
Abstract
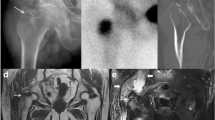
Proximal femoral fractures are frequently encountered in the emergency department (ED). Prompt diagnosis is paramount as delay will exacerbate the already poor outcomes associated with these injuries. In cases where radiography is negative but clinical suspicion remains high, magnetic resonance imaging (MRI) is the study of choice as it has the capability to depict fractures which are occult on other imaging modalities. Awareness of a particular subset of proximal femoral fractures, namely greater trochanteric fractures, is vital for both radiologists and clinicians since it has been well documented that they invariably have an intertrochanteric component which may require surgical management. The detection of intertrochanteric or cervical extension of greater trochanteric fractures has been described utilizing MRI but is underestimated with both computed tomography (CT) and bone scan. Therefore, if MRI is unavailable or contraindicated, the diagnosis of an isolated greater trochanteric fracture should be met with caution. The importance of avoiding this potential pitfall is demonstrated in the following case of an elderly woman with hip pain and CT demonstrating an isolated greater trochanteric fracture who subsequently returned to the ED with a displaced intertrochanteric fracture.





Similar content being viewed by others

References
Ahn JM, El-Khoury GY (2007) Occult fractures of extremities. Radiol Clin North Am 45(3):561–579
Cannon J, Silvestri S, Munro M (2009) Imaging choices in occult hip fracture. J Emerg Med 37(2):144–152
Lubovsky O, Liebergall M, Mattan Y, Weil Y, Mosheiff R (2005) Early diagnosis of occult hip fractures MRI versus CT scan. Injury 36(6):788–792
Feldman F, Staron RB (2004) MRI of seemingly isolated greater trochanteric fractures. AJR Am J Roentgenol 183(2):323–329
Oka M, Monu JUV (2004) Prevalence and patterns of occult hip fractures and mimics revealed by MRI. AJR Am J Roentgenol 182(2):283–288
Hommel A, Ulander K, Bjorkelund KB, Norrman PO, Wingstrand H, Thorngren KG (2008) Influence of optimised treatment of people with hip fracture on time to operation, length of hospital stay, reoperations and mortality within 1 year. Injury 39(10):1164–1174
Schultz E, Miller T, Boruchov S, Schmell EB, Toledano B (1999) Incomplete intertrochanteric fractures: imaging features and clinical management. Radiology 211(1):237–240
Craig JG, Moed BR, Eyler WR, van Holsbeeck M (2000) Fractures of the greater trochanter: intertrochanteric extension shown by MRI. Skeletal Radiol 29(10):572–576
Lee KH, Kim HM, Kim YS et al (2010) Isolated fractures of the greater trochanter with occult intertrochanteric extension. Arch Orthop Trauma Surg 130(10):1275–1280
LaLonde B, Fenton P, Campbell A, Wilson P, Yen D (2010) Immediate weight bearing in suspected isolated greater trochanteric fractures as delineated on MRI. Iowa Orthop J 30:201–204
Bryant LR, Song WS, Banks KP, Bui-Mansfield LT, Bradley YC (2008) Comparison of planar scintigraphy alone and with SPECT for the initial evaluation of femoral neck stress fracture. AJR Am J Roentgenol 191(4):1010–1015
Nicolaou S, Liang T, Murphy DT, Korzan JR, Ouellette H, Munk P (2012) Dual-energy CT: a promising new technique for assessment of the musculoskeletal system. AJR Am J Roentgenol 199:S78–S86
Alam A, Willett K, Ostlere S (2005) The MRI diagnosis and management of incomplete intertrochanteric fractures of the femur. J Bone Joint Surg 87(9):1253–1255
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reiter, M., O’Brien, S.D., Bui-Mansfield, L.T. et al. Greater trochanteric fracture with occult intertrochanteric extension. Emerg Radiol 20, 469–472 (2013). https://doi.org/10.1007/s10140-013-1117-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-013-1117-9