
Abstract
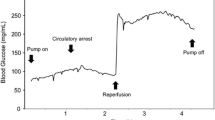
Intraoperative continuous glucose monitoring revealed that liver ischemia/reperfusion causes a rapid and profound transition in glucose concentration. We hypothesized that the washout of the glucose stored in the liver leads to a rapid transition in blood glucose concentration. Six female beagles were studied. A portosystemic shunt was established, and the glucose levels in the jugular, hepatic, and portal veins were continuously monitored. All beagles were stabilized for 30 min, and, subsequently, the hepatic artery and portal vein were clamped (the Pringle maneuver). After 30 min of warm hepatic ischemia, the clamp was removed in order to initiate hepatic reperfusion. The endpoint of the experiment was 60 min after the onset of reperfusion. The glucose levels in the abovementioned veins were recorded continuously. The glucose level in the hepatic vein increased 10 min after the start of the Pringle maneuver and was significantly higher than that in the jugular vein and portal vein just before unclamping. The glucose level in the hepatic vein peaked at 2 min after unclamping and that in the portal and jugular veins started to increase after reperfusion. The glucose level in the hepatic vein was significantly higher than that in the jugular and portal veins between 9 min after clamping and 8 min after reperfusion. In conclusion, our study among beagles showed that glucose release from the hepatic vein and sinusoid leads to a rapid elevation in systemic blood glucose levels after liver ischemia/reperfusion. This knowledge might help in the development of new strategies for blood glucose management during hepatectomy.




Similar content being viewed by others


References
Pringle JH. V. Notes on the arrest of hepatic hemorrhage due to trauma. Ann Surg. 1908;48:541–9.
Maeda H, Okabayashi T, Nishimori I, Yamashita K, Sugimoto T, Hanazaki K. Hyperglycemia during hepatic resection: continuous monitoring of blood glucose concentration. Am J Surg. 2010;199:8–13.
de Rougemont O, Lehmann K, Clavien PA. Preconditioning, organ preservation, and postconditioning to prevent ischemia-reperfusion injury to the liver. Liver Transpl. 2009;15:1172–82.
Behrends M, Martinez-Palli G, Niemann CU, Cohen S, Ramachandran R, Hirose R. Acute hyperglycemia worsens hepatic ischemia/reperfusion injury in rats. J Gastrointest Surg. 2010;14:528–35.
Ungerstedt J, Nowak G, Ungerstedt U, Ericzon BG. Microdialysis monitoring of porcine liver metabolism during warm ischemia with arterial and portal clamping. Liver Transpl. 2009;15:280–6.
Carmichael FJ, Lindop MJ, Farman JV. Anesthesia for hepatic transplantation: cardiovascular and metabolic alterations and their management. Anesth Analg. 1985;64:108–16.
Shangraw RE, Hexem JG. Glucose and potassium metabolic responses to insulin during liver transplantation. Liver Transpl Surg. 1996;2:443–54.
van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–67.
Gandhi GY, Nuttall GA, Abel MD, Mullany CJ, Schaff HV, Williams BA, Schrader LM, Rizza RA, McMahon MM. Intraoperative hyperglycemia and perioperative outcomes in cardiac surgery patients. Mayo Clin Proc. 2005;80:862–6.
Duncan AE, Abd-Elsayed A, Maheshwari A, Xu M, Soltesz E, Koch CG. Role of intraoperative and postoperative blood glucose concentrations in predicting outcomes after cardiac surgery. Anesthesiology. 2010;112:860–71.
NICE-SUGAR Study Investigators. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360:1283–97.
Hanazaki K, Maeda H, Okabayashi T. Tight perioperative glycemic control using an artificial endocrine pancreas. Surg Today. 2010;40:1–7.
Okabayashi T, Nishimori I, Yamashita K, Sugimoto T, Maeda H, Yatabe T, Kohsaki T, Kobayashi M, Hanazaki K. Continuous postoperative blood glucose monitoring and control by artificial pancreas in patients having pancreatic resection: a prospective randomized clinical trial. Arch Surg. 2009;144:933–7.
Okabayashi T, Nishimori I, Maeda H, Yamashita K, Yatabe T, Hanazaki K. Effect of intensive insulin therapy using a closed-loop glycemic control system in hepatic resection patients: a prospective randomized clinical trial. Diabetes Care. 2009;32:1425–7.
Yamashita K, Okabayashi T, Yokoyama T, Yatabe T, Maeda H, Manabe M, Hanazaki K. The accuracy of a continuous blood glucose monitor during surgery. Anesth Analg. 2008;106:160–3.
Lipshutz AK, Gropper MA. Perioperative glycemic control: an evidence-based review. Anesthesiology. 2009;110:408–21.
Nowak G, Ungerstedt J, Wernerman J, Ungerstedt U, Ericzon BG. Metabolic changes in the liver graft monitored continuously with microdialysis during liver transplantation in a pig model. Liver Transpl. 2002;8:424–32.
Kannerup AS, Funch-Jensen P, Grønbaek H, Jørgensen RL, Mortensen FV. Metabolic changes in the pig liver during warm ischemia and reperfusion measured by microdialysis. J Gastrointest Surg. 2008;12:319–26.
Imai J, Katagiri H, Yamada T, Ishigaki Y, Suzuki T, Kudo H, Uno K, Hasegawa Y, Gao J, Kaneko K, Ishihara H, Niijima A, Nakazato M, Asano T, Minokoshi Y, Oka Y. Regulation of pancreatic beta cell mass by neuronal signals from the liver. Science. 2008;322:1250–4.
Egi M, Bellomo R, Stachowski E, French CJ, Hart G. Variability of blood glucose concentration and short-term mortality in critically ill patients. Anesthesiology. 2006;105:244–52.
Acknowledgments
The Kochi University President’s Discretionary Grant.
Author information
Authors and Affiliations
Corresponding authors
Additional information
This work was performed at Kochi Medical School, Kochi, Japan.
Rights and permissions
About this article
Cite this article
Yatabe, T., Kitagawa, H., Kawano, T. et al. Continuous monitoring of glucose levels in the hepatic vein and systemic circulation during the Pringle maneuver in beagles. J Artif Organs 14, 232–237 (2011). https://doi.org/10.1007/s10047-011-0574-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10047-011-0574-8