
Abstract
Background
Various conditions lead to the development of colonic fistulas. Contemporary surgical data is scarce and it is unclear whether advances in surgical care have impacted outcome. The aim of the present study was to review the short- and long-term outcome of patients treated surgically for colonic fistula over an 8-year period at a tertiary institution.
Methods
A retrospective review was performed, focusing on the type of operative interventions, short- and long-term complications, length of hospital stay, readmission rate, mortality rate, and fistula recurrence.
Results
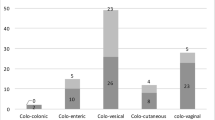
Forty-five patients were treated for colonic fistula. The most common etiology was diverticulitis (74 %). Fistula type was colovesical (58 %), colocutaneous (18 %) and colovaginal (15 %). Laparoscopic resection was performed in 42 % of cases. An intraoperative complication occurred in 4 %. A primary anastomosis was performed in 96 % of patients and 10 (23 %) had a temporary stoma. Median length of hospital stay was 6 days. Postoperative complications were common (47 %) and wound infection was noted in 20 % of patients. The readmission rate was 29 % and the 90-day mortality was 4 %. All patients healed their fistula with no recurrences noted during a median follow-up of 37 months.
Conclusions
Surgical intervention healed the majority of patients with colonic fistula. However postoperative complications were common and readmission occurred in one-third of the cases. Laparoscopic excision was feasible in nearly half of the patients.
Similar content being viewed by others


References
Woods RJ, Lavery IC, Fazio VW, Jahgelman DG, Weakley FL (1988) Internal fistulas in diverticular disease. Dis Colon Rectum 31:591–596
Lynn ET, Ranasinghe NE, Dallas KB, Divino CM (2012) Management and outcomes of colovesical fistula repair. Am Surg 78:514–518
Holroyd DJ, Banerjee S, Beavan M, Prentice R, Vijay V, Warren SJ (2012) Colovaginal and colovesical fistulae: the diagnostic paradigm. Tech Coloproctol 16:119–126
Garcea G, Majid I, Sutton CD, Pattenden CJ, Thomas WM (2006) Diagnosis and management of colovesical fistulae; six-year experience of 90 consecutive cases. Colorectal Dis 8:347–352
Najjar SF, Jamal MK, Savas JF, Miller TA (2004) The spectrum of colovesical fistula and diagnostic paradigm. Am J Surg 188:617–621
Pollard SG, Macfarlane R, Greatorex R, Everett WG, Hartfall WG (1987) Colovesical fistula. Ann R Coll Surg Engl 69:163–165
Walker KG, Anderson JH, Iskander N, McKee RF, Finlay IG (2002) Colonic resection for colovesical fistula: 5-year follow-up. Colorectal Dis 4:270–274
Driver CP, Anderson DN, Findlay K, Keenan RA, Davidson AI (1997) Vesico-colic fistulae in the Grampain region: presentation, assessment, management and outcome. J R Coll Surg Edinb 42:182–185
Wassef R, Morgan S, Tassé D, Bernard D (1983) Fistulas in diverticular disease of the colon: study of 29 cases. Can J Surg 26:546–549
Melchior S, Cudovic D, Jones J, Thomas C, Gillitzer R, Thüroff J (2009) Diagnosis and surgical management of colovesical fistulas due to sigmoid diverticulitis. J Urol 182:978–982
Leicht W, Thomas C, Thüroff J, Roos F (2012) Colovesical fistula caused by diverticulitis of the sigmoid colon: diagnosis and treatment. Urology 51:971–974 (German)
King RM, Beart RW, Mcllrath DC (1982) Colovesical and rectovesical fistulas. Arch Surg 117:680–683
Smeenk RM, Plaisier PW, van der Hoeven JA, Hesp WL (2012) Outcome of surgery for colovesical and colovaginal fistulas of diverticular origin in 40 patients. J Gastrointest Surg 16:1559–1565
Hjern F, Goldberg SM, Johansson C, Parker SC, Mellgren A (2007) Management of diverticular fistulae to the female genital tract. Colorectal Dis 9:438–442
Bahadursingh AM, Longo WE (2003) Colovaginal fistulas. Etiology and management. J Reprod Med 48:489–495
Greenstein AJ, Sachar DB, Tzakis A (1984) Course of enterovesical fistulas in Crohn’s disease. Am J Surg 17:788–792
Menenakos E, Hahnloser D, Nassiopoulos K, Chanson C, Sinclair V, Petropoulos P (2003) Laparoscopic surgery for fistulas that complicate diverticular disease. Langenbecks Arch Surg 388:189–193
Bartus CM, Lipof T, Sarwar CM et al (2005) Colovesical fistula: not a contraindication to elective laparoscopic colectomy. Dis Colon Rectum 48:233–236
Zapletal C, Woeste G, Bechstein WO, Wullstein C (2007) Laparoscopic sigmoid resections for diverticulitis complicated by abscesses or fistulas. Int J Colorectal Dis 22:1515–1521
Royds J, O’Riordan JM, Eguare E, O’Riordan D, Neary PC (2012) Laparoscopic surgery for complicated diverticular disease: a single-center experience. Colorectal Dis 14:1248–1254
Solkar MH, Forshaw MJ, Sankararajah D, Stweart M, Parker MC (2005) Colovesical fistula—is a surgical approach always justified? Colorectal Dis 7:467–471
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tam, M.S., Abbass, M., Tsay, A.T. et al. Outcome of colonic fistula surgery in the modern surgical era. Tech Coloproctol 18, 467–472 (2014). https://doi.org/10.1007/s10151-013-1085-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-013-1085-9