
Abstract
Background
Urine uric acid (UUA) has been implicated in the pathogenesis of diabetic nephropathy via its effect on tubular cells. We hypothesized that the UUA level would be higher in adolescents with type 1 diabetes (T1D) than in those without T1D. We also hypothesized that UUA and fractional uric acid excretion (FeUA) would be higher in adolescents with T1D and hyperfiltration [estimated glomerular filtration rate (eGFR) ≥141 mL/min/1.73 m2] than in those without hyperfiltration.
Methods
The UUA concentration was determined and FeUA calculated in adolescents with (n = 239) and without T1D (n = 75). The eGFR was calculated using the Zappitelli equation based on serum creatinine and cystatin C concentrations.
Results
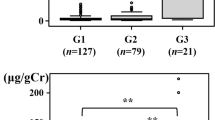
Compared to the non-diabetic adolescents enrolled in the study, those with T1D had a higher eGFR (mean ± standard deviation: 120 ± 22 vs. 112 ± 16 mL/min/1.73 m2; p = 0.0006), lower urine pH (6.2 ± 0.8 vs. 6.5 ± 1.0; p = 0.01), and higher UUA (37.7 ± 18.6 vs. 32.8 ± 18.1 mg/dL; p = 0.049) and FeUA (median [interquartile range]: 6.2 [4.3–8.7] vs. 5.2 [3.6–7.0] %; p = 0.02). Among adolescents with T1D, those with hyperfiltration had higher median FeUA (8.6 [5.2–9.9] vs. 6.0 [4.2–8.3] %; p = 0.02) than those without hyperfiltration.
Conclusions
The adolescents with T1D enrolled in the study had higher eGFR, higher UUA and more acidic urine than the non-diabetic controls, which may have increased their risk of UUA crystallization. Adolescents with T1D and hyperfiltration had higher FeUA than those without hyperfiltration. These hypothesis-generating observations may suggest a potential pathophysiologic association between uricosuria and hyperfiltration.


Similar content being viewed by others


References
Maahs DM, Rewers M (2006) Editorial: Mortality and renal disease in type 1 diabetes mellitus—progress made, more to be done. J Clin Endocrinol Metab 91:3757–3759
Orchard TJ, Secrest AM, Miller RG, Costacou T (2010) In the absence of renal disease, 20 year mortality risk in type 1 diabetes is comparable to that of the general population: a report from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetologia 53:2312–2319
Bjornstad P, Cherney D, Maahs DM (2014) Early diabetic nephropathy in type 1 diabetes: new insights. Curr Opin Endocrinol Diabetes Obes 21:279–286
Bjornstad P, Cherney DZ, Snell-Bergeon JK, Pyle L, Rewers M, Johnson RJ, Maahs DM (2015) Rapid GFR decline is associated with renal hyperfiltration and impaired GFR in adults with Type 1 diabetes. Nephrol Dial Transplant 30:1706–1711
Remuzzi G, Benigni A, Remuzzi A (2006) Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes. J Clin Invest 116:288–296
Premaratne E, Verma S, Ekinci EI, Theverkalam G, Jerums G, MacIsaac RJ (2014) The impact of hyperfiltration on the diabetic kidney. Diabetes Metab 41:5–17
Magee GM, Bilous RW, Cardwell CR, Hunter SJ, Kee F, Fogarty DG (2009) Is hyperfiltration associated with the future risk of developing diabetic nephropathy? A meta-analysis. Diabetologia 52:691–697
Bjornstad P, Maahs DM, Rivard CJ, Pyle L, Rewers M, Johnson RJ, Snell-Bergeon JK (2014) Serum uric acid predicts vascular complications in adults with type 1 diabetes: the coronary artery calcification in type 1 diabetes study. Acta Diabetol 51:783–791
Gilbert RE, Cooper ME (1999) The tubulointerstitium in progressive diabetic kidney disease: more than an aftermath of glomerular injury? Kidney Int 56:1627–1637
Ginevri F, Piccotti E, Alinovi R, DeToni T, Biagini C, Chiggeri GM, Gusmano R (1993) Reversible tubular proteinuria precedes microalbuminuria and correlates with the metabolic status in diabetic children. Pediatr Nephrol 7:23–26
Ryu ES, Kim MJ, Shin HS, Jang YH, Choi HS, Jo I, Johnson RJ, Kang DH (2013) Uric acid-induced phenotypic transition of renal tubular cells as a novel mechanism of chronic kidney disease. Am J Physiol Renal Physiol 304:F471–480
Lytvyn Y, Škrtić M, Yang GK, Yip PM, Perkins BA, Cherney DZ (2015) Glycosuria-mediated urinary uric acid excretion in patients with uncomplicated type 1 diabetes mellitus. Am J Physiol Renal Physiol 308:F77–83
Bjornstad P, Pyle L, Nguyen N, Snell-Bergeon JK, Bishop FK, Wadwa RP, Maahs DM (2015) Achieving international society for pediatric and adolescent diabetes and american diabetes association clinical guidelines offers cardiorenal protection for youth with type 1 diabetes. Pediatr Diabetes 16:22–30
Specht BJ, Wadwa RP, Snell-Bergeon JK, Nadeau KJ, Bishop FK, Maahs DM (2013) Estimated insulin sensitivity and cardiovascular disease risk factors in adolescents with and without type 1 diabetes. J Pediatr 162:297–301
Maahs DM, Prentice N, McFann K, Snell-Bergeon JK, Jalal D, Bishop FK, Aragon B, Wadwa RP (2011) Age and sex influence cystatin C in adolescents with and without type 1 diabetes. Diabetes Care 34:2360–2362
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637
Bacchetta J, Cochat P, Rognant N, Ranchin B, Hadj-Aissa A, Dubourg L (2011) Which creatinine and cystatin C equations can be reliably used in children? Clin J Am Soc Nephrol 6:552–560
Fadrowski JJ, Neu AM, Schwartz GJ, Furth SL (2011) Pediatric GFR estimating equations applied to adolescents in the general population. Clin J Am Soc Nephrol 6:1427–1435
Chiarelli F, Cipollone F, Romano F, Tumini S, Costantini F, di Ricco L, Pomilio M, Pierdomenico SD, Marini M, Cuccurullo F, Mezzetti A (2000) Increased circulating nitric oxide in young patients with type 1 diabetes and persistent microalbuminuria: relation to glomerular hyperfiltration. Diabetes 49:1258–1263
Hostetter TH, Rennke HG, Brenner BM (1982) Compensatory renal hemodynamic injury: a final common pathway of residual nephron destruction. Am J Kidney Dis 1:310–314
Hostetter TH, Rennke HG, Brenner BM (1982) The case for intrarenal hypertension in the initiation and progression of diabetic and other glomerulopathies. Am J Med 72:375–380
Roncal-Jimenez C, Garcia-Trabanino R, Barregard L, Lanaspa MA, Wesseling C, Harra T, Aragόn A, Grases F, Jarquin ER, González MA, Weiss I, Glaser J, Sánchez-Lozada LG, Johnson RJ (2015) Heat stress nephropathy from exercise-induced uric acid crystalluria: a perspective on mesoamerican nephropathy. Am J Kidney Dis. doi:10.1053/j.ajkd.2015.08.021
Cook JD, Strauss KA, Caplan YH, Lodico CP, Bush DM (2007) Urine pH: the effects of time and temperature after collection. J Anal Toxicol 31:486–496
Drummond K, Mauer M (2002) The early natural history of nephropathy in type 1 diabetes: II. Early renal structural changes in type 1 diabetes. Diabetes 51:1580–1587
Bjornstad P, Lanaspa MA, Ishimoto T, Kosugi T, Kume S, Jalal D, Maahs DM, Snell-Bergeon JK, Johnson RJ, Nakagawa T (2015) Fructose and uric acid in diabetic nephropathy. Diabetologia 58:1993–2002
Lanaspa MA, Ishimoto T, Cicerchi C, Tamura Y, Roncal-Jimenez CA, Chen W, Tanabe K, Andres-Hernando A, Orlicky DJ, Finol E, Inaba S, Li N, Rivard CJ, Kosugi T, Sanchez-Lozada LG, Petrash JM, Sautin YY, Ejaz AA, Kitagawa W, Garcia GE, Bonthron DT, Asipu A, Diggle CP, Rodriguez-Iturbe B, Nakagawa T, Johnson RJ (2014) Endogenous fructose production and fructokinase activation mediate renal injury in diabetic nephropathy. J Am Soc Nephrol 25:2526–2538
Kim SM, Choi YW, Seok HY, Jeong KH, Lee SH, Lee TW, Ihm CG, Lim SJ, Moon JY (2012) Reducing serum uric acid attenuates TGF-beta1-induced profibrogenic progression in type 2 diabetic nephropathy. Nephron Exp Nephrol 121:e109–21
Maahs DM, Caramori L, Cherney DZ, Galecki AT, Gao C, Jalal D, Perkins BA, Pop-Busui R, Rossing P, Mauer M, Doria A, PERL Consortium (2013) Uric acid lowering to prevent kidney function loss in diabetes: the preventing early renal function loss (PERL) allopurinol study. Curr Diab Rep 13:550–559
Verzola D, Ratto E, Villaggio B, Parodi EL, Pontremoli R, Garibotto G, Viazzi F (2014) Uric acid promotes apoptosis in human proximal tubule cells by oxidative stress and the activation of NADPH oxidase NOX 4. PLoS One 9:e115210
Schepers MS, van Ballegooijen ES, Bangma CH, Verkoelen CF (2005) Crystals cause acute necrotic cell death in renal proximal tubule cells, but not in collecting tubule cells. Kidney Int 68:1543–1553
Kim YG, Huang XR, Suga S, Mazzali M, Tang D, Metz C, Bucala R, Kivlighn S, Johnson RJ, Lan HY (2000) Involvement of macrophage migration inhibitory factor (MIF) in experimental uric acid nephropathy. Mol Med 6:837–848
Martinon F, Petrilli V, Mayor A, Tardivel A, Tschopp J (2006) Gout-associated uric acid crystals activate the NALP3 inflammasome. Nature 440:237–241
Ichida K, Hosoyamada M, Hisatome I, Enomoto A, Hikita M, Endou H, Hosoya T (2004) Clinical and molecular analysis of patients with renal hypouricemia in Japan-influence of URAT1 gene on urinary urate excretion. J Am Soc Nephrol 15:164–173
Zhou Y, Fang L, Jiang L, Wen P, Cao H, He W, Dai C, Yang J (2012) Uric acid induces renal inflammation via activating tubular NF-kappaB signaling pathway. PLoS One 7:e39738
Han HJ, Lim MJ, Lee YJ, Lee JH, Yang IS, Taub M (2007) Uric acid inhibits renal proximal tubule cell proliferation via at least two signaling pathways involving PKC, MAPK, cPLA2, and NF-kappaβ. Am J Physiol Renal Physiol 292:F373–381
Cirillo P, Gersch MS, Mu W, Scherer PM, Kim KM, Gesualdo L, Henderson GN, Johnson RJ, Sautin YY (2009) Ketohexokinase-dependent metabolism of fructose induces proinflammatory mediators in proximal tubular cells. J Am Soc Nephrol 20:545–553
Bouvet Y, Bouissou F, Coulais Y, Séronie-Vivien S, Tafani M, Decramer S, Chatelut E (2006) GFR is better estimated by considering both serum cystatin C and creatinine levels. Pediatr Nephrol 21:1299–306
Sharma AP, Yasin A, Garg AX, Filler G (2011) Diagnostic accuracy of cystatin C-based eGFR equations at different GFR levels in children. Clin J Am Soc Nephrol 6:1599–1608
Acknowledgments
Support for this study was provided by NIDDK grants (T32DK06387, DK075360), JDRF (11-2007-694), and CTSI UL-1 RR025780. The study was performed at the Barbara Davis Center for Childhood Diabetes, Aurora, CO. Dr. Maahs was supported by a grant from NIDDK (DK075360), Dr. Snell-Bergeon by an American Diabetes Association Junior Faculty Award (7-13-CD-10), and Dr. Wadwa by an early career award from the Juvenile Diabetes Research Foundation (11-2007-694).
Author contributions
PB researched, wrote, contributed to discussion, and reviewed/edited the manuscript; LP researched, performed the statistical analyses, contributed to the discussion, reviewed/edited the manuscript; CR researched, contributed to the discussion, reviewed/edited the manuscript; MGL researched, contributed to the discussion, reviewed/edited the manuscript; JKSB researched, contributed to the discussion, reviewed/edited the manuscript; RJJ researched, contributed to the discussion, reviewed/edited the manuscript; RPW researched, contributed to discussion, and reviewed/edited the manuscript; DMM researched, contributed to discussion, and reviewed/edited the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the Colorado Multiple Institution Review Board, and informed consent and assent (for subjects <18 years) were obtained from all subjects.
Conflict of interest disclosure
Drs. Bjornstad, Roncal, Pyle Lanaspa, Snell-Bergeon, Wadwa, and Maahs and Ms. Harra and Bishop have no conflict of interest to disclose. Dr Johnson holds a patent related to lowering uric acid in the treatment of diabetic nephropathy and has shares with XORT therapeutics.
Duality of interest
Drs. Bjornstad, Pyle and Maahs are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Rights and permissions
About this article

Cite this article
Bjornstad, P., Roncal, C., Milagres, T. et al. Hyperfiltration and uricosuria in adolescents with type 1 diabetes. Pediatr Nephrol 31, 787–793 (2016). https://doi.org/10.1007/s00467-015-3299-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-015-3299-8