
Abstract
In 1957, an anonymous editorial published in the American Journal of Public Health boldly titled itself, “Prediction and Theory in Epidemiology”, and raised the ante even higher in its subtitle: “Where there is no vision the people perish. Proverbs XXIX.18” Theory is indeed inextricably linked to vision—the Greek word “theoria” refers to seeing inwards, such that to theorize is to use our mind’s eye systematically, following articulated principles, to discern meaningful patterns among both ideas and observations, and to develop causal explanations. Until the last decade of the 20th c. CE, however, development or analysis of epidemiologic theories of disease distribution in the mainstream English-language literature was a rare event. A shift is now underway. In this article, guided by the ecosocial theory of disease distribution, I review developments in contemporary use of explicit epidemiologic theories, and provide critical suggestions for their further development and application.
Similar content being viewed by others

Introduction
In 1957, an anonymous editorial published in the American Journal of Public Health boldly titled itself, “Prediction and Theory in Epidemiology”, and raised the ante even higher in its subtitle: “‘Where there is no vision the people perish.’ Proverbs XXIX.18” [1]. Written to accompany an article focused on the changing epidemiology of tuberculosis, as it shifted from being a disease of younger to older persons, and also was becoming increasingly “prevalent among the economically underprivileged,” the editorial emphasized the resounding importance of epidemiologic theory for prediction and disease control. Observing that “as a method for advancing knowledge, the analysis of theoretical models has proved fruitful in other fields—vide theoretical physics—and there would appear to be no a priori reason why this should not be equally true in epidemiology,” it optimistically concluded: “As the present interest in the epidemiology of noncommunicable diseases continues to expand there is need for the further development of a theoretical epidemiology” [1, pp.1306-7].
Theory is indeed inextricably linked to vision—traced to its Greek roots, the word “theoria” refers to seeing inwards [2], such that to theorize is to use our mind’s eye systematically, following articulated principles, to discern meaningful patterns among both ideas and observations, and develop causal explanations [3••]. Until the last decade of the 20th c. CE, however, development or analysis of epidemiologic theories of disease distribution in the mainstream English-language literature was a rare event [3••, 4]. A shift is now underway. In this article, guided by the ecosocial theory of disease distribution, I review developments in contemporary use of explicit epidemiologic theories and provide critical suggestions for their further development and application.
Epidemiologic Theory: An Intrinsic Part of Epidemiology
But first: why bother about epidemiologic theory? Simply put, in epidemiology, as in any science, the causal theories it employs are key to its definition and practices [3••, 4–6]. A corollary is that methods, however vital for testing hypotheses, cannot by themselves define a scientific discipline [3••, 6]; think only of the shared use of randomized trials in the public health, biomedical, and social sciences [7, 8].
Moreover, in the case of epidemiology, two aspects of the discipline’s domain and practice, as a population science, require the use of epidemiologic theory [3••, 5]. The first is epidemiology’s intrinsic interest in elucidating causal explanations of disease rates in populations, not just disease mechanisms in individuals, with these causal explanations necessarily needing to bridge the individual-level and population-level occurrence of disease. The second, linked to this, is every single epidemiological study’s need, no matter what the study design, to grapple with (1) who is eligible to become, and who actually becomes, a study participant, (2) the implications of potential selection bias for affecting the range of exposures and outcomes observed, and (3) the subsequent risk estimates produced.
In both cases, there is no way to get around the need to think about the relationships between—and substantive features of —“individuals” and “populations,” and their implications for disease risk and rates, including their variation by time, place, society, and population group [5]. This thinking about explaining health, disease and well-being at the population level is, in the most basic terms, the stuff of epidemiologic theorizing [3••]. It can no more be eliminated from epidemiology than can the actual or simulated data that fuel epidemiologic research.
Dominant and Alternative Epidemiologic Theories of Disease Distribution: An Early 21st c. CE Appraisal
As I have written about in depth elsewhere [3••, 9–11], present-day epidemiologic theories of disease distribution belong to one of two groups: dominant (biomedical and lifestyle) and alternative (theories used in social epidemiology, broadly writ). Table 1 lists the key features of the theories within these two groups. Table 2, in turn, presents data on trends in the number of articles explicitly focused on epidemiologic theory, as indexed by the Web of Science [12] and PubMed [13]; also included is a selected list of 21st c. CE books from the global North and South addressing epidemiologic theory (nine US and European, all in English, and six Latin American: three in Spanish, three in Portuguese).
Range of Theories: From Dominant to Alternative
In brief, the dominant theories are biomedical and lifestyle [3••]. Together, they respectively (1) focus on individual-level biological characteristics, exposures, and behaviors, and (2) emphasize individually-oriented medical treatment and behavioral interventions, (3) ignore sociodemographic and contextual variables or else treat them as “nuisance” variables whose effects can be controlled through statistical adjustment, and (4) conceptualize population rates as simply the aggregate manifestation of individual-level phenomena [3••, 4, 14, 15]. Dominant metaphors portray the body as a machine and/or output of a genetic program, and “choice” as simply the taste of individual “consumers,” independent of context or constraints. Disease rates and distributions are thus conceptualized and analyzed as a consequence of ostensibly individual-level biological phenomena and freely-made choices, including those affecting the prenatal milieu, with history reduced to a question of individual biological development. Differentials in disease rates by race/ethnicity and gender (for the majority of conditions that occur in both biological females and males) are portrayed as primarily reflecting innate biology and cultural preferences, with difference emphasized over similarity. Multiple causation is addressed through the invocation of a “web of causation” [16], which in effect is “spiderless” [9], and with the causal theory behind what and who appears in the web left unstated [9, 14, 17].
By contrast, the alternatives comprise the diverse array of epidemiologic theories of disease distribution that populate the sub-field of social epidemiology (Table 1). Although differing in their emphases, they nevertheless all (1) are explicit about their theoretical premises, and (2) posit that socially-structured exposures, ranging from macroeconomics to psychosocial stress, drive population patterns of health [3••, 9–11, 17]. While it is beyond the scope of this review to offer a nuanced analysis of each alternative theory listed, they can be usefully subdivided into three groups: sociopolitical, psychosocial, and ecosocial [3••].
The sociopolitical theories, although varied in their approach to social analysis, share the common thread of analyzing disease distribution primarily in relation to power, politics, economics, and rights; elucidating biological pathways is a secondary concern. Examples include the social production of disease, political economy of health, Latin American social medicine (LASM), health and human rights, and fundamental cause. The first three, which gained their names in the 1970s [3••], together have roots that extend back to the mid-1800 s (e.g., in the writings of Engels [18], Virchow [19], and Villermé [20]); although applicable to any type of society, they primarily focus on adverse the health consequences of capitalism, mindful of who benefits from and who bears the burden of economies dedicated to maximizing private profit [3••, 9–11, 17–21, 22, 23••]. The health and human rights approach, developed in the mid-1990s in the wake of the HIV/AIDs epidemic, in turn calls attention to the health impacts of who is engaged in upholding and extending, versus violating and restricting, the five sets of indivisible human rights (economic, social, political, civil, and cultural) articulated in the United Nation’s 1948 Universal Declaration of Human Rights [3••, 24]. “Fundamental cause,” first proposed in 1998, emphasizes the socially-shaped capacity of people to use material and social resources flexibly to improve or protect their health, to the extent that knowledge and technology permits; the “surface” causes (i.e., disease mechanisms) put into play by these fundamental causes are accorded less importance [3••, 25].
The psychosocial theories, by contrast, tend to emphasize people’s psychological perceptions of—and their health-damaging or health-enhancing responses to—social conditions, social interactions, and social status [3••, 26]. Grounded in the early 20th c. CE work on stress response by Cannon [27] and Seyle [28], a major emphasis is on the body’s capacity to regulate biological responses to stress (as per the construct of “allostatic load” [29]); although attention is given to how the perception of and response to stressors are affected by the presence and absence of social and material resources, analysis of the sociopolitical determinants of these resources is typically absent.
The ecosocial theory of disease distribution, which I first proposed in 1994 and have developed since [3••, 5, 9–11, 30–32], shares features of the handful of other recent social epidemiologic theories that engage explicitly and literally with ecology (i.e, not ecology as metaphor or as an abstract stand-in for thinking about levels and cross-level interactions and causation, but actual dynamic ecosystems), and with these other theories, including eco-epidemiology (proposed in 1996 [33]) and critical epidemiology (referring to its 21st c. CE articulation as a specific theory [34], as opposed to its prior use in Latin America as equivalent to “social epidemiology” [17]). Additional important shared features include a concern with history, in relation to not only multilevel societal determinants and trends in population health, but also to the intellectual history of, and conflicts between, diverse epidemiologic theories and the accountability of epidemiologists for the frameworks we employ. Some differences include their attention to the role of overt politics and political movements in shaping societal health (accorded less attention by eco-epidemiology) and to biological mechanisms of pathogenesis (accorded less attention by critical epidemiology). Ecosocial theory, in particular, pays heed to societal and ecologic context, to lifecourse and historical generation, to levels of analysis, and to interrelationships between diverse forms of social inequality, including racism, class, and gender. A central focus is on “embodiment,” referring to how we literally embody, biologically, our lived experience, in societal and ecological context, thereby creating population patterns of health and disease; another is on “accountability and agency,” both for social inequalities in health and for ways they are—or are not—monitored, analyzed, and addressed [3••, 5, 9–11, 30–32].
As should be evident, although the dominant and alternative theories certainly can and do overlap in their recognition of specific exposures (e.g., viruses, diet, smoking) and also in their use of constructs (e.g., lifecourse, etiologic period), they nevertheless differ profoundly in how they theorize the relevant causal pathways. It is one thing, after all, to agree that HIV causes HIV/AIDS; it is another entirely to explain who, in which societies and which population groups, is most at risk of becoming infected and developing the disease, including via what pathways of infection and at what point in the lifecourse (e.g., as an infant, adolescent, or adult) [3••, 24, 35].
Trends: Dominant and Alternative Epidemiologic Theories
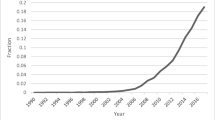
Before reviewing recent trends in the explicit use of the epidemiologic theories, it is important to underscore just how dominant the dominant approaches are. Figure 1 offers an illustration. Thus, whether evaluated in terms of grants awarded by the US National Institutes of Health [36], or by articles included in PubMed [13], scientific work indexed by the terms “biomedical OR lifestyle”—especially with a genetic focus—completely overshadows work indexed by “social epidemiology OR health disparities”. For grants actively funded as of mid-July 2013, the ratio was on the order of 230:1; for articles, it was on the order of 410:1.

Although the mapping of index words to underlying theory might not be 1:1, nevertheless, work indexed by “biomedical” or “lifestyle” is unlikely to be informed by social epidemiologic theories of disease distribution, and vice versa. Relatedly, the extent of misclassification required to dilute the ratios reported above would need to be enormous. Thus, Fig. 1 offers good grounds for inferring that despite the recent growth of alternative theories of disease distribution, as reviewed below, their influence on the actual funding and products of present-day epidemiologic research is, at best, modest.
Common Trends Across all Theories
One of the more notable trends in Table 2, cutting across all theories, is the pronounced rise, beginning in the 1990s and accelerating in the 21st c. CE, of conceptual articles about epidemiologic theory. Indeed, for more than half of the different alternative social epidemiology theories listed, the number of such articles published between 2010 and July 2013 equals or exceeds the number appearing between 2000 and 2009. When interpreting Table 2, it is important to remember that the different rows are not mutually exclusive, because any given article might be indexed by one or more theories (see Table 2 footnote on the search strategy); even so, how often a specific theory is indexed is informative. Also of note is the increase in use of the term “epidemiologic theory of disease distribution,” with 16 (70 %) of the 23 articles indexed by this phrase being published since 2000.
Biomedical and Lifestyle
A naïve prediction would be that, on account of their dominance, biomedical and lifestyle articles would garner the lion’s share of citations for articles focused on epidemiologic theory. Table 2 shows this is not the case. The most plausible explanation is that, given their hegemony, the premises of these theories are so ingrained that they need not be the objects of intellectual analysis; they are “simply” the water in which we swim [3••, 14]. Underscoring this point, of the 19 biomedical articles indexed, fully 10 negatively critiqued the “biomedical model,” seven offered a mixed appraisal, and only two were positive.
Social Epidemiology Alternatives
Among the social epidemiology theories, the most commonly indexed were the ecologically-oriented theories (n = 55), followed by the sociopolitical theories (n = 44); fewer were devoted to the psychosocial theories (n = 26). The most frequently indexed specific theory was ecosocial theory (n = 30).
Additional Relevant (or Potentially Relevant) Theories
Also starting in the 1990s, a growing number of articles that explicitly focused on epidemiologic theory were indexed by additional theoretical constructs or by theories external to epidemiology, as shown in Table 2. For each construct and theory listed, in the following text I provide solely one citation (from among the articles included) to serve as an illustration and also as a gateway to the broader literature.
Two commonly employed constructs, sometimes treated as theories, pertain to the epidemiologic transition (n = 28) [37] and lifecourse (n = 19) [38]. As is true for theoretical constructs employed by different theories, how each is elaborated depends on the underlying theory used, e.g., for lifecourse, the discussion of prenatal milieu in relation to “lifestyle choices” (dominant approach) versus ways of living that are facilitated or constrained by, say, racial privilege or discrimination (alternative approach) [3••].
The most common sets of external theories brought into articles on epidemiologic theory were from evolutionary biology (n = 21) [39] and ecology (n = 20) [40]. Next most frequent were articles drawing on theories pertaining to genetics or epigenetics (n = 14) [41] and development (n = 13) [42]. More general scientific theories that were invoked included theories pertaining to complexity or system sciences (n = 10) [43] and to critical realism, albeit less often (n = 4) [44]. Among theories originating in the social sciences, those most frequently deployed with epidemiologic theory were feminist theories (n = 10) [45] and theories of justice (n = 10) [46], followed by critical race theory (n = 5) [47] and intersectionality, a framework arising out of black feminist theory that emphasizes connections between different forms of inequitable social relations (e.g., involving racism, sexism, sexuality, and social class; n = 2) [48]; no articles on epidemiologic theory, however, were indexed by queer theory [49]. Several conceptual papers focused on epidemiologic theory in relation to theoretical systems of indigenous knowledge (n = 6) [50].
Prominence by Field
Considered in relation to field, as also shown in Table 2, a large jump in the 1990s occurred in articles on epidemiologic theory also indexed by “social epidemiology” [51] or by disciplines in the social sciences (overall and by each classic social science) [52]. A similar rise occurred in the 2000s for “population health” [53] and “social determinants of health” [54]. By mid-2013, the respective number of such articles for these four fields equaled 122, 121, 50 and 52. A growing number of books in these fields have also begun to address epidemiologic theory (see Table 2), with the number published since 2000 equaling, if not exceeding, the number of such books published in the prior 50 years [3••, 55].
Interpretation of Trends and Implications
The late 20th c. CE rise of conceptual articles focused on epidemiologic theory, whether in articles or books, is evident across all the theories listed, despite being most prominent among the alternative theories associated with social epidemiology. A reasonable question to ask is: why this trend now?
Four likely reasons exist, two external and one internal to epidemiology as a discipline, and a fourth that bridges these three. The first, and probably most influential, pertains to growing global attention to links between society and health, as reflected by the work of the WHO Global Commission on the Social Determinants of Health [56, 57] and involved in myriad political and policy debates about economic growth, poverty, sustainability, climate change, the Millennium Development Goals, and the framework of “Health in All Policies” [58]. Population distributions of health and their determinants, and hence epidemiologic theory, are central to all of these discussions. Second, in parallel, there is a rising call across the natural and social sciences and the humanities for interdisciplinary, multidisciplinary, and transdisciplinary research—and such work requires, among other things, a clear appraisal of the distinctions and links between the core theories that define these diverse disciplines [3••, 59].
The third reason, internal to epidemiology, is methodological, and arises from developments in the use of explicit causal models (e.g., DAGs) and also analytic techniques such as instrumental variables [60–63]. As increasingly recognized, the ultimate utility of such models and approaches hinges on the quality of reasoning as to the variables included, which in turn depends on the underlying epidemiologic theory leading to specification of the variables and how they might be causally connected [3••, 60, 63].
Finally, the fourth reason, bridging from external into internal, concerns the very basic issue of who does epidemiology. Until well into the 1980s, most students receiving academic training in the USA in epidemiology had, by design or preference, a prior medical degree, such that well into the 1990s, most leaders in the field were imbued with biomedical training; similar trends are apparent in other countries [3••, 64, 65]. The subsequent rise of epidemiologists with training in fields outside of medicine, including the social sciences (in which explicit attention to theory is the norm), thus has made possible a new generation of epidemiologists potentially more versed in—or at least open to—the use of epidemiologic theory. Also likely contributing are post-1980 gains, linked to the long overdue rise of affirmative action programs in the late 1960s and 1970s, in the admission of students from groups previously underrepresented in academic epidemiology (e.g., people of color in the USA, people from the global South, Indigenous people in both the global North and South, along with women in any country context) [3••]; also germane for Latin America is the rise of academics and other health professionals connected to Latin American social medicine who no longer are held back by repressive dictatorships [17, 21, 22, 23••, 66]. Science, after all, is done by real people in real times; as usual, context—and critical mass—matters.
If correct, the four proposed explanations for the recent rise in the explicit analysis and use of epidemiologic theory augur well for the trend to continue. Nothing, however, is guaranteed.
Conclusion: Next Steps for Developing Epidemiologic Theories of Disease Distribution
Consequently, conscious steps are required to develop epidemiologic theories of disease distribution in the 21st c. CE. Needed are both (a) theoretical writings that further flesh out the kinds of causal explanations and predictions these theories envision and how their constructs can be operationalized, and (b) empirical studies, using apt methods, to test the hypotheses generated.
In advocating greater testing of epidemiologic theories in relation to the hypothesis they generate and predictions they make, a caveat is in order. It is one thing to reject a specific hypothesis (assuming the study results are valid); it is another entirely to reject an entire theory. Two considerations are at play. The first, as elegantly argued by Lieberson [67], pertains to the extent to which any given empirical study can test all the conditions under which the theory’s particular hypothesis may or may not hold—with the short answer being, especially in analyses involving complex systems, it cannot [6, 67]. The simplified scenario of any given theory triumphantly being rejected on the basis of one apparently refuted hypothesis, as per the Popperian approach advocated in modern epidemiology texts [68], belies the complexity of scientific theorizing, empirical research, and its interpretation [6, 69]. Relatedly, Kunitz’s recent useful critique of general theories in population health that are inconsistent with empirically observed particular realities [70], requires the further recognition that conflicting particular realities can in fact be consonant with general theories, as long these theories wrestle with historical contingency and the conditions under which their predictions will and will not hold.
More profoundly, exemplified by Longino’s new philosophical work examining scientific pluralism in relation to the scientific study of human behavior [71••], including behaviors that affect health, is a growing appreciation that different theories not only produce partial knowledge but can also lead to incommensurable findings. Whereas partial knowledge can arise because each theory poses questions at different levels (e.g., micro versus macro level phenomena), incommensurable knowledge can result from competing theories differently parsing the relevant “causal space” within the same level(s) [71••, pp.126–129]. For example, as Longino observes, to the extent that “genetic” and “environmental” explanations “apportion variance between genetic and environmental factors, each must put uterine effect into what is for it the alternative category,” such that “the values assignable to G [genetic] or E [environmental] will vary depending on what is included in those categories.” Hence, “correctness must be relativized to the initial parsing of the causal space” [71••, pp. 147–148].
Beyond this, Longino calls attention to a key insight fundamental to epidemiologic theory and inquiry: determinants of differences between populations and variation within populations may often differ [71••, pp.136–137], such that, as Rose iconically argued in his classic 1985 essay “Sick Individuals, Sick Population” [72], asking why populations vary in their rates of disease is not equivalent to asking who is at high risk of disease within a given population [3••, 5, 53]. These distinctions and questions in turn hinge on conceptualizing who and what are “populations” [5]—a complex and contested issue that goes to the heart of epidemiology and kindred disciplines in the population sciences and their respective theories.
What additional steps might help epidemiologic theory to blossom? I’ll propose a few. The first, echoing calls of Latin American epidemiologists [17, 21, 22, 23••], is that there needs to be more conscious global exchange, discussion, and debate about epidemiologic theory. Leading English-language epidemiology textbooks, for example, continue to include little mention of epidemiologic theories [3••, 55], even as such theory is more prominent in diverse Latin American epidemiology textbooks [23, 73]. One welcome sign is that what until now has been the only epidemiologic meeting pulling together the different epidemiology organizations in the USA—the North American Congress of Epidemiology—is en route to becoming, in 2016, the Epidemiology Congress of the Americas, involving epidemiology associations in both North and South America [74]. This expansion builds, in part, upon work done for the 2011 Congress and via related workshops to build better regional ties [75, 76], and also reflects the fast-growing number of epidemiologists in Latin America [77]. Any such dialogue, however, of course must involve more than just epidemiologists of the global North and Latin America. There are likely important insights to be gained, for example, from aspects of more ecologically-attuned and integrative frameworks, as per the classic Hippocratic emphasis on “Airs, Waters, Places” and related forms of “traditional” medicine [3••, 78••], and also from diverse systems of Indigenous knowledge that currently are informing epidemiologic analyses [3••, 34, 50, 79, 80].
Imagine, moreover, if journals that publish epidemiologic research permitted articles that are explicit about theory an additional 250 words and five references regarding their use of theory, as well as a bonus increase of 5 % in total words permitted. Imagine, too, if one of the explicit criteria for grant reviews included the evaluation of explicit use of epidemiologic theory. Both steps, I venture, would increase the quality of epidemiologic thinking and research, as well as provide an incentive for teaching courses on epidemiologic theory. Together, they might make “got theory?” as common a query in epidemiology as the “got milk?” of the iconic US ad campaign [81–83].
In 1995, Tony McMichael warned fellow epidemiologists of the dangers of being “prisoners of the proximate” and called for greater use of what he termed “a social-ecologic systems perspective,” including forecasts regarding possible impacts of “large-scale social and environmental changes,” such as global climate change [84]. The proverb had it right: without vision, the people will perish [1]. The need for epidemiologic theory for understanding and prediction, and for testing causal explanations using rigorous methods and measures, is greater than ever, to improve the odds of generating knowledge that promotes health equity and enables the people’s health – and our planet – to flourish.
References
Papers of particular interest, published recently, have been highlighted as:•• Of major importance
Anon. Prediction and theory in epidemiology. Am J Public Health. 1957;47:1305–7.
"theory, n.2". OED Online. Oxford University Press. 2013. http://www.oed.com.ezp-prod1.hul.harvard.edu/view/Entry/200432?rskey=KVowSx&result=2. Accessed 4 Aug 2013.
Krieger N. Epidemiology and the people’s health: theory and context. New York: Oxford University Press; 2011. Provides in-depth analysis and history of epidemiologic theories of disease distribution, past and present, and concrete examples of why choice of epidemiologic theory matters.
Susser M, Stein Z. Eras in epidemiology: the evolution of ideas. New York: Oxford University Press; 2009.
Krieger N. Who and what are `populations?’ – historical debates, current controversies, and implications for understanding `population health” and rectifying health inequities. Milbank Q. 2012;90:634–81.
Ziman J. Real science: what it is, and what it means. Cambridge: Cambridge University Press; 2004.
The LAM, Fielding H. Garrison Lecture: Ceteris Paribus: the evolution of the clinical trial. Bull Hist Med. 1982;56:1–18.
Oakley A. A historical perspective on the use of randomized trials in social science settings. Crime Delinquency. 2000;46:315–29.
Krieger N. Epidemiology and the web of causation: has anyone seen the spider? Soc Sci Med. 1994;39:887–903.
Krieger N. Epidemiology and social sciences: towards a critical reengagement in the 21st century. Epidemiol Rev. 2000;11:155–63.
Krieger N. Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol. 2001;30:668–77.
Web of science. http://thomsonreuters.com/web-of-science/ Accessed 4 Aug 2013.
PubMed. http://www.ncbi.nlm.nih.gov/pubmed Accessed 4 Aug 2013.
Lock M, Gordon D, editors. Biomedicine examined. Dordrecht: Kluwer Academic Publishers; 1988.
Terris M. The lifestyle approach to prevention: editorial. J Public Health Policy. 1980;1:6–9.
MacMahon B, Pugh TF, Ipsen J. Epidemiologic methods. Boston: Little, Brown & Co; 1960. p. 18–22.
Breilh J. Latin American critical (‘Social’) epidemiology: new settings for an old dream. Int J Epidemiol. 2008;37:745–50.
Engels F. The condition of the working class in England. (Transl: OW Henderson, WH Chalones).Stanford, CA: Stanford University Press; 1958 (originally published: 1848).
Rather LJ, editor. Rudolf Virchow: collected essays on public health and epidemiology, Vol. 1. Canton: Science History Publications; 1988.
Coleman W. Death is a social disease: public health and political economy in early industrial France. Madison: University of Wisconsin Press; 1982.
Tajer D. Latin American Social Medicine: roots, developments during the 1990s, and current challenges. Am J Public Health. 2003;92:2016–20.
Waitzkin H, Iriart C, Estrada A, Lamadrid S. Social medicine then and now: lessons from Latin America. Am J Public Health. 2001;91:1592–601.
Almeida Filho N, Barreto ML. Epidemiologia & saúde – fundamentos, métodos e aplicações. Rio de Janiero: Guanabara Koogan; 2011. Useful example of Latin American epidemiology textbook that incorporates epidemiologic theory.
Gruskin S, Mills EJ, Tarantola D. Health and human rights 1: history, principles, and practice of health and human rights. Lancet. 2007;370:449–55.
Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Social Behav. 2010;51:S28–40.
Elstad JI. The psycho-social perspective on social inequalities in health. In: Bartley M, Blane D, Davey Smith G, editors. The sociology of health inequalities. Oxford: Blackwell; 1998. p. 39–58.
Cannon WB. Stresses and strains of homeostasis. Am J Med Sci. 1935;189:1–14.
Selye H. The general adaptation syndrome and the diseases of adaptation. J Allergy. 1946;17:231-248, 289-323, 358-398.
McEwen B, Wingfield JC. What’s in a name? Integrating homeostasis, allostasis and stress. Hormones Behav. 2010;57:105–11.
Krieger N. Embodiment: a conceptual glossary for epidemiology. J Epidemiol Community Health. 2005;59:350–5.
Krieger N. Proximal, distal, and the politics of causation: what’s level got to do with it? Am J Public Health. 2008;98:221–30.
Krieger N. Methods for the scientific study of discrimination and health: from societal injustice to embodied inequality – an ecosocial approach. Am J Public Health. 2012;102:936–45.
Susser M. Choosing a future for epidemiology: II. From black boxes to Chinese boxes and eco-epidemiology. Am J Public Health. 1996;86:674–7.
Breilh J. Epidemiología crítica: ciencia emancipadora e interculturalidad. Buenos Aires: Lugar Editorial; 2003.
Loewenson R, Hadingham J, Whiteside A. Household impacts of AIDS: using a life course approach to identify effective, poverty-reducing interventions for prevention, treatment, and care. AIDS Care. 2009;21:1032–41.
NIH Research Portfolio Online Reporting Tools (RePORT). http://report.nih.gov/ Accessed 4 Aug 2013.
Weisz G, Olszynko-Gryn J. The theory of epidemiologic transition: the origins of a classic citation. J His Med Allied Sci. 2010;65:287–326.
Kuh D, Ben-Shlomo Y, Lynch J, Hillqvist J, Power C. Life course epidemiology. J Epidemiol Community Health. 2003;57:778–83.
Struchiner CJ, Luz PM, Codeco CT, Massad E. The many faces of epidemiology: evolutionary epidemiology. Cien Saude Colet. 2008;13:1743–52.
Rohani P, King AA. Never mind the length, feel the quality: the impact of long-term epidemiological data sets on theory, application, and policy. Trends Ecol Evol. 2010;25:611–8.
Burris HH, Collins Jr JW. Race and preterm birth – the case for epigenetic inquiry. Ethn Dis. 2010;20:296–9.
Avan BI, Kirkwood BR. Review of the theoretical frameworks for the study of child development within public health and epidemiology. J Epidemiol Community Health. 2010;64:388–93.
Roux AVD. Integrating social and biological factors in health research: a systems view. Annals Epidemiol. 2007;17:569–74.
Patterson M, Johnston J. Theorizing the obesity epidemic: health crisis, moral panic and emerging hybrids. Social Theory Health. 2012;10:265–91.
Inhorn MC, Whittle KL. Feminism meets the “new” epidemiologies: toward an appraisal of antifeminist bias in epidemiological research on women’s health. Soc Sci Med. 2001;53:533–67.
Venkatapuram S, Marmot M. Epidemiology and social justice in light of social determinants of health research. Public Health Ethics. 2009;23:79–89.
Ford CL, Airhikenbuwa CO. The public health critical race methodology: praxis for antiracism research. Soc Sci Med. 2010;71:1390–8.
Dressel P, Minkler M, Yen I. Gender, race, class, and aging: advances and opportunities. Int J Health Services. 1997;27:579–600.
Motta JI, Riberio VM. Who teaches queer: the prospect of queer theory analysis for the health education process. Cien Saude Colet. 2013;18:1695–704.
King M, Smith A, Gracey M. Indigenous health part 2: the underlying causes of the health gap. Lancet. 2009;374:76–85.
Wallerstein NB, Yen IH, Syme SL. Integration of social epidemiology and community-engaged interventions to improve health equity. Am J Public Health. 2010;101:822–30.
Fassin D. Social capital, from sociology to epidemiology: critical analysis of a transfer across disciplines. Rev Epidemiol Sante Publique. 2003;51:403–13.
Pearce N. Epidemiology in a changing world: variation, causation and ubiquitous risk factors. Int J Epidemiol. 2011;40:503–12.
O’Campo P. Are we producing the right kind of actionable evidence for the social determinants of health? J Urban Health. 2012;89:881–93.
Porta M, Vandenbroucke JP, Ionnaidis JPA, Sanz S, Fernandez E, Bhopal R, et al. Trends in citations to books on epidemiological and statistical methods in the biomedical literature. PLoS ONE. 2013;8(5):e61837. doi:10.1371/journal.pone.0061837.
World Health Organization. Closing the gap in a generation: health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva: World Health Organization, 2008.
Solar O, Irwin A. A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2 (Policy and Practice). Geneva: World Health Organization, 2010. http://www.who.int/social_determinants/corner/SDHDP2.pdf. Accessed 4 Aug 2013.
Kickbusch I. Health in all policies. BMJ. 2013;37:f4283. doi:10.1136/bmj.f4283.
Klein JT. Evaluation of interdisciplinary and transdisciplinary research: a literature review. Am J Prev Med. 2008;35:S116–23.
Galea S, Riddle M, Kaplan GA. Causal thinking and complex system approaches in epidemiology. Int J Epidemiol. 2010;39:97–106.
Hernán MA, Cole SR. Invited commentary: causal diagrams and measurement error. Am J Epidemiol. 2009;170:959–62.
Hernán MA, Robins JM. Instruments for causal inference: an epidemiologist’s dream? Epidemiol. 2006;17:360–72.
Robins JM. Data, design, and background knowledge in etiologic inference. Epidemiol. 2001;12:313–20.
Magee JH. A review of the field of epidemiology: current activities and training of practitioners. Washington, DC: Association of Schools of Public Health; 1983.
Olsen J, Saracci R, Trichopolous D, editors. Teaching epidemiology: a guide for teachers in epidemiology, public health, and medicine. 3rd ed. New York: Oxford University Press; 2010.
Laurell AC. What does Latin American social medicine do when it governs? Am J Public Health. 2003;93:2021–4.
Lieberson S. Einstein, Renoir, and Greeley: some thoughts about evidence in sociology. Am Sociol Rev. 1992;57:1–15.
Rothman K, editor. Causal inference. Chestnut Hill: Epidemiology Resources Inc.; 1988.
Susser M. The logic of Sir Karl Popper and the practice of epidemiology. Am J Epidemiol. 1986;124:711–8.
Kunitz SJ. The health of populations: general theories and particular realities. New York: Oxford University Press; 2007.
Longino H. Studying human behavior: how scientists investigate aggression and sexuality. Chicago: University of Chicago Press; 2013. Instructive analysis of scientific pluralism and complementary versus incommensurable findings based on different theoretical approaches routinely used in epidemiologic research.
Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14:32–8.
Breilh J. Epidemiología: economía, medicina y política. 7ma ed. Quito: Universidad Andina Simón Bolívar, Ediciones Abya Yala; 2009. (1st ed: 1979)
International Epidemiologic Association. North American Regional Newsletter, July 2013. http://ieaweb.org/. Accessed 4 Aug 2013.
Symposium on: “Epidemiologic theories for analyzing health inequities: contributions from Latin America and North America -- in global context,” with Birn AE, Krieger N, Barreto ML, and Almeida-Filho N; 3rd North American Congress of Epidemiology, Montreal, Quebec, Canada, June 21-24, 2011. http://ieaweb.org/wp-content/uploads/2012/07/iea-newsletter-june-2011-e.pdf Accessed 4 Aug 2013.
Krieger N, Alegría M, Almeida-Filho N, Jr BdSJ, Barreto ML, Beckfield J, et al. Who, and what, causes health inequities? Reflections on emerging debates from an exploratory Latin American/North American workshop. J Epidemiol Community Health. 2010;64:747–9.
Barreto SM, Miranda JJ, Figueroa JP, Schmidt MI, Munoz S, Kuri-Morales PP, et al. Epidemiology in Latin America and the Caribbean: current situation and challenges. Int J Epidemiol. 2012;41:557–71.
Rosenberg C. Epilogue: airs, waters, places. A status report. Bull Hist Med. 2012;86:661–70. Useful brief analysis and comparison of ancient and current ways of comprehending people’s bodies and population health as necessarily situated, in time and place.
Durie M. Understanding health and illness: research at the interface between science and indigenous knowledge. Int J Epidemiol. 2004;33:1138–43.
Walters KL, Mohammed SA, Evans-Campbell T, Beltran R, Chae DH, Duran B. Bodies don’t just tell stories, they tell histories: embodiment of historical trauma among American Indians and Alaska Natives. Du Bois Rev. 2011;8:179–89.
“Got milk? – milk.zzz.” http://www.milkzzz.com/ Accessed 4 August 2013.
Original “got milk” commercial – Who Shot Alexander Hamilton? http://www.youtube.com/watch?v=OLSsswr6z9Y Accessed 4 Aug 2013.
Vintage Ad Browser. Got Milk Ads. http://www.vintageadbrowser.com/got-milk-ads Accessed 4 Aug 2013.
McMichael AJ. Prisoners of the proximate: loosening the constraints on epidemiology in an age of change. Am J Epidemiol. 1995;149:887–97.
Compliance with Ethics Guidelines
Conflict of Interest
N Krieger declares no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by the author.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Krieger, N. Got Theory? On the 21st c. CE Rise of Explicit use of Epidemiologic Theories of Disease Distribution: A Review and Ecosocial Analysis. Curr Epidemiol Rep 1, 45–56 (2014). https://doi.org/10.1007/s40471-013-0001-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40471-013-0001-1
Keywords
- Biomedical
- Causal inference
- Critical epidemiology
- Ecosocial theory Epidemiology
- Epidemiologic transition Epidemiologic theory
- Epidemiologic theories of disease distribution
- Framework
- Health and human rights
- Health equity
- Health inequities
- Latin American social medicine
- Lifecourse
- Paradigm
- Political economy of health
- Population
- Population health
- Psychosocial
- Social epidemiology
- Social determinants of health
- Social inequalities in health
- Social production of disease
- Theory