
Abstract
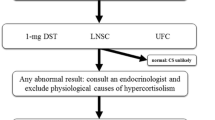
Spontaneous Cushing’s syndrome is well known but unusual clinical disorder. Many of the clinical features (central weight gain, glucose intolerance, hypertension, muscle weakness) are seen in other common conditions. Recognition of patients with multiple features, features unusual for their age (i.e. early onset osteoporosis or hypertension), patients with features more specific to Cushing’s syndrome (i.e. easy bruising, facial plethora, and violaceous striae), and patients with incidental adrenal mass or polycystic ovary syndrome should prompt an evaluation for cortisol excess. Late-night salivary cortisol, 1 mg overnight dexamethasone suppression testing, or 24 h urine free cortisol determination have excellent diagnostic characteristics and should be obtain in patients with suspected Cushing’ syndrome. If this initial testing is abnormal, further evaluation should be directed by an endocrinologist experienced in the diagnosis and differential diagnosis of Cushing’ syndrome.

Similar content being viewed by others


References
Swearingen B, Biller BM, Barker 2nd FG, et al. Long-term mortality after transsphenoidal surgery for Cushing disease. Ann Intern Med. 1999;130:821–4.
Nieman LK, Biller BM, Findling JW, et al. The diagnosis of Cushing’s syndrome: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2008;93:1526–40.
Etxabe J, Vazquez JA. Morbidity and mortality in Cushing’s disease: an epidemiological approach. Clin Endocrinol (Oxf). 1994;40:479–84.
Lindholm J, Juul S, Jorgensen JO, et al. Incidence and late prognosis of cushing’s syndrome: a population-based study. J Clin Endocrinol Metab. 2001;86:117–23.
Anderson Jr GH, Blakeman N, Streeten DH. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens. 1994;12:609–15.
Omura M, Saito J, Yamaguchi K, et al. Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens Res. 2004;27:193–202.
Reincke M, Nieke J, Krestin GP, et al. Preclinical Cushing’s syndrome in adrenal “incidentalomas”: comparison with adrenal Cushing’s syndrome. J Clin Endocrinol Metab. 1992;75:826–32.
Terzolo M, Pia A, Ali A, et al. Adrenal incidentaloma: a new cause of the metabolic syndrome? J Clin Endocrinol Metab. 2002;87:998–1003.
Catargi B, Rigalleau V, Poussin A, et al. Occult Cushing’s syndrome in type-2 diabetes. J Clin Endocrinol Metab. 2003;88:5808–13.
Leibowitz G, Tsur A, Chayen SD, et al. Pre-clinical Cushing’s syndrome: an unexpected frequent cause of poor glycaemic control in obese diabetic patients. Clin Endocrinol (Oxf). 1996;44:717–22.
Chiodini I, Mascia ML, Muscarella S, et al. Subclinical hypercortisolism among outpatients referred for osteoporosis. Ann Intern Med. 2007;147:541–8.
Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’s syndrome. Lancet. 2006;367:1605–17.
Kelly W. Exophthalmos in Cushing’s syndrome. Clin Endocrinol (Oxf). 1996;45:167–70.
Bouzas EA, Mastorakos G, Chrousos GP, Kaiser-Kupfer MI. Lisch nodules in Cushing’s disease. Arch Ophthalmol. 1993;111:439–40.
Bouzas EA, Scott MH, Mastorakos G, et al. Central serous chorioretinopathy in endogenous hypercortisolism. Arch Ophthalmol. 1993;111:1229–33.
Bourdeau I, Bard C, Forget H, et al. Cognitive function and cerebral assessment in patients who have Cushing's syndrome. Endocrinol Metab Clin North Am. 2005;34:357. 69, ix.
Raff H, Findling JW. A physiologic approach to diagnosis of the Cushing syndrome. Ann Intern Med. 2003;138:980–91.
RP DOE, JA VENNES, EB FLINK. Diurnal variation of 17-hydroxycorticosteroids, sodium, potassium, magnesium and creatinine in normal subjects and in cases of treated adrenal insufficiency and Cushing’s syndrome. J Clin Endocrinol Metab. 1960;20:253–65.
Glass AR, Zavadil 3rd AP, Halberg F, et al. Circadian rhythm of serum cortisol in Cushing’s disease. J Clin Endocrinol Metab. 1984;59:161–5.
Refetoff S, Van Cauter E, Fang VS, et al. The effect of dexamethasone on the 24-hour profiles of adrenocorticotropin and cortisol in Cushing’s syndrome. J Clin Endocrinol Metab. 1985;60:527–35.
Bolufer P, Gandia A, Rodriguez A, Antonio P. Salivary corticosteroids in the study of adrenal function. Clin Chim Acta. 1989;183:217–25.
Kahn JP, Rubinow DR, Davis CL, et al. Salivary cortisol: a practical method for evaluation of adrenal function. Biol Psychiatry. 1988;23:335–49.
Reid JD, Intrieri RC, Susman EJ, Beard JL. The relationship of serum and salivary cortisol in a sample of healthy elderly. J Gerontol. 1992;47:P176–9.
Read GF, Walker RF, Wilson DW, Griffiths K. Steroid analysis in saliva for the assessment of endocrine function. Ann N Y Acad Sci. 1990;595:260–74.
Carroll T, Raff H, Findling JW. Late-night salivary cortisol measurement in the diagnosis of Cushing’s syndrome. Nat Clin Pract Endocrinol Metab. 2008;4:344–50.
Elamin MB, Murad MH, Mullan R, et al. Accuracy of diagnostic tests for Cushing’s syndrome: a systematic review and metaanalyses. J Clin Endocrinol Metab. 2008;93:1553–62.
Keller J, Flores B, Gomez RG, et al. Cortisol circadian rhythm alterations in psychotic major depression. Biol Psychiatry. 2006;60:275–81.
Carroll BJ, Cassidy F, Naftolowitz D, et al. Pathophysiology of hypercortisolism in depression. Acta Psychiatr Scand Suppl. 2007;115:90–103.
Jones NM, Holzman CB, Zanella AJ, et al. Assessing mid-trimester salivary cortisol levels across three consecutive days in pregnant women using an at-home collection protocol. Paediatr Perinat Epidemiol. 2006;20:425–37.
Carr BR, Parker Jr CR, Madden JD, et al. Maternal plasma adrenocorticotropin and cortisol relationships throughout human pregnancy. Am J Obstet Gynecol. 1981;139:416–22.
Newell-Price J, Trainer P, Besser M, Grossman A. The diagnosis and differential diagnosis of Cushing’s syndrome and pseudo-Cushing’s states. Endocr Rev. 1998;19:647–72.
Gorges R, Knappe G, Gerl H, et al. Diagnosis of Cushing’s syndrome: re-evaluation of midnight plasma cortisol vs urinary free cortisol and low-dose dexamethasone suppression test in a large patient group. J Endocrinol Invest. 1999;22:241–9.
Findling JW, Raff H, Aron DC. The low-dose dexamethasone suppression test: a reevaluation in patients with Cushing’s syndrome. J Clin Endocrinol Metab. 2004;89:1222–6.
Wood PJ, Barth JH, Freedman DB, et al. Evidence for the low dose dexamethasone suppression test to screen for Cushing’s syndrome–recommendations for a protocol for biochemistry laboratories. Ann Clin Biochem. 1997;34(Pt 3):222–9.
Kyriazopoulou V, Vagenakis AG. Abnormal overnight dexamethasone suppression test in subjects receiving rifampicin therapy. J Clin Endocrinol Metab. 1992;75:315–7.
Castro M, Elias PC, Quidute AR, et al. Out-patient screening for Cushing’s syndrome: the sensitivity of the combination of circadian rhythm and overnight dexamethasone suppression salivary cortisol tests. J Clin Endocrinol Metab. 1999;84:878–82.
Yaneva M, Mosnier-Pudar H, Dugue MA, et al. Midnight salivary cortisol for the initial diagnosis of Cushing’s syndrome of various causes. J Clin Endocrinol Metab. 2004;89:3345–51.
Papanicolaou DA, Yanovski JA, Cutler Jr GB, et al. A single midnight serum cortisol measurement distinguishes Cushing’s syndrome from pseudo-Cushing states. J Clin Endocrinol Metab. 1998;83:1163–7.
Papanicolaou DA, Mullen N, Kyrou I, Nieman LK. Nighttime salivary cortisol: a useful test for the diagnosis of Cushing’s syndrome. J Clin Endocrinol Metab. 2002;87:4515–21.
Meikle AW, Findling J, Kushnir MM, et al. Pseudo-Cushing syndrome caused by fenofibrate interference with urinary cortisol assayed by high-performance liquid chromatography. J Clin Endocrinol Metab. 2003;88:3521–4.
Findling JW, Pinkstaff SM, Shaker JL, et al. Pseudohypercortisoluria: spurious elevation of urinary cortisol due to carbamazepine. Endocrinologist. 1998;8:51.
Masserini B, Morelli V, Bergamaschi S, et al. The limited role of midnight salivary cortisol levels in the diagnosis of subclinical hypercortisolism in patients with adrenal incidentaloma. Eur J Endocrinol. 2009;160:87–92.
Nunes ML, Vattaut S, Corcuff JB, et al. Late-night salivary cortisol for diagnosis of overt and subclinical Cushing’s syndrome in hospitalized and ambulatory patients. J Clin Endocrinol Metab. 2009;94:456–62.
Reimondo G, Allasino B, Bovio S, et al. Evaluation of the effectiveness of midnight serum cortisol in the diagnostic procedures for Cushing’s syndrome. Eur J Endocrinol. 2005;153:803–9.
Patil CG, Prevedello DM, Lad SP, et al. Late recurrences of Cushing’s disease after initial successful transsphenoidal surgery. J Clin Endocrinol Metab. 2008;93:358–62.
Toms GC, McCarthy MI, Niven MJ, et al. Predicting relapse after transsphenoidal surgery for Cushing’s disease. J Clin Endocrinol Metab. 1993;76:291–4.
Trainer PJ, Lawrie HS, Verhelst J, et al. Transsphenoidal resection in Cushing’s disease: undetectable serum cortisol as the definition of successful treatment. Clin Endocrinol (Oxf). 1993;38:73–8.
Losa M, Bianchi R, Barzaghi R, et al. Persistent adrenocorticotropin response to desmopressin in the early postoperative period predicts recurrence of Cushing’s disease. J Clin Endocrinol Metab. 2009;94:3322–8.
Romanholi DJ, Machado MC, Pereira CC, et al. Role for postoperative cortisol response to desmopressin in predicting the risk for recurrent Cushing’s disease. Clin Endocrinol (Oxf). 2008;69:117–22.
Carrasco CA, Coste J, Guignat L et al (2008) Midnight Salivary Cortisol Determination for Assessing the Outcome of Transsphenoidal Surgery in Cushing’s Disease. J Clin Endocrinol Metab
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carroll, T.B., Findling, J.W. The diagnosis of Cushing’s syndrome. Rev Endocr Metab Disord 11, 147–153 (2010). https://doi.org/10.1007/s11154-010-9143-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11154-010-9143-3