
Abstract
Background
Despite the laparoscopic approach, patients can suffer moderate to severe pain following bariatric surgery. This randomized controlled double-blinded trial investigated the analgesic efficacy of ultrasound-guided transversus abdominis plane (TAP) blocks for laparoscopic gastric-bypass surgery.
Methods
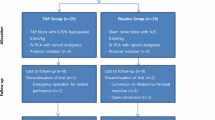
Seventy patients undergoing laparoscopic gastric-bypass surgery were randomized to receive either bilateral ultrasound-guided subcostal TAP block injections after induction of general anesthesia or none. All patients received trocar insertion site local anesthetic infiltration and systemic analgesia. The primary outcome was cumulative opioid consumption (IV morphine equivalent) during the first 24 h postoperatively. Interval opioid consumption, pain severity scores, rates of nausea or vomiting, and rates of pruritus were measured during phase I recovery, and at 24 and 48 h postoperatively.
Results
There was no difference in cumulative opioid consumption during the first 24 h postoperatively between the TAP (32.2 mg [95% CI, 27.6–36.7]) and control (35.6 mg [95% CI, 28.6–42.5]; P = 0.41) groups. Postoperative opioid consumptions during phase I recovery and the 24–48-h interval were similar between groups, as were pain scores at rest and with movement during all measured intervals. The rates of nausea or vomiting and pruritus were equivalent.
Conclusions
Bilateral TAP blocks do not provide additional analgesic benefit when added to trocar insertion site local anesthetic infiltration and systemic analgesia for laparoscopic gastric-bypass surgery.



Similar content being viewed by others


References
Schumann R. Anaesthesia for bariatric surgery. Best Pract Res Clin Anaesthesiol. 2011;25:83–93.
Tufanogullari B, White PF, Peixoto MP, et al. Dexmedetomidine infusion during laparoscopic bariatric surgery: the effect on recovery outcome variables. Anesth Analg. 2008;106:1741–8.
Benumof JL. Obesity, sleep apnea, the airway and anesthesia. Curr Opin Anaesthesiol. 2004;17:21–30.
El-Dawlatly AA, Turkistani A, Kettner SC, et al. Ultrasound-guided transversus abdominis plane block: description of a new technique and comparison with conventional systemic analgesia during laparoscopic cholecystectomy. Br J Anaesth. 2009;102:763–7.
Ra YS, Kim CH, Lee GY, et al. The analgesic effect of the ultrasound-guided transverse abdominis plane block after laparoscopic cholecystectomy. Korean J Anesthesiol. 2010;58:362–8.
Niraj G, Searle A, Mathews M, et al. Analgesic efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing open appendicectomy. Br J Anaesth. 2009;103:601–5.
Belavy D, Cowlishaw PJ, Howes M, et al. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br J Anaesth. 2009;103:726–30.
Abdallah FW, Chan VW, Brull R. Transversus abdominis plane block: a systematic review. Reg Anesth Pain Med. 2012;37:193–209.
Hebbard PD, Barrington MJ, Vasey C. Ultrasound-guided continuous oblique subcostal transversus abdominis plane blockade: description of anatomy and clinical technique. Reg Anesth Pain Med. 2010;35:436–41.
Skaer TL. Practice guidelines for transdermal opioids in malignant pain. Drugs. 2004;64:2629–38.
Sites BD, Neal JM. Placebo or intervention? Is it all a sham? Anaesthesia. 2011;66:73–5.
Jarman J, Marks N, Fahy CJ, et al. Anaesthetists’ risk assessment of placebo nerve block studies using the SHAM (Serious Harm and Morbidity) scale. Anaesthesia. 2012;67:361–6.
Sandeman DJ, Bennett M, Dilley AV, et al. Ultrasound-guided transversus abdominis plane blocks for laparoscopic appendicectomy in children: a prospective randomized trial. Br J Anaesth. 2011;106:882–6.
Ortiz J, Suliburk JW, Wu K, et al. Bilateral transversus abdominis plane block does not decrease postoperative pain after laparoscopic cholecystectomy when compared with local anesthetic infiltration of trocar insertion sites. Reg Anesth Pain Med. 2012;37:188–92.
Barrington MJ, Ivanusic JJ, Rozen WM, et al. Spread of injectate after ultrasound-guided subcostal transversus abdominis plane block: a cadaveric study. Anaesthesia. 2009;64:745–50.
Griffiths JD, Barron FA, Grant S, et al. Plasma ropivacaine concentrations after ultrasound-guided transversus abdominis plane block. Br J Anaesth. 2010;105:853–6.
Torup H, Mitchell AU, Breindahl T, et al. Potentially toxic concentrations in blood of total ropivacaine after bilateral transversus abdominis plane blocks; a pharmacokinetic study. Eur J Anaesthesiol. 2012;29:235–8.
Latzke D, Marhofer P, Kettner SC, et al. Pharmacokinetics of the local anesthetic ropivacaine after transversus abdominis plane block in healthy volunteers. Eur J Clin Pharmacol. 2012;68:419–25.
Borglum J, Jensen K, Christensen AF, et al. Distribution patterns, dermatomal anesthesia, and ropivacaine serum concentrations after bilateral dual transversus abdominis plane block. Reg Anesth Pain Med. 2012;37:294–301.
Acknowledgments
Dr. Richard Brull is supported by the Merit Award Program, Department of Anesthesia, University of Toronto. Equipment support for research was provided from BK Medical, Philips Healthcare and SonoSite.
Conflict of Interest
Dr. Eric Albrecht has received grants from the “Swiss Academy for Anaesthesia Research” (SACAR), Lausanne, Switzerland (no grant numbers attributed). None of the other authors report any conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Albrecht, E., Kirkham, K.R., Endersby, R.V.W. et al. Ultrasound-Guided Transversus Abdominis Plane (TAP) Block for Laparoscopic Gastric-Bypass Surgery:a Prospective Randomized Controlled Double-Blinded Trial. OBES SURG 23, 1309–1314 (2013). https://doi.org/10.1007/s11695-013-0958-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-013-0958-3