
Abstract
Previous research suggests that insecurely attached individuals may, in some cases, have a higher risk of developing negative health symptoms than securely attached ones. We conducted two studies (Study 1, n = 191; Study 2, n = 216) aimed at broadening this finding. We analysed the relationships between two distinct dimensions of insecure attachment (anxious and avoidant) and several classes of negative physical and mental health symptoms. Additionally, we placed emotion regulation difficulties in the role of potential mediator of these relationships. Our results indicated that both anxious and avoidant attachment were positively related to health symptoms on the level of bivariate correlations. However, when both of them were controlled within one mediation model, it was only attachment anxiety, and not attachment avoidance, that proved to be a significant, positive predictor of most health symptom classes: vegetative, agoraphobic, social phobia symptoms and global symptom severity index (which reflects a broad range of negative health symptoms). These relationships were indeed mediated by emotion regulation difficulties. Our results support the notion that (1) different dimensions of insecure attachment can have differential consequences for physical and mental health, and (2) emotion regulation can be one of the mechanisms that explain the links between attachment and health.
Similar content being viewed by others


Introduction
It seems that strong social support and an ability to form healthy and stable relationships can have far reaching benefits for quality of life, psychological and physical health and wellbeing (e.g., Cohen and Janicki-Deverts 2009; Holt-Lunstad et al. 2010; Uchino 2006). In fact, forming and sustaining social ties that are safe and satisfying seem to be a basic human desire. Deprivation of this need, especially in early childhood, can influence the way people function in relationships in their adult life, and can contribute to creating adult insecure attachment patterns (e.g., Bartholomew 1993; Bowlby 1982; Fraley and Shaver 2000). On the basis of several decades of research, researchers have created various classifications of insecure attachment. One such classification that is most visible in the literature is the division into anxious (or anxious-ambivalent) and avoidant attachment (Brennan et al. 1998). Although both of these behavioral tendencies are referred to as “insecure” attachment, they predict a fairly distinct pattern of behaviors both in the domain of close relationships, and beyond this domain (Harms 2011; Li and Chan 2012; Mickelson et al. 1997).
Anxiously attached individuals are characterized by pervasive feelings of nervousness or unease about their close relationships, may be more focused on the threat of a partner leaving them, can react more negatively in the case of negative events in a relationship, and are prone to experiencing more feelings of worry and unworthiness (Feeney and Noller 1996; Fraley and Shaver 2000; Li and Chan 2012). Because of a smaller tolerance of ambiguity in relationship situations, they can require higher commitment from their partner, be more sensitive to signals of lack of commitment and have a higher tendency to react with negative emotions in such cases. On the other hand, avoidant individuals are characterized by a tendency to disengage in situations of close relationships, experience feelings of discomfort when depending on others, avoidance of intimacy and high preference for self-reliance. An avoidant attachment is also associated with attributing less value to social support and social relations in general (e.g., Edelstein and Shaver 2004; Feeney and Noller 1996; Li and Chan 2012). Both of these attachment patterns develop as a response to early-life feelings of rejection or high unpredictability and unreliability in the child-parent relationship (e.g., Bartholomew 1993; Egeland and Sroufe 1981; Fraley and Shaver 2000).
Previous research has shown that attachment can influence health and health behavior (Feeney 2000; Maunder and Hunter 2001; Pietromonaco et al. 2015). For example, West et al. (1986) suggested that insecure (i.e., anxious and avoidant) attachment can lead to health problems through three different mechanisms. Specifically, insecure attachment may: (a) give rise to nonspecific vulnerability to stress, which – in turn – can predispose individuals to experiencing health symptoms; (b) negatively influence one’s ability to effectively form and utilize social support networks, which decreases availability of support; (c) affect the way individuals appraise and react to life events. This model has received empirical support through the years of research on this topic (e.g., Feeney 2000; Maunder and Hunter 2001; Pietromonaco et al. 2013). Additionally, previous research has indicated that insecure attachment may also contribute do developing health symptoms by influencing the choice of health behaviors. Insecurely attached individuals may exhibit poor preventive health behaviors, less adherence to health promotion activities and more frequent engagement in risky behaviors (Ahrens et al. 2012; Huntsinger and Luecken 2004; Scharfe and Eldredge 2001).
Broadly, previous research seems to be largely in agreement about the higher risk of developing health symptoms among insecurely attached individuals. However, there is more doubt about two important, specific points: (a) similarities and differences in terms of health consequences between different patterns of insecure attachment (e.g., avoidant vs. anxious attachment), and a related issue of (b) differential consequences of insecure attachment patterns for different classes of health symptoms. For example, Kotler et al. (1994) reported that an avoidant, but not anxious attachment was linked to maladaptive style of emotional control (suppression), which was related to emotion focused coping style. This variable was, in turn, connected to negative psychological and physical health symptoms. Moreover, Gouin and others (Gouin et al. 2009; see also: Picardi et al. 2007) showed that attachment avoidance is related to immune system dysregulation (higher inflammatory response) during marital conflict, with no such effect for anxious attachment. Differently, Feeney and Ryan (1994) found that attachment anxiety is linked to higher levels of negative health concerns compared with attachment avoidance (the latter dimension was not related to severity of reported symptoms). Nielsen and colleagues (Nielsen et al. 2017) investigated attachment patterns as predictors of anxiety symptoms. For this group of symptoms, when both avoidant and anxious attachment were controlled for, only attachment anxiety contributed to higher symptom severity. Concurrently, research by Stanton and Campbell (2014) showed that both anxious and avoidant attachment were related to negative health consequences, but this relationship was stronger for an anxious attachment, than for an avoidant attachment. Moreover, when both attachment patterns were posed in the role of joint predictors of health outcomes, only attachment anxiety served as a significant predictor, while attachment avoidance no longer predicted health outcomes (Stanton and Campbell 2014). In the study by Rapoza and colleagues (Rapoza et al. 2016), both anxious and avoidant attachment were correlated with decreased social support (r = −.21 and r = −.20 respectively) but only an anxious attachment was related to increased physical (r = .26) and psychological symptoms (r = .31). However, when social support and both attachment patterns were included in the regression analysis as joint predictors of psychological and physical symptoms, anxious attachment predicted higher severity of both classes of symptoms, while avoidant attachment emerged as a protective factor, negatively related to severity of psychological health problems (relation with physical symptoms was not significant) (Rapoza et al. 2016). While the short review that we provided above makes no pretense of being exhaustive, the discussed examples provide a clear illustration of significance of considering factors like attachment pattern and different symptom groups when studying health-related effects of attachment.
Besides investigating relationships between attachment and health symptoms, researchers have also been interested in variables that may best explain this relationship. One such hypothesized variable is emotion regulation. Emotion regulation has an important place within attachment theory itself. Attachment styles are formed by child-parent interaction patterns. In the process of interacting with their caregiver, an infant can learn specific behavioral, cognitive and affective responses that help him/her attain attachment goals (Bowlby 1977). As anxious attachment can often be formed as a response to an unreliable or inconsistent caregiver, anxiously attached individuals may learn to exaggerate or upregulate their emotion to attract a caregiver’s attention or affect the caregiver’s responses. Avoidant attachment is often characterized by shielding from negative emotions by downregulating one’s own emotional responses or using distraction in an interaction with a caregiver who is seen as rejecting or unavailable (Bowlby 1977; Mikulincer and Shaver 2005; Mikulincer et al. 2003; Shaver and Mikulincer 2002). In other words, although emotion regulation and attachment dimensions are distinct constructs, specific regulatory strategies can be thought of as characteristic of particular attachment patterns. In agreement with this hypothesis, some researchers suggest that insecure attachment may contribute to difficulties in affect regulation, and these difficulties can in turn contribute to shaping negative consequences for psychological and physical health (Cassidy 1994; Fuendeling 1998; Mikulincer et al. 2003; Waters et al. 2010). In other words, the proposition is that emotion regulation difficulties, or maladaptive styles of emotion regulation, can serve as a potential mediator in the relationship between insecure attachment and health outcomes. However, not many researchers have actually empirically tested this hypothesis, especially taking into account different health symptom groups and differentiating between distinct insecure attachment patterns.
Research conducted by Kotler and colleagues (Kotler et al. 1994) that was mentioned before, provided some support for this hypothesis and showed that an avoidant attachment was connected to an emotion-focused style of coping and maladaptive strategies of affect regulation (e.g., affect suppression, self-blame, wishful thinking). These variables were, in turn, related to negative psychological and physical health symptoms. Marganska et al. (2013) showed that emotion dysregulation was a significant mediator of the relationship between attachment styles and (a) depressive symptoms and (b) generalized anxiety disorder, in a student sample. Additionally, Marques et al. (2018) showed that, among women in the postpartum period (up to 12 months after giving birth), difficulties in affect regulation mediated the relationship between attachment anxiety and attachment avoidance, on the one hand, and the mental health symptoms: depression and anxiety, on the other hand. Nielsen and colleagues (Nielsen et al. 2017) conducted a study based on the results obtained from 90 clinically anxious and 57 non-clinical participants. Results indicated that emotion regulation difficulties mediated the relationship between anxious attachment and anxiety symptoms, while attachment avoidance was not related to emotion dysregulation, or to anxiety symptoms. As illustrated by the examples given above, while previous research provides evidence for the role of emotion regulation in attachment-health relationship, research directly testing such mediational models often focuses on explaining the severity of symptoms that are characteristic of mood disorders, e.g., depression or anxiety (for a meta-analysis, see Malik et al. 2015). This is understandable, as this class of symptoms is most closely associated with emotional control difficulties, which constitutes a strong basis for investigating the described mediational models. However, this is also a limitation of previous studies, as the mediational role of emotional dysregulation in the relationship between attachment and symptom groups not as strongly connected with mood disorders has received less research attention. One of the main aims of our current research was to investigate if emotion dysregulation is a reliable and consistent mediator of the relationship between insecure attachment and health, across a variety of health symptom classes, some of which fall outside of the mood disorders domain: bodily pain, vegetative symptoms, social phobia symptoms, agoraphobic symptoms and depressive symptoms.
Summing up, the present research aims to contribute to the discussed issues on three levels: (1) clarify the predictive value of two distinct, insecure adult attachment patterns: anxious and avoidant, on several groups of psychological and physical health symptoms (vegetative symptoms, agoraphobic symptoms, social phobia symptoms, depressive symptoms, pain); (2) investigate if emotion regulation difficulties can mediate the described relationships between attachment dimensions and health across different symptom classes (listed above). For some of these symptoms (agoraphobic or social phobia symptoms), there is a lack of such empirical tests. (3) Investigate the described issues and replicability of obtained findings on the basis of two studies, characterized by different research group demographics and a different data gathering method: student group (Study 1, paper-and-pencil) and a more diverse group of participants, with more variety with respect to age (18–77 years, Study 2, web-based).
Based on previous research that we discussed above (e.g. Feeney and Ryan 1994; Feeney 2000), we hypothesize that attachment anxiety will have stronger relationships with health symptoms than attachment avoidance, and that attachment-health relationships will be mediated by emotion regulation difficulties, across all symptom classes.
The other thing worth noting pertains to the measurement and classification of adult attachment. A common classification of attachment patterns - also present in our analyses - is based on the assessment of two attachment dimensions: attachment avoidance and attachment anxiety. On the basis of the scores obtained for these two dimensions, individuals can be subsequently assigned to attachment types or categories. Typologies of three or four attachment subtypes (e.g., Bartholomew and Horowitz 1991) are the most popular in the attachment literature. However, as such classifications reduce the precision of measurement and statistical power of the study (Fraley and Waller 1998), we opted to adopt a dimensional approach. In such an approach, securely attached individuals are those who obtained low scores on both anxious and avoidant attachment dimensions.
Study 1
Method
Participants and Procedure
Study 1 was conducted with 199 Polish-speaking participants. Because of numerous cases of missing data, responses from 8 participants were excluded from the analysis. The resulting sample consisted of 191 participants, 125 women (66%), 65 men (34%, 1 person did not declare his/her gender), aged 18–33 (M = 22.58, SD = 2.86), recruited at the university library. All participants were students. Respondents filled out a series of questionnaires, the order of which was randomized between participants: Experiences in Close Relationships-Revised Scale, Difficulties in Emotion Regulation Scale, Symptom Checklist 27-plus. Participants also filled out other measures that are not relevant to the present study.
Measures
Experiences in Close Relationships-Revised (ECR-R) by Fraley et al. (2000), Polish version adapted by Lubiewska and collegues (Lubiewska et al. 2016), is a 36-item self-report measure aimed at the assessment of adult attachment dimensions in terms of attachment-related anxiety (18 items) and attachment-related avoidance (18 items). For each of the statements, participants provide their answers on a scale from 1 (strongly disagree) to 7 (strongly agree). Examples of specific items include I often worry that my partner doesn’t really love me for the anxiety scale, or I prefer not to show a partner how I feel deep down for the avoidance scale. The questionnaire achieved high internal consistency in our study (avoidant attachment subscale: α = .89, anxious attachment subscale: α = .87) and in previous studies using this measure (α = .92 for avoidant attachment subscale and α = .88 for anxious attachment, Lubiewska et al. 2016).
The Symptom Checklist-27plus (SCL27-plus) by Hardt (2008), Polish version adapted by Kuncewicz et al. (2014), is a self-report screening measure for mental and physical health difficulties. It contains five scales focused on different classes of symptoms: depressive (5 items), vegetative (5 items), agoraphobic (4 items), social phobia symptoms (5 items) and pain (6 items). General score – global severity index – is based on an average score for items constituting five described subscales. For vegetative, agoraphobia, social phobia and pain symptoms, participants rate how often the specific symptoms occur in general, from 0 (never) to 4 (very often), whereas for depressive symptoms the answer options indicate the number of days in the time frame of the last two weeks, in which individual experienced a particular symptom: 0 (never), 1 (1–2 days); 2 (3–7 days), 3 (8–12 days), 4 (13–14 days). Examples of items include: feeling blank inside, would rather be dead (depressive symptoms); dizziness, heart palpitations (vegetative symptoms); fear to leave the house, feeling spacey (agoraphobic symptoms); others do not like me, feeling unwanted (social phobia symptoms); headaches, chest pain (pain). Moreover, assessment of lifetime depression and a screening question for suicidality are included in the questionnaire – these items are, however, beyond the scope of this article and are not included in the analysis. Reliability indices for SCL27-plus obtained in our study (global severity index: α = .87, depressive symptoms: α = .87, vegetative symptoms: α = .69, agoraphobic symptoms: α = .78, social phobia symptoms: α = .84, and pain: α = .52) were comparable to those obtained in previous studies for the Polish version of the questionnaire, although slightly lower for the pain subscale (global severity index: α = .90, depressive symptoms: α = .81, vegetative symptoms: α = .79, agoraphobic symptoms: α = .80, social phobia symptoms: α = .83, and pain: α = .72; Kuncewicz et al. 2014).
Difficulties in Emotion Regulation Scale (DERS) by Gratz and Roemer (2004), Polish adaptation by Czub (2012), is a 36-item self-report measure assessing emotion regulation difficulties, including non-acceptance of emotional responses, difficulties engaging in goal-directed behavior while upset, emotional impulse control problems, lack of emotional awareness, limited access to emotion regulation strategies while experiencing emotions, and lack of emotional clarity. Average of answers for all 36 questionnaire items constitutes a general score. The answer options are provided within 5-points Likert scale, from 1 (almost never) to 5 (almost always). Examples of items include When I’m upset, I become angry with myself for feeling that way and When I’m upset, I acknowledge my emotions. The questionnaire consists of 6 subscales, but in the presented research we analysed DERS scores only on the basis of a general score. Internal consistency for the Polish version of DERS in the current study was as high (α = .93) as for the original version (α = .93; Gratz and Roemer 2004).
Statistical Analysis
Correlation analyses were conducted with the use of IBM SPSS 21, and mediation models were tested with path analysis approach, using Amos software (Arbuckle 2013). For mediation models, we evaluated our effects using bootstrapping with 5000 iterations. The strength of the indirect effects was tested with 95% biased-corrected bootstrapped confidence intervals. As participants in Study 1 differ from participants in Study 2 in terms of their demographic characteristics (different age and gender structure) our mediation models were controlled for the effects of age and gender.
Results
Means and standard deviations for the entire sample, as well as for women and men separately are presented in Table 1. The conducted statistical comparisons showed that women obtained higher scores for global severity index: t(188) = 2.05; p = 0.042, and vegetative symptoms: t(188) = 2.01; p = 0.046. There were no significant differences for other variables (Table 1).
Zero-order correlations for variables included in the analysis are presented in Table 2.
Both avoidant and anxious attachment were significantly, positively related to the global severity index of the SCL27-plus questionnaire, which reflects a broad range of physical and mental health symptoms. Anxious attachment was significantly, positively related to depressive, vegetative, agoraphobic, and social phobia symptoms, but not to pain severity. Attachment avoidance was positively related to depressive, agoraphobic and social phobia symptoms, but not to pain and vegetative symptoms. Both attachment dimensions were also significantly, positively connected to difficulties in emotion regulation (DERS general score). Moreover, participants who declared greater emotion regulation difficulties also reported a higher degree of health problems – this pattern was observed for every group of symptoms, as well as the global severity index (see Table 2).
Mediation Analyses
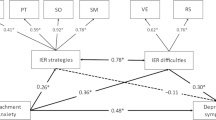
In the next step, to test the mediating role of emotion regulation difficulties (ER difficulties) in the relationship between insecure attachment dimensions (attachment vs. avoidance) and various groups of mental health symptoms, we performed a series of mediation analyses. Within the tested models, both insecure attachment dimensions were placed in the role of simultaneous predictors of health problems, while experienced ER difficulties served as a potential mediator. We created separate models for each of our dependent variables: global symptom severity index (SCL27-plus questionnaire general score, model a) depressive (b), vegetative (c), agoraphobic (d), social phobia symptoms (e) and pain (f). In the next part of this section, we present the results obtained for these mediation models (see Fig. 1). Models were controlled for the effects of age and gender. None of the effects of these demographic variables on health symptoms and emotion regulation difficulties were significant. For all models, attachment anxiety significantly predicted emotion regulation difficulties, while the same effect for avoidant attachment was significant on a trend level (β = .12, p = .061). Both insecure attachment dimensions were also moderately, positively correlated (Fig. 1).

Statistical mediation models of relationships between attachment anxiety, attachment avoidance and health symptoms: global severity index (model a), depressive symptoms (b), vegetative symptoms (c), agoraphobic symptoms (d), social phobia symptoms (e), and pain (f). ER difficulties (DERS questionnaire general score) were included in the models in the mediator role. The coefficients placed within parentheses represent total effects (effects without controlling for the mediator variable). Entries are standardized coefficients. + p < .065. * p < .05. ** p < .001. Models controlled for the effects of sex and age (Study 1)
In the first model, the global severity index of the SCL27-plus questionnaire served as a main dependent variable. As shown in Fig. 1 (model a), when both attachment avoidance and anxiety were placed in the role of simultaneous predictors, only attachment anxiety significantly predicted the global severity index score. Moreover, this effect was partially mediated by emotion regulation difficulties (DERS general score), 95%CIbc = 0.135 to 0.297.
For depressive symptoms (Fig. 1, model b), when effects of both attachment dimensions were accounted for, only attachment anxiety was a significant predictor of depressive symptoms severity. This relation was also partially mediated by emotion regulation difficulties, 95%CIbc = 0.130 to 0.291.
In the next model (Fig. 1, model c), we analysed the predictive value of insecure attachment patterns and ER difficulties on vegetative symptoms. Results indicated that a positive relationship between attachment anxiety and vegetative symptoms was fully mediated by ER difficulties, 95%CIbc = 0.064 to 0.222. Avoidant attachment was not significantly related to this class of health symptoms, both in terms of total effect and direct effect.
Attachment anxiety, but not attachment avoidance, had a significant, positive impact on the severity of agoraphobic symptoms reported by participants (Fig. 1, model d). This relation was partially mediated by ER difficulties, 95%CIbc = 0.038 to 0.187.
Mediation analyses also indicated that both attachment anxiety and attachment avoidance positively predicted social phobia symptoms (Fig. 1, model e). ER difficulties partially mediated the relationship between attachment anxiety and social phobia symptoms (95%CIbc = 0.128 to 0.287) and fully mediated the relationship between attachment avoidance and social phobia (indirect effect significance was on a trend level: 95%CIbc = −0.002 to 0.123, p = .055).
In the last model (Fig. 1, model f), declared pain served as the main dependent variable. Attachment patterns did not significantly predict pain symptoms, both before and after the mediator was introduced into the model. ER difficulties was the only positive, significant predictor of reported pain severity.
Discussion
The results of Study 1 showed that it is attachment anxiety that is a more important predictor of health outcomes, and not attachment avoidance (Feeney and Ryan 1994). Our results showed that anxious attachment predicted a higher severity of depressive, vegetative, agoraphobic, and social phobia symptoms. Anxious attachment also positively predicted the global severity index score. These relationships were mediated by general emotion regulation difficulties, which provides confirmation of the hypothesis about the role of emotion regulation for explaining the relations between insecure attachment patterns and negative health symptoms. This result (significant mediation through ER difficulties) was consistent across various symptom classes. Moreover, our results showed that avoidant attachment was a significant predictor only for social phobia symptoms.
One limitation of Study 1 was that it was conducted only among students (i.e., a homogenous sample). Therefore, in Study 2 we aimed to examine whether the pattern of results obtained in Study 1 would replicate if we focus on a more heterogeneous group of participants (aged between 18 and 77 years old), while also using a different data-gathering method (online questionnaires, instead of paper-and-pencil measures).
Study 2
Method
Participants and Procedure
For Study 2, data was collected online by one of the leading Polish online research panels (Ariadna) in two separate stages – assessment of difficulties in emotion regulation and health symptoms was conducted during the first stage, and a measure of attachment patterns (ECR-R) was completed on a separate occasion a few days after. Measures used in Study 2 were administered to, and completed by, 216 participants. The sample consisted of 107 females (49.5%) and 109 males (50.5%), aged from 18 to 77 years old, M = 43.93, SD = 15.04. More specifically, 11.6% of participants belonged to the 18–24 age group, 20.8% belonged to the 25–34 age group; 16.7% were between 35 to 44 years old; 21.3% between 45 and 54 years; and 29.06% of participants were 55 years of age or older. All participants declared Polish nationality.
Measures
In Study 2, we used the same set of measures as in Study 1.
Experiences in Close Relationships – Revised Scale (ECR-R; Fraley et al. 2000; Polish adaptation: Lubiewska et al. 2016) was used to measure adult attachment anxiety (18 items) and avoidance (18 items) in the sphere of close relationships. Participants provided their answer on a scale from 1 (strongly disagree) to 7 (strongly agree). Both attachment anxiety (α = .94) and attachment avoidance subscale (α = .87) achieved satisfactory reliability.
Difficulties in Emotion Regulation Scale (DERS) by Gratz and Roemer (2004) was used to measure emotion regulation difficulties. Similarly as in Study 1, we used the Polish adaptation of this questionnaire (Czub 2012). The average of answers for all questionnaire items constitutes a general score, reflecting general emotion regulation difficulties. However, as a result of unintentional omission in the research procedure, one item was excluded from this questionnaire (item 25). Consequently, for Study 2, the average score reflecting general difficulties in emotion regulation is based on 35, not 36 items. The answer options are provided within a 5-point Likert scale, from 1 (almost never) to 5 (almost always). The questionnaire consists of 6 subscales, but in the presented research we analysed DERS scores only on the basis of a general score. Internal consistency obtained for DERS in Study 2 was high (α = .94).
As in Study 1, Symptom Checklist-27plus (SCL27-plus) by Hardt (2008), Polish adaptation by Kuncewicz and collegues (Kuncewicz et al. 2014), was used to measure the severity of physical and mental symptoms, which is the main dependent variable in our analyses. The questionnaire has a general score (global severity index), along with 5 subscales, reflecting 5 symptom classes: depressive symptoms, vegetative symptoms, agoraphobic symptoms, symptoms of social phobia and pain. For vegetative, agoraphobia, social phobia and pain symptoms, participants rate how often the specific symptoms occur in general, from 0 (never) to 4 (very often), whereas for depressive symptoms the answer options indicate the number of days in the time frame of the last two weeks, during which the individual experienced a particular symptom: 0 (never), 1 (1–2 days); 2 (3–7 days), 3 (8–12 days), 4 (13–14 days). Moreover, assessment of lifetime depression and a screening question for suicidality are included in the questionnaire – these items are however beyond the scope of this work and are not included in the analysis. Reliability indices obtained in Study 2 for SCL27-plus questionnaire were satisfactory: global severity index: α = .93, depressive symptoms: α = .88, vegetative symptoms: α = .80, agoraphobic symptoms: α = .87, social phobia symptoms: α = .87, and pain: α = .82.
Statistical Analysis
We used the same statistical procedure as in Study 1. IBM SPSS 21 and Amos software (Arbuckle 2013) were used to conduct our analyses. For mediation models, we evaluated our effects using bootstrapping with 5000 re-samples. Indirect effects were tested with 95% biased-corrected bootstrapped confidence intervals. Our mediation models were controlled for the effects of age and gender.
Results
Means and standard deviations for the entire sample, as well as for women and men separately are presented in Table 3. Mean values obtained for Study 2 were very similar to those from Study 1, although respondents in Study 2 declared lower severity of depressive symptoms than those in Study 1. In contrast to Study 1, results of the Student’s t-tests showed that there were no significant differences between women and men with regard to attachment dimensions, health symptoms and emotion regulation difficulties.
Zero-order correlations for variables included in the analysis are presented in Table 4.
Our analysis showed that, similarly to the results of the previous study, attachment anxiety was significantly, positively related to the global severity index, depressive symptoms, vegetative symptoms, agoraphobic and social phobia symptoms, but not to pain. Attachment avoidance was positively correlated with agoraphobic and vegetative symptoms, but not with pain, social phobia and depressive symptoms. Both insecure attachment dimensions were also significantly, positively, related to emotion regulation difficulties (DERS general score). Higher emotion regulation difficulties were also significantly related to all health symptom classes, as well as the global severity index (Table 4) – this also positively replicates the results obtained in Study 1.
Mediation Analyses
In the second step, we created a series of mediation models, to investigate the mediating role of emotion regulation difficulties in the relationship between anxious and avoidant attachment dimensions on the one hand, and mental health symptoms on the other. Within the mediation models, we included both insecure attachment dimensions as simultaneous predictors of health problems, while experienced difficulties in emotion regulation served as a potential mediator. As in Study 1, we created separate models for each of our dependent variables: global symptom severity index (SCL general score, model a) depressive (b), vegetative (c), agoraphobic (d), social phobia symptoms (e), and pain (f). In the next part of this section we present the results obtained for these mediation models (see Fig. 2). Models were controlled for the effects of age and gender. Age was negatively related to emotion regulation difficulties (β = −.17, p = .007). We did not obtain significant relationships between demographic variables (age, gender) and any of the health symptom groups tested within our models. For all models, both attachment anxiety and attachment avoidance significantly predicted emotion regulation difficulties (ER difficulties). As in Study 1, both insecure attachment dimensions were also moderately, positively correlated (Fig. 2).

Statistical mediation models of relationships between attachment anxiety, attachment avoidance and health symptoms: global severity index (model a), depressive symptoms (b) vegetative symptoms (c), agoraphobic symptoms (d), social phobia symptoms (e) and pain (f). ER difficulties (DERS questionnaire general score) were included in the models in the mediator role. The coefficients placed within parentheses represent total effects (effects without controlling for the mediator variable). Entries are standardized coefficients. + p < .065. * p < .05. ** p < .001. Models controlled for the effects of sex and age (Study 2)
In the first model, the global severity index of the SCL questionnaire served as the main dependent variable (Fig. 2, model a). Attachment anxiety, but not attachment avoidance, was a significant, positive predictor of the global severity index score. These relations became insignificant after introducing a mediator to the model – our results indicated full mediation, 95%CIbc = 0.045 to 0.220.
In the next model (Fig. 2, model b) we analysed the predictive value of attachment dimensions and ER difficulties on severity of depressive symptoms. Our results showed that, for Study 2, attachment anxiety and attachment avoidance were not significant predictors of depressive symptoms. Emotion regulation difficulties, however, positively predicted severity of this class of symptoms.
Results of the third mediation model (Fig. 2, model c) indicated that ER difficulties fully mediated the relationship between attachment anxiety and vegetative symptoms, 95%CIbc = 0.033 to 0.160. Avoidant attachment did not significantly predict this class of health symptoms (although the effect was close to significance, β = .12, p = .052).
For agoraphobic symptoms (Fig. 2, model d), attachment anxiety, but not attachment avoidance, had a significant, positive impact on the severity of agoraphobic symptoms reported by participants. This relation was fully mediated by ER difficulties, 95%CIbc = 0.043 to 0.210.
In the fifth model for Study 2 (depicted on Fig. 2, model e) we analysed the predictive power of insecure attachment dimensions and ER difficulties in explaining social phobia symptoms severity. Our results showed that attachment anxiety, but not attachment avoidance, significantly predicted severity of social phobia symptoms. ER difficulties fully mediated the relation between anxious attachment and social phobia symptoms, 95%CIbc = 0.041 to 0.197.
In the last model (Fig. 2, model f), declared pain served as a main dependent variable. As in Study 1, both attachment anxiety and attachment avoidance did not significantly predict pain symptoms. ER difficulties was the only significant predictor of this symptom group.
Discussion
In Study 2 we replicated the results obtained in Study 1, suggesting that attachment anxiety is a stronger predictor of health outcomes than attachment avoidance (Feeney and Ryan 1994). Higher anxious attachment predicted a higher global severity index score, as well as a higher level of vegetative, agoraphobic, and social phobia symptoms. Mentioned relationships were also fully mediated by emotion regulation difficulties, which lends further support to the claim about the role of emotion regulation in explaining the relations between insecure attachment and health symptoms. When anxious attachment was controlled, avoidant attachment did not significantly predict any health outcomes.
General Discussion
The main objective of our research was (a) to investigate the predictive value of two distinct insecure attachment patterns (i.e., avoidant and anxious) for separate groups of health symptoms, and (b) to examine the mediating role of emotional difficulties in the attachment-health relationship, across several groups of health symptoms.
Broadly speaking, the results of two studies indicated that anxious attachment may have stronger consequences for quality of health across a variety of health symptoms, than avoidant attachment. Even when attachment avoidance was significantly related to health symptoms on the level of bivariate correlations, when effects of both attachment dimensions were controlled for, it was attachment anxiety, and not attachment avoidance, that was a significant predictor of most health symptom classes. Specifically, participants higher in attachment anxiety reported a higher severity of vegetative symptoms, agoraphobic symptoms, social phobia symptoms (Studies 1 and 2) and depressive symptoms (Study 1). High attachment anxiety was also predictive of higher global severity index scores (Studies 1 and 2). On the other hand, participants high in attachment avoidance declared higher social phobia symptoms in Study 1 (but not in Study 2). In other words, we obtained a fairly consistent pattern of results indicating that attachment anxiety has broader, and more reliable predictive value for health outcomes, than attachment avoidance.
This pattern of results underlines the notion that insecure attachment is not a unitary phenomenon, but is characterized by substantial multidimensionality (e.g., Brennan et al. 1998). Moreover, multifaceted structure of this construct seems to be very important and consequential for explaining attachment-health relationships (Feeney and Ryan 1994; Feeney 2000). Although frameworks aimed at explaining the mechanisms that govern the attachment and health relationship seem to apply to both attachment anxiety and attachment avoidance (Kotler et al. 1994; Maunder and Hunter 2001; West et al. 1986), our results are in line with previous research showing negative health consequences for an anxious, but not avoidant attachment pattern (e.g., Ciechanowski et al. 2002; Feeney and Ryan 1994; McWilliams and Bailey 2010; Rapoza et al. 2016). However, our findings also go beyond earlier research results by considering specific symptom classes, for which avoidance and anxiety effects were previously untested, such as social phobia and agoraphobic symptoms. Previous research has shown that anxious attachment may be more consequential for health than avoidant attachment, as anxiously attached individuals may chronically experience higher levels of anxiety and distress, which can contribute to negative health consequences. Moreover, they can be hypervigilant to distress signals and be prone to self-blame for their own state of health (Feeney 2000; Feeney and Ryan 1994; Marganska et al. 2013).
The results of our analyses also lend clear support to the hypothesis that emotion regulation difficulties may be the mechanism through which attachment patterns can influence health symptoms (Cassidy 1994; Mikulincer et al. 2003; Pietromonaco et al. 2015; Waters et al. 2010). Previous research has shown, for example, that emotion regulation mediates the relationship between anxious attachment and mood disorders (Marganska et al. 2013; Nielsen et al. 2017; Pascuzzo et al. 2015). In agreement with these results, emotion regulation difficulties mediated all significant effects of attachment on health, in both of our studies. In light of these results, it seems possible that people high in anxious attachment have higher levels of health symptoms due to general problems with emotion regulation.
Importantly, our results contribute to previous knowledge by providing evidence that emotion regulation can also mediate attachment-health relationships for symptom groups that are not categorized as mood disorders, like agoraphobic or social phobia symptoms, for which we did not have such evidence in previous studies. Moreover, emotion regulation difficulties were also a positive predictor of all health symptom classes in Study 1 and Study 2, even when the effects of attachment dimensions were insignificant. This illustrates the high importance of emotion regulation to health and is in agreement with previous literature on this subject (Gross and Muñoz 1995; Jazaieri et al. 2013; Werner and Gross 2010). For instance, previous research conducted on representative samples has shown that emotional competencies (which include emotion regulation) predict objective health symptoms indicators (e.g., drug intake or doctor consultations) over and above other important factors like sex, education, physical activity, social support or diet habits (Mikolajczak et al. 2015).
It is important to note that the difference between attachment anxiety and avoidance in predicting health outcomes may be also the result of differences in the subjective evaluation of one’s own health symptoms. Anxious attachment is characterized by proneness to states of negative emotions, overvigilance and high sensitivity, which may lead anxious individual to perceiving their health concerns as more serious (e.g., Meredith et al. 2008). On the other hand, avoidant individuals tend to value self-reliance, and avoid help-seeking, which in the domain of health behaviors manifests itself by, for example, less frequent visits to health professionals (Feeney and Ryan 1994; Kotler et al. 1994). These individuals may be not as willing to report the health symptoms that they are experiencing. Such an interpretation is in agreement with a line of research showing that attachment avoidance may be more strongly related to physiological stress responses than to self-reported stress, while opposite effects are observed for attachment anxiety. In other words, subjective responses to distress (or: perceived distress) may be dampened in the case of avoidant individuals, and elevated among those anxiously attached (Diamond and Fagundes 2010; Diamond et al. 2006; Maunder et al. 2006). Moreover, there is some evidence that individuals high in anxious attachment have a tendency to catastrophize their pain and emphasize their negative feelings to elicit more support from others (Meredith et al. 2008).
Interestingly, we did not find elevated levels of pain symptoms for anxiously attached participants, nor for avoidantly attached ones (consistent across both studies). The pain subscale of the SCL27-plus questionnaire is concerned with physical symptoms of bodily pain, like chest pain or joints pain. Such symptoms usually have weaker and less direct psychological underpinnings than, for example, agoraphobic or social phobia symptoms. This may be the reason why we did not obtain significant relations between pain and insecure attachment dimensions. In other words, our results seem to indicate that adult attachment patterns have more visible connections with symptoms directly related to the psychological sphere, compared to symptoms that have less direct psychological underpinnings (pain), at least in non-clinical samples (like both of our samples in Study 1 and 2). Most of the previous studies that indicate a positive relationship between insecure attachment dimensions and pain severity were based on clinical populations, patients experiencing chronic pain, with a high level of pain complaints or members of other clinical groups, like cancer patients (Kolb 1982; Meredith et al. 2008; Mikail et al. 1994; Romeo et al. 2017). Our results indicated that in the general population, this relation may not be as reliable – future studies should conduct further tests for the described pattern.
Although our research led to largely consistent results, we also obtained some interesting differences between the results of both of our studies. As mentioned before, the only symptom class that was significantly predicted by attachment avoidance when anxious attachment was controlled was social phobia. Participants high in attachment avoidance declared a higher severity of social phobia symptoms in Study 1, but not in Study 2. Although the results of the two conducted studies give, in this case, mixed results, the discussed finding seems interesting. Among the symptom groups investigated in the present research, social phobia symptoms seem to have special significance in the psychology of avoidant attachment. The core characteristic of this insecure attachment pattern is avoidance of engagement in close relationships and distrust displayed in interpersonal situations, which may be motivated by a fear of rejection or experiences of rejection in the past (e.g., Bartholomew 1993; Feeney and Noller 1996). Such a behavioral description fits perfectly in the picture of social phobia symptoms, and may explain why an avoidant attachment dimension can be connected to social phobia symptoms more reliably than to other symptom classes, like agoraphobia or depression. Although this explanation can be potentially viable, our studies led to mixed results, which should be replicated and expanded in future research.
In the case of depressive symptoms, Study 1’s participants (this study was based on a student sample), which were high in attachment anxiety, declared higher depressive symptoms. This result is consistent with a branch of previous studies, indicating that insecurely attached individuals have a greater possibility of developing depressive symptoms (Carnelley et al. 1994; Malik et al. 2015; Murphy and Bates 1997; Shaver et al. 2005; Wei et al. 2005) In Study 2, however, insecure attachment patterns did not significantly predict depressive symptoms. Our samples in both studies potentially differed in many respects (e.g., education, income – although these variables were not controlled), so the pattern of results may be a consequence of these differences. However, another possible explanation pertains to measurement of this class of symptoms. The SCL-27plus questionnaire only measures depressive symptoms in relation to the last two weeks (it is not the case for other groups of symptoms). This feature can render measurements of depressive symptoms less reliable and more contaminated by transient mood effects. Future studies should further investigate these effects with the use of other measures of depression severity.
Summing up, our results provide a strong support for the notion that (1) attachment avoidance and attachment anxiety differently predict health outcomes, and that (2) emotion dysregulation can be one of the mechanisms explaining attachment – health relationships.
Limitations
The most important limitation of the presented studies is its cross-sectional character. This type of study is not ideal for investigating causal links between variables. While path models contain directional effects, path analysis does not establish causality by itself. Unfortunately, most of the previous studies investigating links between attachment dimensions, health symptoms and emotion regulation have a cross-sectional character. More studies conducted in a longitudinal fashion are needed. In both of our studies, we also use the exact same set of measures. For future studies it would be beneficial to use a variety of measures addressing a wide scope of health symptoms and insecure attachment patterns. Moreover, our analysis is based on two studies with sample sizes of around two hundred participants in each of them (Study 1, n = 191, Study 2, n = 216). There is still little consensus on the recommended sample size for structural equation modelling, and the discussion on this topic is still ongoing (Kline 2011; Sivo et al. 2006; Wang and Wang 2012; Wolf et al. 2013). However, we created multiple path analysis models, and one direction for future research is to replicate the findings presented here using larger sample sizes.
References
Ahrens, K. R., Ciechanowski, P., & Katon, W. (2012). Associations between adult attachment style and health risk behaviors in an adult female primary care population. Journal of Psychosomatic Research, 72(5), 364–370. https://doi.org/10.1016/j.jpsychores.2012.02.002.
Arbuckle, J. L. (2013). IBM SPSS Amos 22 user’s guide. Crawfordville: Amos Development Corporation.
Bartholomew, K. (1993). From childhood to adult relationships: Attachment theory and research. In S. Duck (Ed.), Understanding relationship processes series, Vol. 2. Learning about relationships (pp. 30–62). Thousand Oaks: Sage Publications, Inc..
Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: a test of a four category model. Journal of Personality and Social Psychology, 61(2), 226.
Bowlby, J. (1977). The making and breaking of affectional bonds. I. Aetiology and psychopathology in the light of attachment theory. An expanded version of the Fiftieth Maudsley Lecture, delivered before the Royal College of Psychiatrists, 19 November 1976. The British Journal of Psychiatry, 130, 201–210. https://doi.org/10.1192/bjp.130.3.201.
Bowlby, J. (1982). Attachment and loss: Retrospect and prospect. American Journal of Orthopsychiatry, 52(4), 664–678. https://doi.org/10.1111/j.1939-0025.1982.tb01456.x.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). New York: Guilford Press.
Carnelley, K. B., Pietromonaco, P. R., & Jaffe, K. (1994). Depression, working models of others, and relationship functioning. Journal of Personality and Social Psychology, 66(1), 127–140. https://doi.org/10.1037/0022-3514.66.1.127.
Cassidy, J. (1994). Emotion regulation: Influences of attachment relationships. Monographs of the Society for Research in Child Development, 59(2–3), 228–249. https://doi.org/10.1111/j.1540-5834.1994.tb01287.x.
Ciechanowski, P. S., Walker, E. A., Katon, W. J., & Russo, J. E. (2002). Attachment theory: A model for health care utilization and somatization. Psychosomatic Medicine, 64(4), 660–667. https://doi.org/10.1097/01.PSY.0000021948.90613.76.
Cohen, S., & Janicki-Deverts, D. (2009). Can we improve our physical health by altering our social networks? Perspectives on Psychological Science, 4(4), 375–378. https://doi.org/10.1111/j.1745-6924.2009.01141.x.
Czub T. (2012). Opis Kwestionariusza trudności w regulacji emocji – DERS/PL. Poznań: Instytut Psychologii Uniwersytetu im. Adama Mickiewicza (unpublished manuscript).
Diamond, L. M., & Fagundes, C. P. (2010). Psychobiological research on attachment. Journal of Social and Personal Relationships, 27(2), 218–225. https://doi.org/10.1177/0265407509360906.
Diamond, L. M., Hicks, A. M., & Otter-Henderson, K. (2006). Physiological evidence for repressive coping among avoidantly attached adults. Journal of Social and Personal Relationships, 23(2), 205–229. https://doi.org/10.1177/0265407506062470.
Edelstein, R. S., & Shaver, P. R. (2004). Avoidant attachment: Exploration of an oxymoron. In D. J. Mashek & A. P. Aron (Eds.), Handbook of closeness and intimacy (pp. 397–412). Mahwah: Lawrence Erlbaum Associates Publishers.
Egeland, B., & Sroufe, L. A. (1981). Attachment and early maltreatment. Child Development, 52(1), 44–52. https://doi.org/10.2307/1129213.
Feeney, J. A. (2000). Implications of attachment style for patterns of health and illness. Child: Care, Health and Development, 26(4), 277–288. https://doi.org/10.1046/j.1365-2214.2000.00146.x.
Feeney, J., & Noller, P. (1996). SAGE series on close relationships: Adult attachment. Thousand Oaks: SAGE Publications, Inc.. https://doi.org/10.4135/9781452243276.
Feeney, J. A., & Ryan, S. M. (1994). Attachment style and affect regulation: Relationships with health behavior and family eperiences of illness in a student sample. Health Psychology, 13(4), 334–345. https://doi.org/10.1037/0278-6133.13.4.334.
Fraley, R. C., & Shaver, P. R. (2000). Adult romantic attachment: Theoretical developments, emerging controversies, and unanswered questions. Review of General Psychology, 4(2), 132–154. https://doi.org/10.1037/1089-2680.4.2.132.
Fraley, R. C., & Waller, N. G. (1998). Adult attachment patterns: A test of the typological model. In J. A. Simpson & W. S. Rhodes (Eds.), Attachment theory and close relationships (pp. 77–114). New York: Guilford Press.
Fraley, R. C., Waller, N. G., & Brennan, K. A. (2000). An item-response theory analysis of self-report measures of adult attachment. Journal of Personality and Social Psychology, 78(2), 350–365. https://doi.org/10.1037/0022-3514.78.2.350.
Fuendeling, J. M. (1998). Affect regulation as a stylistic process within adult attachment. Journal of Social and Personal Relationships, 15(3), 291–322. https://doi.org/10.1177/0265407598153001.
Gouin, J. P., Glaser, R., Loving, T. J., Malarkey, W. B., Stowell, J., Houts, C., & Kiecolt-Glaser, J. K. (2009). Attachment avoidance predicts inflammatory responses to marital conflict. Brain, Behavior, and Immunity, 23(7), 898–904. https://doi.org/10.1016/j.bbi.2008.09.016.
Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. https://doi.org/10.1007/s10862-008-9102-4.
Gross, J. J., & Muñoz, R. F. (1995). Emotion regulation and mental health. Clinical Psychology: Science and Practice, 2(2), 151–164. https://doi.org/10.1111/j.1468-2850.1995.tb00036.x.
Hardt, J. (2008). The symptom checklist-27-plus (SCL-27-plus): A modern conceptualization of a traditional screening instrument. GMS Psycho-Social Medicine, 5 Doc08.
Harms, P. D. (2011). Adult attachment styles in the workplace. Human Resource Management Review, 21(4), 285–296. https://doi.org/10.1016/j.hrmr.2010.10.006.
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), e1000316. https://doi.org/10.1371/journal.pmed.1000316.
Huntsinger, E. T., & Luecken, L. J. (2004). Attachment relationships and health behavior: The mediational role of self-esteem. Psychology & Health, 19(4), 515–526. https://doi.org/10.1080/15374410802698396.
Jazaieri, H., Urry, H. L., & Gross, J. J. (2013). Affective disturbance and psychopathology: An emotion regulation perspective. Journal of Experimental Psychopathology, 4(5), 584–599. https://doi.org/10.5127/jep.030312.
Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York: The Guilford Press.
Kolb, L. C. (1982). Attachment behavior and pain complaints. Psychosomatics, 23(4), 413–425. https://doi.org/10.1016/S0033-3182(82)73404-8.
Kotler, T., Buzwell, S., Romeo, Y., & Bowland, J. (1994). Avoidant attachment as a risk factor for health. British Journal of Medical Psychology, 67(3), 237–245. https://doi.org/10.1111/j.2044-8341.1994.tb01793.x.
Kuncewicz, D., Dragan, M., & Hardt, J. (2014). Validation of the polish version of the symptom checklist-27-plus questionnaire. Psychiatria Polska, 48(2), 345–358.
Li, T., & Chan, D. K. S. (2012). How anxious and avoidant attachment affect romantic relationship quality differently: A meta-analytic review. European Journal of Social Psychology, 42(4), 406–419. https://doi.org/10.1002/ejsp.1842.
Lubiewska, K., Głogowska, K., Mickiewicz, K., Wojtynkiewicz, E., Izdebski, P., & Wiśniewski, C. (2016). Skala experience in close relationships-revised: Struktura, rzetelność oraz skrócona wersja skali w polskiej próbie. Psychologia Rozwojowa, 1, 49–63. https://doi.org/10.4467/20843879PR.16.004.4793.
Malik, S., Wells, A., & Wittkowski, A. (2015). Emotion regulation as a mediator in the relationship between attachment and depressive symptomatology: A systematic review. Journal of Affective Disorders, 172, 428–444. https://doi.org/10.1016/j.jad.2014.10.007.
Marganska, A., Gallagher, M., & Miranda, R. (2013). Adult attachment, emotion dysregulation, and symptoms of depression and generalized anxiety disorder. American Journal of Orthopsychiatry, 83(1), 131–141. https://doi.org/10.1111/ajop.12001.
Marques, R., Monteiro, F., Canavarro, M. C., & Fonseca, A. (2018). The role of emotion regulation difficulties in the relationship between attachment representations and depressive and anxiety symptoms in the postpartum period. Journal of Affective Disorders, 238, 39–46. https://doi.org/10.1016/j.jad.2018.05.013.
Maunder, R. G., & Hunter, J. J. (2001). Attachment and psychosomatic medicine: Developmental contributions to stress and disease. Psychosomatic Medicine, 63(4), 556–567. https://doi.org/10.1097/00006842-200107000-00006.
Maunder, R. G., Lancee, W. J., Nolan, R. P., Hunter, J. J., & Tannenbaum, D. W. (2006). The relationship of attachment insecurity to subjective stress and autonomic function during standardized acute stress in healthy adults. Journal of Psychosomatic Research, 60(3), 283–290. https://doi.org/10.1016/j.jpsychores.2005.08.013.
McWilliams, L. A., & Bailey, S. J. (2010). Associations between adult attachment ratings and health conditions: Evidence from the National Comorbidity Survey Replication. Health Psychology, 29(4), 446–453. https://doi.org/10.1037/a0020061.
Meredith, P., Ownsworth, T., & Strong, J. (2008). A review of the evidence linking adult attachment theory and chronic pain: Presenting a conceptual model. Clinical Psychology Review, 28(3), 407–429. https://doi.org/10.1016/j.cpr.2007.07.009.
Mickelson, K. D., Kessler, R. C., & Shaver, P. R. (1997). Adult attachment in a nationally representative sample. Journal of Personality and Social Psychology, 73(5), 1092–1106. https://doi.org/10.1037/0022-3514.73.5.1092.
Mikail, S. F., Henderson, P. R., & Tasca, G. A. (1994). An interpersonally based model of chronic pain: An application of attachment theory. Clinical Psychology Review, 14(1), 1–16. https://doi.org/10.1016/0272-7358(94)90045-0.
Mikolajczak, M., Avalosse, H., Vancorenland, S., Verniest, R., Callens, M., van Broeck, N., Fantini-Hauwel, C., & Mierop, A. (2015). A nationally representative study of emotional competence and health. Emotion, 15(5), 653–667. https://doi.org/10.1037/emo0000034.
Mikulincer, M., & Shaver, P. R. (2005). Attachment theory and emotions in close relationships: Exploring the attachment-related dynamics of emotional reactions to relational events. Personal Relationships, 12(2), 149–168. https://doi.org/10.1111/j.1350-4126.2005.00108.x.
Mikulincer, M., Shaver, P. R., & Pereg, D. (2003). Attachment theory and affect regulation: The dynamics, development, and cognitive consequences of attachment-related strategies. Motivation and Emotion, 27(2), 77–102. https://doi.org/10.1023/A:1024515519160.
Murphy, B., & Bates, G. W. (1997). Adult attachment style and vulnerability to depression. Personality and Individual Differences, 22(6), 835–844. https://doi.org/10.1016/S0191-8869(96)00277-2.
Nielsen, S. K. K., Lønfeldt, N., Wolitzky-Taylor, K. B., Hageman, I., Vangkilde, S., & Daniel, S. I. F. (2017). Adult attachment style and anxiety - the mediating role of emotion regulation. Journal of Affective Disorders, 218, 253–259. https://doi.org/10.1016/j.jad.2017.04.047.
Pascuzzo, K., Moss, E., & Cyr, C. (2015). Attachment and emotion regulation strategies in predicting adult psychopathology. SAGE Open, 5(3). https://doi.org/10.1177/2158244015604695.
Picardi, A., Battisti, F., Tarsitani, L., Baldassari, M., Copertaro, A., Mocchegiani, E., & Biondi, M. (2007). Attachment security and immunity in healthy women. Psychosomatic Medicine, 69(1), 40–46. https://doi.org/10.1097/PSY.0b013e31802dd777.
Pietromonaco, P. R., Uchino, B., & Dunkel Schetter, C. (2013). Close relationship processes and health: Implications of attachment theory for health and disease. Health Psychology, 32(5), 499–513. https://doi.org/10.1037/a0029349.
Pietromonaco, P. R., DeVito, C. C., Ge, F., & Lembke, J. (2015). Health and attachment processes. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and research: New directions and emerging themes (pp. 287–318). New York: Guilford Press.
Rapoza, K. A., Vassell, K., Wilson, D. T., Robertson, T. W., Manzella, D. J., Ortiz-Garcia, A. L., & Jimenez-Lazar, L. A. (2016). Attachment as a moderating factor between social support, physical health, and psychological symptoms. SAGE Open, 6(4), 1–13. https://doi.org/10.1177/2158244016682818.
Romeo, A., Tesio, V., Castelnuovo, G., & Castelli, L. (2017). Attachment style and chronic pain: Toward an interpersonal model of pain. Frontiers in Psychology, 8, 284. https://doi.org/10.3389/fpsyg.2017.00284.
Scharfe, E., & Eldredge, D. (2001). Associations between attachment representations and health behaviors in late adolescence. Journal of Health Psychology, 6(3), 295–307. https://doi.org/10.1177/135910530100600303.
Shaver, P. R., & Mikulincer, M. (2002). Attachment-related psychodynamics. Attachment & Human Development, 4(2), 133–161. https://doi.org/10.1080/14616730210154171.
Shaver, P. R., Schachner, D. A., & Mikulincer, M. (2005). Attachment style, excessive reassurance seeking, relationship processes, and depression. Personality and Social Psychology Bulletin, 31(3), 343–359. https://doi.org/10.1177/0146167204271709.
Sivo, S. A., Fan, X., Witta, E. L., & Willse, J. T. (2006). The search for "optimal" cutoff properties: Fit index criteria in structural equation modeling. The Journal of Experimental Education, 74(3), 267–288. https://doi.org/10.1177/0049124108314720.
Stanton, S. C., & Campbell, L. (2014). Perceived social support moderates the link between attachment anxiety and health outcomes. PLoS One, 9(4), e95358. https://doi.org/10.1371/journal.pone.0095358.
Uchino, B. N. (2006). Social support and health: A review of physiological processes potentially underlying links to disease outcomes. Journal of Behavioral Medicine, 29(4), 377–387. https://doi.org/10.1007/s10865-006-9056-5.
Wang, J., & Wang, X. (2012). Sample size for structural equation modeling. In Structural equation modeling: Applications using Mplus (pp. 391–428). West Sussex:Wiley.
Waters, S. F., Virmani, E. A., Thompson, R. A., Meyer, S., Raikes, H. A., & Jochem, R. (2010). Emotion regulation and attachment: Unpacking two constructs and their association. Journal of Psychopathology and Behavioral Assessment, 32(1), 37–47. https://doi.org/10.1007/s10862-009-9163-z.
Wei, M., Mallinckrodt, B., Larson, L. M., & Zakalik, R. A. (2005). Adult attachment, depressive symptoms, and validation from self versus others. Journal of Counseling Psychology, 52(3), 368–377. https://doi.org/10.1037/0022-0167.52.3.368.
Werner, K., & Gross, J. J. (2010). Emotion regulation and psychopathology. A conceptual framework. In A. M. Kring & D. M. Sloan (Eds.), Emotion regulation and psychopathology. A transdiagnostic approach to etiology and treatment (pp. 13–37). New York: Guilford Press.
West, M., Livesley, W. J., Reiffer, L., & Sheldon, A. (1986). The place of attachment in the life events model of stress and illness. The Canadian Journal of Psychiatry, 31(3), 202–207. https://doi.org/10.1177/070674378603100304.
Wolf, E. J., Harrington, K. M., Clark, S. L., & Miller, M. W. (2013). Sample size requirements for structural equation models: An evaluation of power, bias, and solution propriety. Educational and Psychological Measurement, 76(6), 913–934. https://doi.org/10.1177/0013164413495237.
Funding
The preparation of this paper was supported by National Science Centre grants: 2016/21/N/HS6/02678 and 2014/15/N/HS6/04160.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lewczuk, K., Kobylińska, D., Marchlewska, M. et al. Adult attachment and health symptoms: The mediating role of emotion regulation difficulties. Curr Psychol 40, 1720–1733 (2021). https://doi.org/10.1007/s12144-018-0097-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-018-0097-z