
Abstract
This article places social work clinicians’ compassion fatigue, burnout, and other negative consequences in a broader context of positive social work. We argue for a paradigm shift towards identifying the factors that lead clinical social workers toward human flourishing in their field. We introduce a model for creating “compassion satisfaction” or feelings of fulfillment with clients, rooted in positive psychology and expanded to incorporate the social work perspective. The model suggests that affect, work resources, and self-care influence clinicians’ positivity–negativity ratio, which in turn can result in compassion satisfaction. To maximize compassion satisfaction, research, education, and training should consider how classroom instruction and workplace policies can promote the most success among clinical social workers.
Similar content being viewed by others

Social workers are often deeply connected to their work. When asked why they entered the profession, our students most typically answer “to help others” and “to make a difference.” In helping others and making a difference, as social workers we connect and empathize with clients. Our hearts go out to those who touch us and we feel compassion. As defined in most dictionaries, compassion is a deep sense or quality of knowing or “awareness of the suffering of another coupled with the wish to relieve it” (Marriam-Webster Online Dictionary, n.d.). Compassion is also associated with feelings of condolence, pity, sympathy, empathy, and commiseration, all of which are synonymous with one another and are connected to altruism or the “unselfish concern for the welfare of others” (Marriam-Webster Online Dictionary, n.d.). In the most basic sense, clinical social workers are guided by compassion for humanity and an altruistic desire to improve individual and societal conditions.
Compassion is an essential element in effective direct social work practice. In order to help clients, we must develop rapport and empathize with the client (McCann & Pearlman, 1990). Yet, as our hearts go out to our clients through our sustained compassion, our hearts can give out from fatigue. Over a decade ago, Figley (1995) introduced compassion stress defined as the stress connected with exposure to a sufferer. Compassion fatigue is a direct result of exposure to client suffering and complicated by a lack of support in the workplace and at home (Figley, 1995). Social workers take on their clients’ problems leading to mental, physical, and emotional exhaustion and feelings of hopelessness and disconnection from others (Figley, 1993).
But when do compassion and altruistic behavior become depleting for the caregiver? Four major factors appear to contribute to compassion fatigue: poor self-care, previous unresolved trauma, inability or refusal to control work stressors, and a lack of satisfaction for the work (Figley, 1995). Together these factors explain a large part of why some clinicians get by and others do not. In preventing compassion fatigue, clinicians should detect and reinforce the sense of satisfaction of working with the suffering (Figley & Stamm, 1996). Much work over the past decade examines symptoms and consequences of compassion fatigue and ways of surviving and minimizing it. In this article, we build upon this literature to consider how feelings of compassion can benefit caregivers. How can we turn our compassion towards our clients into momentum for our own flourishing? How can social workers find “compassion satisfaction” or feelings of fulfillment with clients? When involved in their work of helping others, how can social workers reach professional fulfillment as well as personal satisfaction?
The Benefits of Clinical Social Work
To answer these questions, this article introduces a conceptual model for understanding what contributes to compassion satisfaction among clinical social workers and presents case studies to illustrate the model. We argue for a paradigm shift from an avoidance of negative consequences to an identification of what leads social workers to flourish in the field. Our goals as social workers should not be to avoid compassion stress and fatigue; instead, we must seek positive fulfillment through our work. We must treat compassion stress as potentially positive energy culminating in compassion satisfaction. Too often we focus on disorders, psychopathology, dysfunction, and problems. We must balance these negative elements with a focus on altruism, compassion, resilience, success, and thriving (Seligman, 2003; Seligman & Csikszentmihalyi, 2000).
As an alternative to compassion fatigue, we offer that if handled differently, energy from compassion stress can lead instead to a sense of flourishing. To flourish, social workers experience the joy of helping others and find satisfaction with their work. This joy and satisfaction can lead to compassion satisfaction, including a sense of fulfillment derived from seeing clients suffer less and watching them transform from the role of victim to survivor. We recognize that satisfaction is often difficult for clinicians encountering traumatic situations. Practice realities in real life situations often translate into highly destructive relationships and patterns of behavior. Although we do not have the answers to solving all of the complex realities that clinicians face, we propose that promoting satisfaction, rather than avoiding compassion fatigue, can protect them from the negative consequences of working with trauma sufferers.
The social psychology of compassion and flourishing provides a starting point to better understand compassion satisfaction. Fredrickson and Losada (2005) note that human flourishing, found among only 20% of North Americans, means to “live within an optimal range of human functioning, one that connotes goodness, generativity, growth, and resilience” (p. 678). In contrast to flourishing, human languishing is living a life that is “hollow” or “empty” (Keyes, 2002), popular among those suffering from compassion fatigue. Relative to flourishing, languishing brings more emotional distress, psychosocial impairment, limitations in daily activities, and lost work days. Applying the distinction to caregivers, flourishing is providing care within an optimal range that connotes goodness, flexibility, learning, growth, and resilience in the face of work demands. Flourishing caregivers provide highly competent and compassionate care while retaining high morale and work satisfaction.
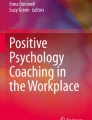
So what does predict flourishing and compassion satisfaction rather than languishing and compassion fatigue among clinical social workers? Figure 1 depicts a conceptual model for understanding the origins of compassion satisfaction and compassion fatigue. This model draws from the work of Frederickson (1998) who provides an excellent psychological perspective in understanding the critical elements in maximizing positivity, which, in turn, can maximize compassion satisfaction. Extending Frederickson’s work and adding our social work perspective, we propose a reciprocal relationship between affect and resources and introduce the importance of self-care to both affect and resources. Applied to compassion satisfaction among clinical social workers, we suggest that influenced by discernment and judgment, affect, physical, intellectual, and social resources, and self-care impact each other reciprocally. For example, positive affect promotes individual resources and resources promote positive affect. Similarly, self-care influences and is influenced by both resources and affect. Together, affect, resources, and self-care contribute to clinicians’ positivity–negativity ratio and result in the presence or absence of compassion satisfaction or compassion fatigue. The following sections detail each component of this model. We use examples from our practice with clients to illustrate the model as applied to social work practice.

Creation of compassion satisfaction or compassion fatigue
Affect
Fredrickson’s (1998) broaden-and-build theory identifies the importance of positive affect in changing one’s thoughts and resources. Affect is defined as the spectrum of valenced feeling states and attitudes. Positive affect, or positivity, includes feeling grateful and upbeat and expressing appreciation and liking. This is in contrast to negative affect or negativity, which represents feeling contemptuous or irritable and expressing disdain or disliking. Unlike negativity, which narrows people’s behavioral urges toward specific actions that are life preserving (e.g., fight, flight, reject, isolate), positivity widens the array of thoughts and actions (e.g., play, explore, cooperate, interact, greet) and generates greater flexibility and innovation. Applied to clinical social workers, positive affect provides clinicians with additional ideas and ways of intervention with clients, while negative affect and the resulting lack of innovative ideas restricts clinicians’ ability to help clients.
Exemplifying Frederickson’s broaden and build theory, Keyes and Haidt (2003) emphasize how flourishing represents a life well-lived and the importance of social benefits as opposed to individual benefits of altruistic acts. They introduce the concept of “elevation” to the vocabulary of social emotions. In direct contrast to social disgust, the feeling of elevation is triggered by witnessing acts of human moral beauty or virtue. Elevation involves a warm or glowing feeling in the chest, and makes people want to become better moral beings. Because elevation increases one’s desire to affiliate with and help others, it provides a clear illustration of Fredrickson’s (2000) broaden-and-build model of positive emotions. Positive emotions promote expanded thoughts increasing practitioners’ physical, intellectual, and social resources (Fredrickson, 1998) and providing an optimal environment for practitioners to help others.
My (MR) experience as an intake worker in a psychiatric hospital illustrates how positive affect can promote client success. I met with clients, assessed their situations and stressors, and, eventually, provided discharge planning. On one occasion, a schizophrenic client was afraid that he was “crazy” and doomed for a long stay in the hospital. He discussed his fear of voices and devils and asked me if he would be all right. As a compassionate empathizer, I felt the client’s fear, pain, and confusion; I wanted to console him and eliminate his suffering. However, I did not want to give the client false hope. As a clinician, I felt that appropriate medications should stop the voices and paranoia. Although I did not assure him of recovery, I did assure him that I was working to ensure his safety and coordinate his successful recovery. Immediately the client lightened up and was relieved. He needed to hear my confidence in his ability to overcome his thoughts. My positivity directly transferred to the client.
Resources
Positive affect can increase (and be increased by) physical, intellectual, and social resources. Fredrickson (1998) recognizes the importance of individual resources in promoting health and well-being. Positive emotions facilitate (and are facilitated by) resource-building. For McGaghie, Mytky, Brown, and Cameron (2002), resource building revolves around one’s “compassionate core” grounded in altruism. This core consists of an individual’s inner resources and capacities (i.e., thriving and resilience) and accumulated wisdom derived from life experiences. Together, inner resources and accumulated wisdom often “call” social workers to the profession and allow them to maintain career enthusiasm. The resulting reinforcement and strengthening of one’s basic compassionate core through resources and wisdom creates “a cyclic mechanism that sustains a satisfying life’s work” (McGaghie et al., 2002, p. 375). Thus, our reaction to compassion stress is a product of the interaction with our compassionate core of inner resources, accumulated wisdom, and the external world.
This interaction was borne out in an experience (MR) running a youth empowerment camp for Medicaid-eligible children. I met with children at various community centers and had no contact with other social workers. New to the profession, I did not have the accumulated wisdom in order to understand how I could help these children with complex problems nor did I have anyone who could provide ideas. New to the city, I did not have anyone to share my experiences of hearing of roach-ridden apartments, the lack of food, and drug-abusing parents. Instead of reaching out to others, my feelings of incompetence led to withdrawal. I felt compassion towards my clients, but I felt that I could not provide the material resources that the families desperately needed. I wanted to help, but I did not know how the camp’s services could address families’ fundamental needs. I lacked the inner resources to handle my clients’ suffering and I felt defeated. Exhaustion overtook me; instead of figuring out how I could help my clients best, I was counting the days to the end of the camp.
The interaction was also borne out in an experience of mine (CRF) interviewing hundreds of combat veterans as a new assistant professor. The interviews were depleting because I lacked sufficient internal resources. My compassionate core was far too under-developed. I was unable to separate the endless number of war stories in those interviews with a broader context in the external world. My passion for understanding the truth, fueled by my wish to help those suffering men grew more and more burdensome. However, once I was able to gain the wisdom of understanding how and why post-war combat stress reactions emerged and were managed, the compassion stress diminished significantly. At the same time, sensing that my work would ultimately benefit those who risked their lives for their country, my compassion satisfaction increased and positivity–negativity ratio shifted to the positive and has continued to this day.
Self-care
Although others have identified the importance of affect and resources in maximizing well-being, self-care has received less attention. Thus, from a social work perspective, we introduce the importance of self-care in influencing the positivity–negativity ratio. Self-care is a potential mechanism to increase clinicians’ positive affect and physical, intellectual, and social resources. Although there is little empirical literature regarding the role of self-care in worker retention and well-being in the social work profession, it makes sense that in order to help others we must first help ourselves.
Case studies and vignettes often emphasize the role of individual and organizational self-care in minimizing compassion fatigue (Astin, 1997; Hesse, 2002). On an individual level, therapists can take care of themselves in common ways to facilitate overall health including exercising, eating right, taking time off, and allowing time for self-reflection. Visits with friends and family, and personal psychotherapy are other mechanisms for individual self-care. Organizational self-care, alternatively, includes ways that agencies facilitate self-care, such as limiting or diversifying caseloads, and providing appropriate supervision, adequate benefits, and staff development opportunities (Hesse, 2002). Most importantly, organizations can promote a warm, friendly, and welcoming environment where clinicians feel they can depend on their colleagues in their times of need. In her work with rape survivors, for example, Astin (1997) felt that having colleagues to process what she had heard and her reactions was critical for her to meet her needs and the needs of her clients. These strategies for minimizing compassion fatigue also apply to increasing compassion satisfaction. Taking care of ourselves and reaching out to our colleagues and our clients creates an optimal environment for compassion satisfaction.
Reflecting on my (MR) experience with the youth empowerment camp, I would have benefited from appropriate self-care. Because self-care was not emphasized in my MSW coursework, I did not realize the importance of taking care of myself before seeking to help others. I did not ask the agency for supervision because clinicians emphasized their busy caseloads. Although I initially wanted to talk with other social workers about my problems and my clients’ circumstances, I felt inadequate. I also did not recognize that neglecting myself culminated in neglecting my clients.
Although my experience (MR) as a youth empowerment specialist illustrates how the lack of positive affect, resources, and self-care can lead to destruction for practitioners and clients, the presence of these features does not translate into compassion satisfaction. Instead, practitioners must use discernment and judgment to perceive and comprehend the proper response and intensity of altruistic expression. An individual who fails to discern and judge the appropriate amount of altruistic behavior in professional, social, or intimate/family situations may over- or under-respond. This can disrupt the mechanism that reinforces compassion, break the cycle, produce burnout or apathy, and lead to compassion fatigue. Astin (1997) documents the potential for this breakdown in her work. After hearing clients’ violent experiences, clinicians must fit these occurrences into their worldview and balance positive and negative perspectives of individual goodness. Thus, discernment and judgment are key features in a worker’s response to stress and consequently important attributes of social worker’s repertoire. Although affect, resources, and self-care are critical in facilitating compassion satisfaction, discernment and judgment provide critical elements in the creating the positivity ratio and compassion satisfaction.
The Positivity Ratio
This raises another issue in understanding the joys and pitfalls of compassion: how much positivity is enough to sustain the caregiver through the sadness and potential toxicity of working with the suffering? Of course, practitioners experience both positive and negative affect in varying degrees in their work. Fredrickson and Losada (2005) suggest the important role of the ratio of positive to negative affect. The positivity ratio, then, is the ratio of pleasant feelings and sentiments (or positive affect) to unpleasant ones (or negative affect) over a given period of time. Studies in various contexts confirm at least a 3 to 1 ratio theory of flourishing (Diener, 2000; Fredrickson & Losada, 2005; Gottman, 1994; Losada, 1999). Fredrickson and Losada (2005) studied two samples of college students who completed a series of tests to determine who was flourishing. Consistent with the positivity ratio hypothesis, those who were flourishing were far more likely to identify three positive experiences for every one negative experience in daily web-based reports over a 28-day period.
This positivity ratio also applies to marriages and work groups. Gottman (1994) found that conflict engagement can be healthy and produce healthy marriages, whereas expressions of disgust and contempt are corrosive. Based on twenty years of research, he concluded that unless a couple is able to maintain a high ratio of positive to negative affect (5:1), it is highly likely that they will divorce. Applied to work groups, Losada (1999) studied interpersonal dynamics among 60 business teams from behind a one-way mirror and trained coders to observe the teams who were developing their annual strategic plans. Based on teams’ high positivity ratio (5.6 to 1), Losada identified 15 “flourishing teams,” out of the 60 and correctly predicted that these teams were significantly more productive.
How does this positivity ratio apply to compassion satisfaction among social workers? The positivity ratio is especially important in the context of clinical practice because practitioners who appear predominately positive, according to broaden and build theory, are more flexible, generative, and creative in solving problems. However, their flexibility and creativity may lead to greater vulnerability when negativity is induced through their work. The positivity ratio, then, can predict when the “heart gives out” in terms of compassion. In other words, a model of altruism grounded in compassion in the social work profession suggests that when the ratio of positive experiences is sufficiently greater than the negative experiences, clinicians have higher morale and the services they deliver will be of higher quality that leads to better health care.
Thus, how can social workers maximize their positivity ratio? Even in times of elevation, clinicians’ resources are essential for their well-being. In these elevated times, clinicians may seek to help others struck by disaster and may turn compassion stress into compassion fatigue because the intoxicating joy of elevation distracted them from positive affect, their use of their own resources, and self-care. In their team approach with secondary trauma workers, Geller, Madsen, and Ohrenstein (2004) emphasize the importance of collegial support to give clinicians an opportunity to recognize both their clients’ strengths and their clients’ successes. Instead of focusing on negativity or what is not working, practitioners can shift their focus and increase their positivity ratio. Reflecting on my role in empowering youth (MR), my experience and the experience of my clients would have been enhanced if I recognized my clients’ strengths in attending camp and my success in providing a safe environment for them.
Another example of maximizing the positivity ratio is the experience of the Green Cross deployment to New York the Sunday after September 11th (Figley, Figley, & Norman, 2002). The Green Cross is a highly specialized humanitarian response organization that provides training and psychological first-aid to individuals and groups at the request of a community-based organization in the disaster zone. Green Cross deployment teams are composed of five members. Four members provide the services while the other member is designated the “Mom.” The Moms’ role is that of Compassion Fatigue Specialist (CFS). This person’s job is to attend to the physical and emotional needs of the other four members. CFS workers receive special training in helping team members to avoid compassion fatigue and embrace compassion satisfaction and self-care. At the end of each shift teams meet together, often with other teams and are lead by the CFS workers. There were six teams dispatched to New York City. The focus of the end-of-shift meetings were on the mental well-being of the team members. Much of the focus on mental well-being is not on symptoms of compassion fatigue but on compassion satisfaction. Though disappointments and sadness are not ignored, most of the time is spent focusing on the successes of the day; the sense of appreciation from the clients; the progress being made in the context of the deployment mission. This theme of success appreciation is carried out throughout the day and well-beyond the deployment when the CFS makes follow-up contact with fellow team members and talks about the successes and self care.
The Maximization of Compassion Satisfaction
Social workers inherently feel compassion because we care and we are empathic. We see the world from the point of view of the distressed. This empathy motivates altruistic behavior, which, in turn, strives to alleviate the suffering of others. Yet in the process we experience a relative degree of demand to resolve or solve the stressors causing a client’s distress. In doing so we are working with the same set of experiences—most often distressing to clients—that has a subsequent effect on ourselves. The distress is useful because it helps the social worker more fully appreciate the suffering of others and empathize with the pain (i.e., to “feel your pain”). Fortunately it is possible to modulate this distress through our consciousness and transfer this energy into satisfaction through the use of positive affect, individual resources, and self-care. This leads to greater action when working with the client to eliminate the cause of suffering, to prevent it from happening again, or to mitigate its effects. Yet, this transfer is not easy. Without the presence of positive affect, resources, and self-care, this energy can create negativity leading to compassion fatigue. Compassion fatigue sets in when our heart gives up when it continues to give and give and give. Our positivity ratio of reactions to altruistic behavior is too low.
How can we be sensitive to the plight of others and find compassion satisfaction? In other words, how can we maximize our satisfaction and flourish when our hearts go out to those who suffer? How can our hearts flourish with the burdens of the suffering? Compassion, altruism, sympathy, and empathy are critical to human survival and facilitate human flourishing. Our compassionate core requires us either to avoid negativity or to transform it. Given that empathetic practitioners will face negativity, our profession requires a constant source of inspiration that increases our positivity. Our model suggest three interrelated ways of doing so, as noted earlier: (1) increasing our positive affect or keeping a positive attitude towards clients (2) increasing our resources to manage stress, including compassion stress, and; (3) increasing self-care that comes from finding inspiration and happiness in life. With appropriate discernment and judgment, these three elements will culminate in increased positivity for practitioners leading to compassion satisfaction.
Increasing Affect
Positive affect provides essential foundation in meeting client needs in clinical practice. In short, social workers need to maintain optimism regarding their clients and their work. Although some practitioners appear inherently positive, this affect can be broadened and nurtured for all clinicians through a positive work environment. As in Astin’s (1997) experience, social workers should have the work environment and appropriate venue to discuss client issues and successes. Caseload variety increases the opportunities for practitioners to find success in their work, which in turn often leads to a more positive outlook. Appropriate time off and distance from distressing client issues also strengthens practitioners’ abilities to stay optimistic.
Increasing Resources
Intellectual, social, and physical resources are critical in maximizing compassion satisfaction. Students often enter the social work major to help people; however, they often fail to understand the importance of gaining and sustaining helping skills in the classroom. To maximize students’ intellectual resources when starting field placements, instructors need to emphasize how class concepts apply to students’ future careers and highlight how class materials, including videos, books, and lectures, can be used to answer their initial questions in their new jobs. Although most students will not absorb all material, they should understand that they can and should return to course material when the abstract class examples become real life experiences in their clinical positions. Beyond initial training, continuing education credits provide an excellent opportunity to expand practitioners’ intellectual resources.
Instructors also have the responsibility of teaching the importance of social resources and good health. Although they often teach these skills less directly, instructors should teach students the importance of reaching out to others, including friends, colleagues and supervisors. Social workers will be better practitioners inevitably when they look to others for support. In addition to fulfilling social needs, instructors must also emphasize the importance of students taking care of themselves physically. Client trauma can subsume a practitioner without appropriate preparation. Students must realize that in taking care of their physical health, they take better care of their clients. If instructors are concerned that a lack of a social network or poor physical health may influence a student’s ability to deliver competent social work services, instructors must gate-keep the profession by bringing these concerns forward to the student and appropriate authorities. Similarly, supervisors and colleagues must monitor their fellow practitioners to ensure that they are appropriately suited to serve current and future clients.
Increasing Self-care
Appropriate intellectual, social, and physical resources are not possible without adequate attention to self-care. Although psychologists have identified that positive affect and resources are fundamental to flourishing, maximizing the use of self-care among social workers warrants special attention because of the nature of the field and our work. The examination of self-care from three perspectives—teaching, clinical, and research—provides critical insight into increasing flourishing and compassion satisfaction among social work practitioners.
The Council on Social Work Education (CSWE) sets standards for field education. Among other things, all MSW students are expected to complete 180 hours in an approved internship and a field seminar covering particular content. There is, however, no classroom or internship requirement for students to learn and practice self-care. There is an assumption that the lessons of self-care will emerge; they are embedded in all practice, ethics, and field experience courses. There is no evidence, however, that this is the case. Based on even a casual review of the research literature on burnout and secondary trauma among social workers (c.f., Boscarino, Figley, & Adams, 2004), self-care is being overlooked universally by clinical social workers. The social worker educators need to do a far better job of educating social workers about the costs of caring and about the critical need for self-care throughout one’s career. Field education presents an excellent opportunity to introduce this self-care. Field instructors, for example, can set self-care as a goal on the educational contract with students specifying objectives of how the student will practice self-care. Similarly, field liaisons should discuss the importance of self-care during their field visits and contact with the student throughout the internship.
In addition to focusing on how self-care will help the student succeed, instructors must emphasize the negative consequences that their neglect of self-care will have on their clients. Social work students are often overburdened with school and work responsibilities. Often times, students feel they do not have the luxury to take a day off, exercise, or participate in extracurricular activities or groups that they find relaxing. It is predicted that when they recognize that this neglect can hurt their clients, they will give self-care a higher priority.
In addition to emphasizing self-care to social work students, agencies must contribute to their clinicians’ self-care. Treatment team meetings where individuals share experiences with troubling clients provide an opportunity to shed new light on practitioner-client situations. These meetings can also provide critical social support to clinicians. Meetings should also give practitioners the opportunity to share their successful experiences with clients. Practitioners often minimize their successes and focus on their more problematic cases. Team meetings can provide an opportunity for practitioners to highlight their success as well as share helpful techniques which can help assist future clients. In addition to treatment team meetings, clinicians must have the opportunity to debrief with colleagues and others about their own stress in working with clients. This debriefing should be considered part of the job rather than as discussions over lunch or a break. Again, as in the educational arena, self-care should be emphasized as critical not only for the success and health of the practitioner, but, also, the success of clients.
Although common sense suggests the importance of self-care, little empirical research examines how self-care influences practitioner and client well-being. With the emphasis on evidenced-based practice, empirical studies need to examine how the presence or absence of self-care contributes to worker turnover and burnout, or alternatively, compassion satisfaction. Is there a threshold of required self-care for optimal satisfaction or a linear relationship in which self-care continually increases satisfaction levels? What characteristics distinguish practitioners who practice self-care versus those who do not? Because self-care appears to increase compassion satisfaction, research is needed to better understand the mechanisms through which it works.
Increasing Positivity
The social psychology of human flourishing and the broaden-and-build model suggest that positivity is an important factor in enhancing and sustaining compassion through both personality and psychosocial education. First, given that emotions typically follow from assessments of personal meaning, we should identify factors that predispose individuals to find positive meaning. The personality traits of ego resilience (Block & Block, 1980), optimism (Scheier & Carver, 1992), hopefulness (Nunn, 1996), and happiness (Argyle, 1987) appear relevant. Individuals who possess these traits, studies have shown, tend to be the ones most likely to find positive meaning (Lyubomirsky & Lepper, 1999), experience positive emotions (Affleck & Tennen, 1996; Scheier & Carver, 1992), and evaluate self-relevant information carefully and with less defensiveness (Aspinwall, 1997; Aspinwall & Brunhart, 1996; Trope & Pomerantz, 1998), employ effective coping strategies (Aspinwall & Taylor, 1997), and experience fastest relief from distress (Folkman, 1997; Scheier et al., 2000).
Second, in addition to recognizing the role of personality, it is important to enhance positive meaning making through psychosocial education. Seligman (1994) has demonstrated how those with depression can acquire “learned optimism.” Practitioners suffering from compassion fatigue or lacking compassion satisfaction should be teachable as well. Similarly, enhancing compassion by learning to find positive meaning in dire circumstances may be another route to increasing levels of optimism and the positivity ratio. Studies have documented that finding benefit in adversity is not only predicted by preexisting levels of optimism but is also predictive of future increases in optimism (Park, Cohen, & Murch, 1996). A way of increasing optimism for social workers is increasing affect, resources, and self-care.
Conclusion
Rather than focusing on dysfunction and compassion fatigue, we introduce how clinicians faced with trauma can capitalize on compassion and energy culminating in compassion satisfaction. Increased affect, resources, and self-care can lead to a higher positivity–negativity ratio providing an optimal environment for satisfaction. We should generate research and theory on compassion enhancement and equip students with appropriate skills and perspectives that will enhance their compassionate core and self-care in addition to their skills in human relations. With appropriate attention, research will lead professional caregivers to flourish. Compassion satisfaction is not an easily attainable goal; nonetheless, clinicians can take concrete steps to reach this satisfaction improving both personal well-being and service provision for clients.
To our colleagues in the trenches every day working with the suffering, we express our sincere respect and appreciation for your work. What can we say to you based on what we have written and our collective understanding of the social psychology of compassion? Jessie Jackson’s most memorable saying was: Keep hope alive! We hope that our research and observations will remind social workers and others in direct practice that hope and optimism are as vital as self-care because they are soul care. Human service providers need to feel in the soul every day with every client that there is hope in the world and that the provided services—though perhaps small and perceived as insignificant—are important nonetheless. This sense of hope, optimism, and pride should be taught to our students as a partial antidote to compassion fatigue. Together with boundary maintenance, self-care, good training and supervision, we can be confident that your future social workers will thrive as compassionate professionals.
References
Affleck, G., & Tennen, H. (1996). Construing benefits from adversity: Adaptational significance and dispositional underpinnings. Journal of Personality, 64, 899–922.
Argyle, M. (1987). The psychology of happiness. London: Routledge.
Aspinwall, L. G. (1997). Future-oriented aspects of social comparisons: A framework for studying health-related comparison activity. In B. P. Buunk, & F. X. Gibbons (Eds.), Health, coping, and well-being: Perspectives from social comparison theory (pp. 125–165). Mahwah, NJ: Erlbaum.
Aspinwall, L. G., & Brunhart, S. M. (1996). Distinguishing optimism from denial: Optimistic beliefs predict attention to health threats. Personality & Social Psychology Bulletin, 22, 993–1003.
Aspinwall, L. G., & Taylor, S. E. (1997). A stitch in time: Self-regulation and proactive coping. Psychological Bulletin, 121, 417–436.
Astin, M. (1997). Traumatic therapy: How helping rape victims affects me as a therapist. Women & Therapy, 20, 101–109.
Block, J. H., & Block, J. (1980). The role of ego-control and ego-resiliency in the organization of behavior. In W. A. Collins (Ed.), The Minnesota symposia on child psychology, 13 (pp. 39–101). Hillsdale, NJ: Erlbaum.
Boscarino, J. A., Figley, C. R., & Adams, R. E. (2004). Evidence of compassion fatigue following the September 11 terrorist attacks: A study of secondary trauma among social workers in New York. International Journal of Emergency Mental Health, 6, 98–108.
Diener, E. (2000). Subjective well-being: The science of happiness and a proposal for a national index. American Psychologist, 55, 34–43.
Figley, C. R. (1993). Compassion stress: Toward its measurement and management. Family Therapy News, 1–2.
Figley, C. R. (Ed.) (1995). Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. New York: Brunner/Mazel.
Figley, C. R., Figley, K. R., & Norman, J. (2002). Tuesday morning September 11, 2001: The Green Cross project’s role as a case study in community-based traumatology services. Journal of Trauma Practice, 1(4), 13–36.
Figley, C. R., & Stamm, B. H. (1996). Psychometric review of compassion fatigue self test. In B. H. Stamm (Ed.), Measurement of stress, trauma and adaptation (pp. 127–128). Lutherville, MD: Sidran Press. .
Folkman, S. (1997). Positive psychological states and coping with severe stress. Social Science Medicine, 45, 1207–1221.
Fredrickson, B. L. (1998). What good are positive emotions? Review of General Psychology, 2, 300–319.
Fredrickson, B. L. (2000). Cultivating positive emotions to optimize health and well-being. Prevention & Treatment, 3. Available on the World Wide Web: http://journals.apa.org/prevention.
Fredrickson, B. L., & Losada, M. F. (2005). Positive affect and the complex dynamics of human flourishing. American Psychologist, 60, 678–686.
Geller, J., Madsen, L., & Ohrenstein, L. (2004). Secondary trauma: A team approach. Clinical Social Work Journal, 32, 415–430.
Gottman, J. M. (1994). What predicts divorce? The relationship between marital processes and marital outcomes. Hillsdale, NJ: Erlbaum.
Hesse, A. (2002). Secondary trauma: How working with trauma survivors affects therapists. Clinical Social Work Journal, 30, 293–309.
Keyes, C. L. (2002). The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior, 43, 207–222.
Keyes, C. L., & Haidt, J. (Eds.) (2003). Flourishing: Positive psychology and the life well lived. Washington DC: American Psychological Association.
Lyubomirsky, S., & Lepper, H. S. (1999). A measure of subjective happiness: Preliminary reliability and construct validation. Social Indicators Research, 46, 137–155.
Losada, M. (1999). The complex dynamics of high performance teams. Mathematical and Computer Modelling, 30(9–10), 179–192.
Marriam-Webster Online Dictionary (n.d.). Retrieved April 16, 2007, from http://www.m-w.com/
McCann, I., & Pearlman, L. (1990). Vicarious traumatization: A framework for understanding the psychological effects of working with victims. Journal of Traumatic Stress, 3(1), 131–149.
McGaghie, W. C., Mytky, J. J., Brown, W. N., & Cameron, J. R. (2002). Altruism and compassion in the health professions: A search for clarity and precision. Medical Teacher, 24, 374–378.
Nunn, K. P. (1996). Personal hopefulness: A conceptual review of the relevance of the perceived future to psychiatry. British Journal of Medical Psychology, 69, 227–245.
Park, C. L., Cohen, L. H., & Murch, R. (1996). Assessment and prediction of stress-related growth. Journal of Personality, 64, 71–105.
Scheier, M. F., & Carver, C. S. (1992). Effects of optimism on psychological and physical well-being: Theoretical overview and empirical update. Cognitive Therapy and Research, 16, 201–228.
Scheier, M. F., Matthews, K. A., Owens, J. F., Schultz, M. W., Magovern, G. J., & Carver, C. S. (2000). Optimism and rehospitalisation after coronary artery bypass graft surgery. Archives of Internal Medicine, 159, 829–843.
Seligman, M. (1994). What you can change and what you can’t. New York: Knopf.
Seligman, M. (2003). Positive psychology: Fundamental assumptions. The Psychologist, 16, 126–127.
Seligman, M., & Csikszentmihalyi, M. (2000). Positive psychology. American Psychologist, 55, 5–14.
Trope, Y., & Pomerantz, E. M. (1998). Resolving conflicts among self-evaluative motives: Positive experiences as a resource for overcoming defensiveness. Motivation and Emotion, 22, 53–72.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Radey, M., Figley, C.R. The Social Psychology of Compassion. Clin Soc Work J 35, 207–214 (2007). https://doi.org/10.1007/s10615-007-0087-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10615-007-0087-3