00268-009-0316-8
Duclos A, Peix JL, Colin C, Kraimps JL, Menegaux F, Pattou F, Sebag F, Touzet S, Bourdy S, Voirin N, Lifante JC (2012) Influence of experience on performance of individual surgeons in thyroid surgery: prospective cross sectional multicentre study. BMJ 344:d8041. doi:10.1136/bmj.d8041
Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A (2008) Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg 32(7):1358–1366. doi:10.1007/s00268-008-9483-2
Snyder SK, Lairmore TC, Hendricks JC, Roberts JW (2008) Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J Am Coll Surg 206(1):123–130. doi:10.1016/j.jamcollsurg.2007.07.017
Goretzki PE, Schwarz K, Brinkmann J, Wirowski D, Lammers BJ (2010) The impact of intraoperative neuromonitoring (IONM) on surgical strategy in bilateral thyroid diseases: is it worth the effort? World J Surg 34(6):1274–1284. doi:10.1007/s00268-009-0353-3
Moskalenko V, Huller M, Gasser M, Demidchik Y, Thiede A, Timm S, Ulrichs K, Hamelmann W (2009) Investigation of the regeneration potential of the recurrent laryngeal nerve (RLN) after compression injury, using neuromonitoring. Langenbeck's Arch Surg Deutsche Gesellschaft fur Chirurgie 394(3):469–474. doi:10.1007/s00423-008-0407-2
Snyder SK, Hendricks JC (2005) Intraoperative neurophysiology testing of the recurrent laryngeal nerve: plaudits and pitfalls. Surgery 138(6):1183–1191. doi:10.1016/j.surg.2005.08.027, discussion 1191–1182
Hermann M, Alk G, Roka R, Glaser K, Freissmuth M (2002) Laryngeal recurrent nerve injury in surgery for benign thyroid diseases: effect of nerve dissection and impact of individual surgeon in more than 27,000 nerves at risk. Ann Surg 235(2):261–268
Randolph GW, Dralle H, Abdullah H, Barczynski M, Bellantone R, Brauckhoff M, Carnaille B, Cherenko S, Chiang FY, Dionigi G, Finck C, Hartl D, Kamani D, Lorenz K, Miccolli P, Mihai R, Miyauchi A, Orloff L, Perrier N, Poveda MD, Romanchishen A, Serpell J, Sitges-Serra A, Sloan T, Van Slycke S, Snyder S, Takami H, Volpi E, Woodson G (2011) Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope 121(Suppl 1):S1–S16. doi:10.1002/lary.21119
Dionigi G, Chiang FY, Rausei S, Wu CW, Boni L, Lee KW, Rovera F, Cantone G, Bacuzzi A (2010) Surgical anatomy and neurophysiology of the vagus nerve (VN) for standardised intraoperative neuromonitoring (IONM) of the inferior laryngeal nerve (ILN) during thyroidectomy. Langenbeck's Arch Surg Deutsche Gesellschaft fur Chirurgie 395(7):893–899. doi:10.1007/s00423-010-0693-3
Hermann M (2012) Schildddrüsenchirurgie. Springer-Verlag, Wien
Schneider R, Bures C, Lorenz K, Dralle H, Freissmuth M, Hermann M (2013) Evolution of nerve injury with unexpected EMG signal recovery in thyroid surgery using continuous intraoperative neuromonitoring. World J Surg 37(2):364–368. doi:10.1007/s00268-012-1853-0
Shedd DP, Burget GC (1966) Identification of the recurrent laryngeal nerve. Arch Surg 92(6):861–864
Horn D, Rotzscher VM (1999) Intraoperative electromyogram monitoring of the recurrent laryngeal nerve: experience with an intralaryngeal surface electrode. A method to reduce the risk of recurrent laryngeal nerve injury during thyroid surgery. Langenbeck's Arch Surg Deutsche Gesellschaft fur Chirurgie 384(4):392–395
Kunath M, Hussock J, Marusch F, Horschig P, Gastinger I (1999) Identifying the recurrent laryngeal nerve by intraoperative neuromonitoring. Zentralbl Chir 124(7):641–645
Thomusch O, Sekulla C, Ukkat J, Gastinger L, Lippert H, Dralle H (2001) Quality assurance study of benign and malignant goiter. Prospective multicenter data collection regarding 7,617 patients. Zentralbl Chir 126(9):664–671. doi:10.1055/s-2001-18249
Petro ML, Schweinfurth JM, Petro AB (2006) Transcricothyroid, intraoperative monitoring of the vagus nerve. Arch Otolaryngol Head Neck Surg 132(6):624–628. doi:10.1001/archotol.132.6.624
Thomusch O, Machens A, Sekulla C, Ukkat J, Lippert H, Gastinger I, Dralle H (2000) Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: prospective multicenter study in Germany. World J Surg 24(11):1335–1341
Dralle H, Sekulla C, Haerting J, Timmermann W, Neumann HJ, Kruse E, Grond S, Muhlig HP, Richter C, Voss J, Thomusch O, Lippert H, Gastinger I, Brauckhoff M, Gimm O (2004) Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 136(6):1310–1322. doi:10.1016/j.surg.2004.07.018
Lamadé W, Ulmer C, Rieber F, Friedrich C, Koch KP, Thon KP (2011) New backstrap vagus electrode for continuous intraoperative neuromonitoring in thyroid surgery. Surg Innov 18(3):206–213. doi:10.1177/1553350611409955
Acknowledgements
The authors thank Dr. Andreas Langer and Mr. Daniel Haberstroh from Dr. Langer Medical, GmbH (Waldkirch, Germany) for administrative, technical, material support and aid in extracting the data and step-by-step analysis of the signals.
Conflicts of interest
None of the authors mentioned in this study have any competing interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Van Slycke, S., Gillardin, JP., Brusselaers, N. et al. Initial experience with S-shaped electrode for continuous vagal nerve stimulation in thyroid surgery. Langenbecks Arch Surg 398, 717–722 (2013). https://doi.org/10.1007/s00423-013-1068-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-013-1068-3