
Abstract
We evaluate how the productive structure and level of specialization of a hospital affect technical efficiency by analyzing a six-year panel database (2000/2005) drawn from hospital discharge records and Ministry of Health data. We adopt a distance function approach, while measuring the technical efficiency level with stochastic frontier techniques. After controlling for environmental variables and hospital case-mix, inefficiency is negatively associated with specialization and positively associated with capitalization. Capitalization is typical of private structures which, on average, use resources less efficiently with respect to public and not-for-profit hospitals. Finally, by looking at scale elasticities, we find some evidence of unexploited economies of scale, leaving room for centralization.



Similar content being viewed by others

Notes
For a good and quick review of the different nature of these structures, see (European Observatory of Health Care 2001).
A hospital is basically viewed as a human service enterprise whose primary function is the provision of diagnostic and therapeutic medical services. Production lines are specific sets of services provided to individual patients and largely coincide with an appropriate definition of treatments within each ward typology.
See for instance Rosko and Broyles (1988).
We attempted to use an index of hospital machineries as a more refined measure of capital, attaching their average costs as a weight. However the set of known costs is incomplete, and even if this missing data concerns only a couple of machines, we believe this might bias the index value. This may affect parameter estimates, as happened in most of the adopted model specifications.
Farley and Hogan (1990) made an in-depth analysis of hospital specialization measures. They proposed an Information Theory Index, where specialization is given by caseload deviation from that of the typical hospital. The main pitfall of this Information Theory Index is therefore its inability to distinguish between hospitals that treat either a very narrow or a very broad range of cases, since both will tend to have relatively high index values. Hence, we decided to make use only of the Gini ratio.
Note that each input and output variable has been standardized with its median.
Public hospitals include hospitals directly managed by ASL and AOs. Hospitals assimilated to public structures are the following: (1) “Istituto qualificato presidio della USL”; (2) “Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS)”; (3) “Ospedali classificati o assimilati ai sensi dell’art.1 u.c. L.132/68”; (4) “Policlinici Universitari”.
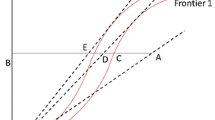
Remember that for a correct interpretation, the sign in the distance functions must be reversed. This implies that in the output distance model, the upward shift of the frontier is given by a negative sign. While for an input distance function by a positive sign.
We remind that signs and magnitudes of the cross-effects represent input/output jointness. In the input specification negative cross-output terms represent output jointness, while in the output specification positive cross-input effects imply input complementarities.
References
Alchian A, Demsetz H (1972) Production, information costs, and economic organization. Am Econ Rev 62(5):777–795
Barbetta GP, Turati G, Zago A (2007) Behavioral differences between public and private not-for-profit hospitals in the Italian national health service. Health Econ 16:75–96
Coelli T, Perelman S (2000) Technical efficiency of European railways: a distance function approach. Appl Econ 32:1967–1976
European Observatory of Health Care Systems (2001) Health care systems in transition—Italy. http://www.euro.who.int/document/e73096.pdf
Fabbri D (2003) L’efficienza tecnica e di scala degli ospedali pubblici in Italia. L’efficienza dei servizi pubblici, Banca d’Italia
Farley DE, Hogan C (1990) Case-mix specialization in the market for hospital services. Health Serv Res 25(5):757–783
Farsi M, Filippini M (2006) An analysis of efficiency and productivity in Swiss hospitals. Swiss J Econ Stat 142(1):1–37
Grassetti L, Gori E, Minotti S (2005) Multilevel flexible specification of the production function in health economics. IMA J Manage Math 16(4):383–398
Hansmann H (1996) The ownership of enterprise. Harvard University Press, Cambridge, MA
Kumbhakar SC, Lovell CA (2000) Stochastic frontier analysis. Cambridge University Press
Lovell CAK, Richardson S, Travers P, Wood LL (1994) Resources and functioning: a new view of inequality in Australia. In: Eichhorn W (ed) Models and measurement of welfare and inequality. Springer, Berlin
Milne R, Clarke A (1990) Can readmission rates be used as an outcome indicator? Br Med J 301:1139–1140
Morrison CJ, Johnston WE, Frengley G (2000) Efficiency in New Zealand sheep and beef farming: the impacts of regulatory reform. Rev Econ Stats 82:325–337
Newhouse JP (1994) Frontier estimation: how useful a tool for health economics? J Health Econ 13:317–322
Rosko M, Broyles R (1988) The economics of healthcare: a reference handbook. Greenwood Press Inc., Westport, CT
Rosko MD, Mutter RL (2008) Stochastic frontier analysis of hospital inefficiency. A review of empirical issues and an assesment of robustness. Med Care Res Rev 165(2):131–166
Shephard RW (1970) The theory of cost and production functions. Princeton University Press
Wang H (2002) Heteroscedasticity and non-monotonic efficiency effects of a stochastic frontier model. J Product Anal 18:241–253
Wang H, Schmidt P (2002) One-step and two-step estimation of the effects of exogenous variables on technical efficiency levels. J Product Anal 18:129–144
Zweifel P, Breyer F (1997) Health economics. Oxford University Press
Acknowledgements
We would like to thank: Vincenzo Atella and Federico Belotti for continuous and stimulating discussion; two anonymous referees; Giorgia Marini; the participants of the Sixteenth European Workshop on Econometrics and Health Economics and the Masterclass in applied Health Economics held in Bergen; the participants of the Econometrics PhD Students’ seminars, held at University of Rome Tor Vergata; the participants of the Technical Efficiency Parallel Session at the Third Italian Congress of Econometrics and Empirical Economics, held at University of Ancona; and Hung-Jen Wang for the assistance with his new STATA package and for his suggestions concerning convergence of the models. We also thank Cristina Tamburini from the Ministry of Health for the data used throughout the paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Daidone, S., D’Amico, F. Technical efficiency, specialization and ownership form: evidences from a pooling of Italian hospitals. J Prod Anal 32, 203–216 (2009). https://doi.org/10.1007/s11123-009-0137-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11123-009-0137-7
Keywords
- Stochastic frontiers
- Hospital discharge records
- Hospital specialization
- Distance functions
- Technical efficiency