
Abstract
Existing evidence suggests that there is a relationship between sensory processing difficulties and the clinical and non-clinical features of autism spectrum disorder (ASD). The current review aimed to evaluate evidence of the psychological correlates of sensory processing patterns in individuals with ASD. Primary studies investigating sensory processing patterns in children and adolescents with ASD were identified through systematic searches of electronic databases and evaluated for methodological rigor and reporting quality. In 21 studies, associations between sensory processing patterns and psychological correlates were found. Sensory hyporesponsiveness was correlated with core features of ASD. Social awareness difficulties and affective disorders were associated with hyperresponsiveness. Mixed results were found for repetitive behaviours. Further research is needed to confirm, clarify and extend these findings.
Similar content being viewed by others

Sensory Atypicalities in ASD
Effective reception, integration and processing of sensory input, as visual, auditory or proprioceptive information, enables us to respond to environmental signals in an adaptive manner (John and Mervis 2010), which is essential to everyday functioning and learning. In autism spectrum disorder (ASD), it has been reported that sensory processing atypicalities are present in over 90 % of children (Leekam et al. 2007) and adults (Crane et al. 2009). Sensory processing difficulties are now included in the most recent diagnostic criteria for ASD (Diagnostic and Statistical Manual of Mental Disorders—5th edition, DSM-V, APA 2013) with ‘hyper- or hyporeactivity to sensory input or unusual interests in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement)’ (APA 2013 p.50) as one of the diagnostic features.
Sensory Processing Patterns in ASD
There are several theoretical approaches to the classification of sensory processing difficulties in ASD. The DSM-V (APA 2013) highlights two sensory processing patterns, hyper- and hyporesponsiveness, understood as exaggerated behavioural reaction and lack of, or insufficient behavioural reaction to, sensory stimuli (Boyd et al. 2009). It has been claimed, for example, that features associated with the hyporesponsiveness pattern can discriminate between children with autism, developmental delay and those of typical development (Baranek et al. 2006). In addition, sensory atypicalities associated with different patterns of sensory processing may be present within the same individual with ASD (Baranek 2002; Baranek et al. 2006; Ben-Sasson et al. 2009). Another approach taken in investigating sensory atypicalities focuses on sensory modulation disorder (SMD). SMD is characterised by difficulties in regulating and organising appropriate behavioural responses to sensory input (Miller et al. 2007). The disorder has distinct three subtypes—overresponsivity, underresponsivity and sensory seeking associated with the craving of sensory experience (Miller et al. 2007). This classification system has been acknowledged by the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood, Revised (known as the DC: 0–3R) (Zero to Three 2005), the Diagnostic Manual for Infancy and Early Childhood of the Interdisciplinary Council on Developmental and Learning Disorders (ICDL 2005), and the Psychodynamic Diagnostic Manual (PDM Task Force 2006). Other researchers examine sensory difficulties in ASD by applying Dunn’s model of sensory processing (Dunn 1997). In that approach, hyper- and hyporesponsiveness are further divided depending on whether passive and active self-responding strategies are used to respond to sensory stimulation. As a result, four patterns of sensory processing are distinguished: Low Registration, Sensation Seeking, Sensory Sensitivity and Sensation Avoiding. All four sensory processing patterns have been reported as present in individuals with ASD (Kern et al. 2007). These multiple theoretical stands present in investigating sensory processing atypicalities in ASD are reflected in the current literature.
Symptom Comorbidity
Research suggests that there is a relationship between sensory processing difficulties and the clinical features of ASD. Some studies reported significant associations between sensory processing atypicalities, communication and social impairments (Watson et al. 2011) as well as repetitive behaviours (Boyd et al. 2009), the presence of maladaptive behaviours, antisocial behaviours, self-absorption and parent-reported child anxiety (Baker et al. 2008) or perseveration and overfocusing attention (Liss et al. 2006). There is also evidence of significant associations between sensory processing atypicalities and other non-clinical psychological constructs such as temperament (Brock et al. 2012), emotion dysregulation (Samson et al. 2013) or eating difficulties (Nadon et al. 2011). However, there is variability in the methodological approaches used in those studies, including the selection of measures, diagnostic subgroups and specified inclusion criteria. Due to a vast number of psychological constructs that have been investigated, and a wide range of methods of investigation employed, both interpretation and comparison of findings has been hampered.
Previous Reviews
Four literature reviews of sensory atypicalities in individuals with ASD have been published to date (Ben-Sasson et al. 2009; Iarocci and McDonald 2006; O’Neill and Jones 1997; Rogers and Ozonoff 2005). However, these evaluations focused on differently defined sensory difficulties: Ben-Sasson et al. (2009) reviewed sensory modulation symptoms in individuals with autism, Iarocci and McDonald (2006) investigated multisensory integration, O’Neill and Jones (1997) studied unusual sensory responses, while Rogers and Ozonoff (2005) concentrated on sensory dysfunction. Secondly, the previous reviews employed different methodological approaches, ranging from experimental laboratory findings combined with theoretical and conceptual papers (Iarocci and McDonald 2006; Rogers and Ozonoff 2005), through reviewing clinical and experimental studies (O’Neill and Jones 1997) to the inclusion of only clinical findings (Ben-Sasson et al. 2009). Thirdly, the previous reviews focused more on the discriminant validity of sensory atypicalities between ASD and typical groups. There is also growing number of studies investigating physiological reactivity to different types of sensory stimuli (for review see Lydon et al. 2014). However, none of the published reviews have described evidence of associations between sensory processing patterns in individuals with ASD and other psychological constructs. Therefore, this current approach to the review is important because, while there is growing interest and research in sensory processing in individuals with ASD and sensory processing patterns are included in the diagnostic criteria for ASD (APA 2013), a systematic summary of the recent findings is lacking.
Aim of the Review
The current review therefore aims to systematically summarise and evaluate available evidence, recognise and discuss any shortcomings, and identify goals for future research in order to address the following question: What are the psychological correlates of sensory processing patterns in individuals with ASD?
Method
Inclusion/ Exclusion Criteria
Inclusion and exclusion criteria were defined prior to conducting the literature search. Studies were eligible for inclusion if they investigated sensory processing patterns in individuals with ASD and explicitly reported associations with psychological correlates such as cognition, emotions, behaviour or interpersonal relationships. Studies were searched from 1997 onwards. Non-primary studies were excluded from the search (e.g. reviews, book chapters). Also, single case studies and case series designs were excluded. This decision was based upon the consideration that results from single case studies would not provide quantitative statistical data which is important from the point of this review and do not allow further generalisation of the findings. The search was neither restricted to any particular age group nor particular diagnostic subgroup.
Search Strategy
A systematic literature search aimed to identify studies reporting sensory processing patterns of individuals with ASD conducted up to February 2014. The search used five electronic databases: Scopus, Web of Knowledge, PsychInfo, Embase and Medline. For both Scopus and Web of Knowledge, which allow authors to search for a number of keywords, the search terms were based on the keywords used in the Ben-Sasson et al. (2009) meta-analysis. After identifying relevant papers, additional keywords that were used in categorising those papers were added into the search terms. The combinations of the following search terms were used: a diagnostic term (autis* or “pervasive developmental disorder*” or Asperger), a sensory term (sensory or reactivity or responsivity or sensation*) and a descriptor term (processing or integration or modulation or regulation or stimul* or input or event* or dysfunction or respons* or profile* or symptom* or unusual or difficulties or interest* or feature* or experience* or hypo* or hyper* or pattern* or sensitiv* or seeking or avoid* or registration or threshold* or defensiveness). In PsychInfo, Embase and Medline databases, searches are based on controlled vocabularies. However, because different types of headings are used for each database (e.g. medical subjects headings for Medline, but APA thesaurus for PsychInfo), the vocabulary used in the databases varied. For PsychInfo, autism or pervasive developmental disorders or Asperger syndrome were used as diagnostic terms, combined with sensory integration or intersensory processes or perceptual motor processes or sensorimotor measures or sensory adaptation or adaptation or thresholds or self stimulation. In the Embase database, Asperger syndrome or infantile autism or autism terms were used, combined with sensory dysfunction or abnormal sensation or sensory defensiveness or sensory stimulation or sensation or abnormal sensation or sensation seeking or self stimulation or perceptive threshold or sensorimotor function or sensorimotor integration. When searching in Medline, a combination of terms child development disorders, pervasive or autistic disorder or Asperger syndrome, and sensory thresholds or sensation disorders or self stimulation or occupational therapy were used.
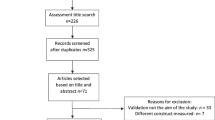
A flowchart of the search strategy and numbers of articles identified and excluded at each stage is outlined in Fig. 1. All databases were searched between 1997 and the 2nd of February 2014.

Flowchart of search
Electronic Search
Results from five electronic databases were exported to Endnote® referencing software resulting in 3336 records in total. Most duplicates of the papers were identified by Endnote’s duplicate identification function and removed from the records’ list. Further duplicates not recognised by the software were removed manually, and 1964 records were carried forward to the screening stage.
Screening of Electronic Search Results
Screening of the search results consisted of four main phases. In phase 1, the non-primary sources were electronically identified and removed (a total of 99 records). In phase 2, the remaining titles of the records were screened considering their relevance to the search question and 1441 studies were removed. In phase 3, remaining article abstracts were screened. Only 90 met inclusion criteria and those were carried forward to the final phase in which articles were screened by full text and the final selection was made.
Final Selection
Sixty nine papers were excluded after screening the full text. Five papers were excluded due to unpublished status (three theses, two conference papers). Four were excluded due to being published in languages other than English (Japanese, Italian, Portuguese and Chinese). Four papers focused on sensory modalities (such as auditory or tactile modality) rather than sensory patterns, which were a main interest of this review. In another 27 papers, sensory atypicalities in general were investigated (mainly reporting the Short Sensory Profile total score). Four studies used physiological measures of sensory processing. Nine papers were not found appropriate due to the lack of correlational analysis (four were descriptive in nature, reporting, for example, cross-group comparisons and another five presented only means for different constructs, without reporting relations between the constructs or presenting sensory clusters). Seven papers did not include any psychological constructs, but examined relationships between sensory processing and for example oral care difficulties, leisure activities, or family life impairment and maternal parenting stress. Two papers were validity studies (investigating psychometric properties of tools). In seven papers, a clear ASD sample was not recruited, either studies included participants from the general population, with or without some ASD-traits, or the results were presented for a combined ASD sample with another group (e.g. developmental delay). The remaining 21 papers were included in the systematic review. The summary of the descriptive characteristics of these studies can be found in Table 1.
Critical Evaluation
Each of the retained papers was evaluated against a review quality evaluation grid developed for the purpose of this review. The available checklists for the quality assessment of studies (e.g. PRISMA, Moher et al. 2009; QUADAS, Whiting et al. 2003) or well-known guidelines for conducting systematic reviews in health care (e.g. the Cochrane Collaboration) focus on diagnostic accuracy, evaluation of randomised trials and intervention studies. The newly developed grid aimed to systematically evaluate the overall quality of the studies, their strengths and limitations or potential sources of bias. The grid was divided into four main sections, following the IMRaD structure: introduction, methods, results and discussion (Sollaci and Pereira 2004). The methods section was of particular importance including items evaluating a studies quality in participants and method selection. To adequately evaluate the methodology used in the studies, the grid contained items concentrating on appropriate sample characteristics and confirmation of ASD diagnosis. The methods section of the evaluation grid also highlighted the importance of sound psychometric properties of the tools used in the studies as suggested by the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) guideline (Mokkink et al. 2010). The total number of criteria that the studies were scored against was kept within the recommended limit to keep clear focus of the review (SIGN 2008).
Subjective judgement is a part of the evaluation process (Deeks et al. 2003; SIGN 2008); to minimise the reviewer’s subjectivity, the following steps were undertaken. First, all scoring criteria were explained in detail. Second, three levels of quality ratings were used, the equivalent of the levels of ratings proposed by SIGN (high, acceptable and low quality). Finally, a proportion of the studies included in the review (19 %) were evaluated by an independent rater. The inter-rater reliability between the author’s and independent rater’s scorings calculated as percentage agreement on individual criteria was 87.5 %.
Results
Of the 1964 unique references identified via the electronic searches, 21 papers met the inclusion criteria and were retained for review.
Evaluation Grid—Papers’ Quality
Originally, the papers included in the review were scored against 26 criteria. Ten criteria were emphasised during the evaluation. Two criteria were selected from the participants’ section (‘Was ASD diagnosis confirmed for the study?’ and ‘Is the sample adequately described?’). They allowed us to assess whether the sample of interest was included in the study and whether the authors reported participants’ characteristics in a high-quality manner. Items from the ‘Sensory measures’ and ‘Psychological correlate measure’ sections were also considered as the criteria of the key importance. They allowed us to evaluate the appropriateness, reliability and validity of the tools used in the studies. The chosen criteria are fundamental to evaluate the quality of the studies in the light of the research question asked in this review. For the summary of the information included in the evaluation grid and ten selected criteria, see Table 2.
Participants’ Section
The two items describing participants’ characteristics are essential to establish whether the particular clinical group of interest was selected according to widely accepted research standards. In addition, it was important to confirm whether or not the characteristics were described well enough to allow other researchers to replicate the study and identify some possible important covariates that might influence the study findings. All the studies provided a confirmation of diagnosis of participants. In 14 papers, the assessment of children was carried out prior to inclusion in the study by using ‘gold-standard’ diagnostic tools such as the Autism Diagnostic Observation Schedule (ADOS) or the Autism Diagnostic Interview-Revised (ADI-R). In the remaining seven papers (Ashburner et al. 2008; Gal et al. 2010; Hilton et al. 2007; Lane et al. 2012; Liss et al. 2006; Nadon et al. 2011; Tseng et al. 2011), documents stating children’s and young people’s diagnosis were gathered or non-‘gold-standard’ tools were used to confirm diagnosis, e.g. medical chart review. However, sample characteristics were not always well described. Three studies (Lane et al. 2012; Liss et al. 2006; Tseng et al. 2011) reported only gender and age of their participants. Only Nadon et al. (2011) provided all the demographics selected in the evaluation grid characteristics (e.g. age, gender, ASD subtype, comorbidities and demographic variables). The remaining studies reported three or four of these features.
Sensory Measures Section
Nine different tools were used to assess sensory processing pattern or patterns in the selected studies (additionally the Sensory Profile was used in two language versions—English and Chinese). Three authors (Boyd et al. 2010; Brock et al. 2012; Watson et al. 2011) used more than one sensory measure and selected items from each measure to inform a factor analytic model of sensory processing patterns. These models were informed with both observational data and parent reports, and in both studies further confirmatory factor analysis was performed to ensure appropriate model fit to the data (in Table 3, information on each measure separately rather than the final models can be found). Pfeiffer et al. (2005) used two measures depending on the age of their participants and Lane et al. (2012) used two tools, reporting their outcomes as equivalent to each other. Hence, overall there were ten different sensory measures used across the 21 selected papers (with 38 tool’s references in total), with the Sensory Profile and Short Sensory Profile being used most frequently.
In eight studies, there was information about a sensory measure being standardised (Gal et al. 2010; Jasmin et al. 2009; Lane et al. 2010, 2012; Nadon et al. 2011; Pfeiffer et al. 2005; Reynolds et al. 2012; Watson et al. 2011) with Liss et al. (2006) providing a reference to a current standardisation work. Remaining studies did not report on the measures’ standardisation. Reliability was more often reported than validity of the measures, with three studies providing calculations of reliability—test-retest reliability (Baranek et al. 2013) and internal consistency (Green et al. 2012; Pfeiffer et al. 2005, but only for the Adolescent/Adult Sensory Profile, AASP). Only Pfeiffer et al. (2005) provided discriminative and convergent validity calculations (for the AASP). Across the papers included in the review, there was no information regarding reliability of nine of the referenced tools used compared to 14 measures missing information on validity. Across the studies, four measures were referenced as being appropriate for use with ASD population or being ASD specific (Sensory Processing Assessment, SPA; Tactile Defensiveness and Discrimination Test, TDDT-R; Sensory Experiences Questionnaire, SEQ; and Sensory Questionnaire, SQ). Sensory Profile and Short Sensory Profile, in four and three studies, respectively, were reported as widely used within the ASD research.
Psychological Correlate Measure Section
Thirty one different measures of psychological correlates were used in the reviewed papers. Some of the tools were used in several publications, Child Behavior Checklist (CBCL) was used in two language versions—English and Chinese, and Vineland Adaptive Behaviour Scales were used in their original version and newest revision (VABS and VABS-2), resulting in 37 references to psychological correlate measures across selected papers. Only in six papers (Hilton et al. 2007; Lane et al. 2010; Lidstone et al. 2014; Mazurek et al. 2013; Pfeiffer et al. 2005; Watson et al. 2011) some measures were reported as standardised (SRS, VABS, SCAS-P, PAS, CBCL, ABAS, MSEL and PLS-4). The remaining papers did not indicate standardisation status of the tools used. In Liss et al. (2006), a tool measuring exceptional memory was used; however, no information on tool development, measurement properties or scoring criteria was given. Reliability calculations were performed for four tools: inter-rater reliability for the JAA (Baranek et al. 2013), RBQ-2 (Lidstone et al. 2014), EDI (Samson et al. 2013) and test-retest for Eating Profile (Nadon et al. 2011). Structural validity was only calculated for the RBQ-2 in Lidstone et al. (2014) and face validity for Eating Profile in Nadon et al. (2011). Across the reviewed studies, there was no information about the reliability of the 13 referenced measures and about the validity of 14 selected tools. Across the studies, seven measures were referenced as being appropriate for use with ASD population or being ASD specific (GARS, GADS, GI SIQ, Eating Profile, ADOS, RBS-R and SRS), and further five were reported as widely used in ASD research or developmental disorders (JAA, EFT, VABS, KOS, CBCL).
Results—Associations
The authors selected different sensory patterns for their investigation. Hyporesponsiveness was examined in Baranek et al. (2013); hyperresponsiveness in Green et al. (2012), Lane et al. (2012) and Mazurek et al. (2013); hypo-, hyperresponsiveness and sensation seeking in Boyd et al. (2010), Brock et al. (2012) and Watson et al. (2011); a pattern combining underresponsiveness and sensation seeking in Ashburner et al. (2008), Baker et al.(2008), Chen et al. (2009), Gal et al. (2010), Lane et al. (2010), Nadon et al. (2011) and Samson et al. (2013); and sensory processing patterns from Dunn’s model in Hilton et al. (2007), Jasmin et al. (2009), Lidstone et al. (2014), Reynolds et al. (2012) and Tseng et al. (2011). Liss et al. (2006) used terms sensory seeking and over- and under-reactivity, which were treated as synonyms of hyper- and hyporesponsiveness. Pfeiffer et al. (2005) examined hypo- and hypersensitivity which were treated same as hypo- and hyperresponsiveness. Some authors preferred using responsiveness, some responsivity—both were also treated as synonyms in this review.
In 12 papers (Baranek et al. 2013; Boyd et al. 2010; Brock et al. 2012; Gal et al. 2010; Green et al. 2012; Hilton et al. 2007; Lane et al. 2010, 2012; Liss et al. 2006; Nadon et al. 2011; Reynolds et al. 2012; Samson et al. 2013), investigation of associations between sensory processing patterns and a single psychological construct was carried out. Three of these papers have multiple hypotheses on the sub-constructs of the phenomenon under investigation that were tested. Baranek et al. (2013) looked at joint attention and reported the results for both initiation of and response to joint attention. Brock et al. (2012) were interested in sensory patterns’ association with several dimensions of temperament such as withdrawal, distractibility, persistence or slowness to adapt, and in Liss et al. (2006) the concept of overarousal was characterised by overfocused behaviour, perseverative preoccupation and exceptional memory for self-selected material. In the remaining studies, the relationship between sensory processing atypicalities and two (Baker et al. 2008; Chen et al. 2009; Jasmin et al. 2009; Lidstone et al. 2014; Mazurek et al. 2013; Tseng et al. 2011; Watson et al. 2011) or more (Ashburner et al. 2008; Pfeiffer et al. 2005) constructs were explored. Data extraction was carried out for each construct separately and for this reason those papers investigating multiple constructs were included in the review results’ sections more than once.
Participants
Across the 21 studies included in the review, a total of 4149 children and adolescents with ASD were included. One study recruited 2973 participants (Mazurek et al. 2013); the remaining studies involved between 22 and 149 participants.
The age of participants ranged from 20 months to 17 years (overall mean age = 7.09 years). One study focussed particularly on toddlers (Green et al. 2012; with a mean of 28.2 months). Nine studies (Baker et al. 2008; Baranek et al. 2013; Boyd et al. 2010; Brock et al. 2012; Jasmin et al. 2009; Lane et al. 2010; Nadon et al. 2011; Tseng et al. 2011; Watson et al. 2011) focussed on early and middle childhood (20 to 115 months). A further nine studies (Ashburner et al. 2008; Chen et al. 2009; Gal et al. 2010; Hilton et al. 2007; Lane et al. 2012; Liss et al. 2006; Pfeiffer et al. 2005; Reynolds et al. 2012; Samson et al. 2013) included children and adolescents between middle childhood and mid-teens (6 to 17 years). Two studies included both children and adolescents; Lidstone et al. (2014) recruited 3–17-;9-year-old participants and Mazurek et al.(2013) used a sample between 2 and 17 years old.
In all the studies, the gender of the participants was reported and 84.3 % of participants were male. This percentage mirrors the widely reported uneven sex ratio for the prevalence of ASD in males, with males being four times more likely of having this condition than females (Anello et al. 2009).
A minority of studies were highly selective when recruiting participants with a particular diagnosis. Pfeiffer et al. (2005) included only children and adolescents who had Asperger’s syndrome, while Hilton et al. (2007) included only children with High Functioning ASD. Four studies included participants across the spectrum. Chen et al. (2009) included those with a diagnosis of ASD or Asperger’s syndrome; Green et al. (2012) recruited toddlers with either autism or PDD-NOS; Jasmin et al. (2009) included in their study children with AD or PDD-NOS. In a couple of studies, participants were characterised as diagnosed with autism (Tseng et al. 2011; Gal et al. 2010) and further five (Baker et al. 2008; Baranek et al. 2013; Boyd et al. 2010; Lane et al. 2010; Watson et al. 2011) included those with autistic disorder. In the remaining studies, participants fell into the general diagnostic category for ASD. Only Mazurek et al. (2013) and Nadon et al. (2011) reported an exact percentage of ASD children in each diagnostic category (AD, Asperger’s disorder, PDD-NOS).
The method of reporting cognitive ability varied markedly across the reviewed studies. Ability in the form of an IQ score was reported by Lane et al. (2012), Reynolds et al. (2012) and Samson et al. (2013), with the following means (standard deviations): 95.5 (18), 95.88 (17.8) and 82.75 (23.61), respectively. Standard score of 61.3 (26.5) was reported in Jasmin et al. (2009). Green et al. (2012) stated non-verbal and verbal developmental functioning (78.1 (18.06) and 58.62 (25.15)) of their participants, whereas Baranek et al. (2013), Boyd et al. (2010), Brock et al. (2012) and Watson et al. (2011) reported mental age (23.25 (14.04), 31.97 (20.84), 36.11 (19.88) and 32.0 (20.6), respectively). Ashburner et al. (2008) included only participants with IQ above 80, while Chen et al. (2009) and Hilton et al. (2007) included individuals with ASD with IQ above 70. Mazurek et al. (2013) reported that 3.9 % of their sample had an IQ lower than 70, while the remaining sample had IQ above 70. Remaining authors did not provide any indicators of cognitive functioning of their participants.
Only two studies reported co-occurring medical conditions for their participants. Nadon et al. (2011) reported attention deficit disorder, hyperactivity and mental retardation as the most common co-occurring conditions, while in Hilton et al. (2007) attention deficit/hyperactivity disorder, learning disability, anxiety disorder, depression and Tourette syndrome were reported as additional diagnoses.
Psychological Constructs
In the selected studies, the authors examined relationships between sensory processing patterns and a variety of psychological constructs. In order to present our findings in a systematic way, the papers have been grouped. In the most recent Diagnostic and Statistical Manuals of Mental Disorders, core features of ASD, such as impairments in the social use of both non-verbal and verbal communication and presence of restricted, repetitive patterns of behaviour, interests or activities, are diagnostic components for the disorder (APA 2013). In addition to these core features that are present in individuals with ASD, a number of associated difficulties have been listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; APA 2000); these include emotional, attentional, cognitive and behavioural problems. The psychological constructs examined in the selected papers have been grouped accordingly, either belonging to the core features of ASD, such as social functioning and repetitive behaviours, or characterised as associated conditions of ASD, e.g. affective and cognitive difficulties. As a result, six main groups of psychological constructs were created: symptom severity, social functioning, restricted and repetitive behaviours, emotional and behavioural functioning, affective and cognitive symptoms, and physical skills.
In the identified groups, the following constructs were included (as indicated by the authors):
-
symptom severity: social communicative symptoms (Watson et al. 2011), social competence (Hilton et al. 2007), social symptoms/communication impairment (Liss et al. 2006), autism quotient and Asperger’s disorder quotient (Ashburner et al. 2008);
-
social functioning: language skills (Watson et al. 2011), language abilities (Baranek et al. 2013), social and communication adaptive skills (Watson et al. 2011) and joint attention (Baranek et al. 2013);
-
restricted and repetitive behaviours: restricted and repetitive behaviours (Chen et al. 2009; Boyd et al. 2010; Lidstone et al. 2014) and stereotyped movement (Gal et al. 2010);
-
emotional and behavioural functioning: emotional, behavioural and educational outcomes (Ashburner et al. 2008), emotional and behavioural problems (Tseng et al. 2011), emotion dysregulation (Samson et al. 2013), adaptive/maladaptive functioning (Baker et al. 2008; Lane et al. 2010; Liss et al. 2006; Pfeiffer et al. 2005), behavioural responsiveness (Baker et al. 2008), gastrointestinal problems (Mazurek et al. 2013), eating (Nadon et al. 2011) and sleep (Reynolds et al. 2012) problems;
-
affective and cognitive symptoms:
-
physical skills: motor skills (Jasmin et al. 2009) and daily living skills (Jasmin et al. 2009).
Symptom Severity
Four papers investigated associations between sensory atypicalities and symptom severity. Ashburner et al. (2008) found a significant negative correlation between the underresponsive/seeks sensation subscale of the Short Sensory Profile and GARS autism quotient (r = −0.53 p = 0.003), but not with GADS Asperger’s disorder quotient, suggesting more sensory problems being associated with more autism symptoms (low score on the SSP indicates more sensory issues). Hilton et al. (2007) reported significant associations between all sensory processing patterns as measured by the Sensory Profile and SRS scores, both total score (correlations with Sensory Sensitivity, r = −0.745, p < 0.01; Sensory Avoiding, r = −0.796, p < 0.01; Low Registration, r = −0.578, p < 0.01; and Sensation Seeking, r = −0.527, p < 0.01) and subscales, with the exception of SRS social awareness for which only sensory sensitivity and sensation avoiding were found to be negatively correlated. Liss et al. (2006) found significant correlations between overreactivity, underreactivity and sensation seeking and all the subscales of DSM-IV checklist. Only the DSM-IV communication impairment subscale was not significantly associated with overreactivity. Watson et al. (2011) used ADOS as one of the outcome measures in their study and found associations between social-communicative algorithm scores and both hyporesponsiveness (β = 0.48, SE = 0.023, p = 0.040) and sensation seeking (β = 0.78, SE = 0.025, p = 0.002).
Social Functioning/Social Skills
The relationship between sensory processing patterns and verbal and non-verbal communication skills in individuals with ASD was investigated in two studies. Baranek et al. (2013) were interested in associations between sensory difficulties and language abilities and joint attention. Watson et al. (2011) explored the relationships between sensory atypicalities and language skills, social and communication adaptive skills. All verbal and non-verbal variables were associated with sensory hyporesponsiveness (Receptive language ratio scores, β = −2.0, SE = 0.68, p = 0.004; Expressive language ratio scores, β = −2.1, SE = 0.73, p = 0.005; Receptive Joint Attention, β = −0.83, SE = 0.37, p = 0.025; Initiating Joint Attention, β = −1.63, SE = 0.59, p = 0.006; Aggregate language quotient scores, β = −0.010, SE = 0.004, p = 0.018; Social adaptive scores, β = −0.017, SE = 0.007, p = 0.011). Also in Watson et al. (2011) language skills (aggregate language quotient scores) were correlated with sensory seeking (β = −0.011, SE = 0.004, p = 0.005).
Restricted and Repetitive Behaviours (RRBs)
Restricted and repetitive behaviours (RRBs) is a broad term which includes behaviours ranging from self-injurious behaviour and stereotyped motor mannerisms through insistence on sameness and circumscribed interests (Bodfish et al. 2000). Turner (1999) suggested distinguishing two levels of behaviours—‘lower level’ including motor repetitions and stereotyped behaviours, and ‘higher level’ relating to insistence on sameness and circumscribed interests. This division of RRBs into two separate levels is present in the studies included in our review, hence we present the results distinguishing between ‘lower’ and ‘higher’ levels of RRBs.
Four papers looked at the relationship between sensory processing patterns and the presence of restricted and repetitive behaviours. Boyd et al. (2010) reported a significant association between hyperresponsiveness and stereotypy (β = 3.40, SE = 1.35, p = 0.012). Gal et al. (2010) found a significant negative correlation between the number of Different Stereotyped Movements and the underresponsiveness/seeks sensation subscale of Short Sensory Profile (r = −0.43, p < 0.001). Lidstone et al. (2014) reported significant negative correlations between repetitive motor behaviours and sensation avoiding and sensation seeking (r = −0.42, p < 0.01 for both). In the same study, significant negative correlations were found between all sensory processing patterns and insistence of sameness (correlations with Sensory Sensitivity, r = −0.43, p < 0.01; Sensory Avoiding, r = −0.49, p < 0.01; Low Registration, r = −0.38, p < .01; and Sensation Seeking, r = −0.49, p < 0.01). Chen et al. (2009), however, did not find any associations between underresponsiveness/seeks sensation patterns and ‘compulsive-like behaviours’. Compulsions were associated with hyperresponsiveness in Boyd et al. (2010) study (β = 3.50, SE = 1.41, p = 0.013). The authors found also significant associations between rituals and both hyperresponsiveness (β = 4.47, SE = 1.35, p = 0.001) and sensory seeking (β = 5.92, SE = 2.97, p = 0.046).
Emotional and Behavioural Functioning
Seven papers examined associations between sensory difficulties and the emotional and behavioural functioning of individuals with ASD. Ashburner et al. (2008) reported significant correlations between the underresponsive/seeks sensation subscale of the Short Sensory Profile and three subscales of Conner’s Teacher Rating Scale–Revised Long Version, cognitive problems/inattention (r = −0.48, p < 0.01), social problems (r = −0.32, p < 0.05) and inattentive (r = −0.42, p < 0.05). They also found significant associations of the Short Sensory Profile underresponsiveness/seeks sensation subscale and two of the subscales of the Achenbach System of Empirically Based Assessment: Teacher Report Form, namely thought problems (r = −0.39, p < 0.05) and academic performance (r = 0.62, p < 0.01). Baker et al. (2008) using the Short Sensory Profile reported correlations with the following subscales of the Developmental Behaviour Checklist subscales: self-absorbed (r = −0.523, p = 0.012), Autism Screening Algorithm (r = −0.533, p = 0.011) and total score (r = −0.491, p = 0.020); and maladaptive behaviour scale of Vineland Adaptive Behaviour Scales (r = −0.482, p = 0.023). Lane et al. (2010) also found similar associations with the maladaptive behaviour scale of the VABS. Using the VABS, Liss et al. (2006) reported correlations between the socialisation subscale and hyperresponsiveness (r = −0.195, p < 0.05), VABS daily living and adaptive behaviour composites and hyporesponsiveness (r = −0.326, p < 0.01 and r = −0.221, p < 0.01, respectively) and sensory seeking with the VABS communication (r = −0.263, p < 0.01), daily living (r = −0.165, p < 0.05) and adaptive behaviour composite (r = −0.235, p < 0.01). Pfeiffer et al. (2005) investigated relationships between sensory processing patterns and adaptive behaviours. They found significant negative associations between both hypo- and hypersensitivity and community use (r = −0.271, p = 0.05 and r = −0.291, p = 0.041, respectively) and social skills subscales of the Adaptive Behavior Assessment System (r = −0.298, p = 0.036 and r = −0.278, p = 0.05, respectively). Samson et al. (2013) looked at emotion dysregulation and its relationship with sensory atypicalities, reporting higher emotion regulation difficulties in those individuals with ASD who also had high scores on the underresponsive/seeks sensation subscale of the SSP (r = −0.57, p < 0.001). Tseng et al. (2011) were interested in sensory processing dysfunction and children’s emotional and behavioural problems. They used the Child Behavior Checklist to measure both internalising and externalising difficulties and found a number of significant associations of those dimensions with all the sensory processing patterns. Internalising was negatively associated with Sensory Sensitivity: r = −0.24, p = 0.047, Sensory Avoiding: r = −0.43, p < 0.001, Low Registration: r = −0.28, p = 0.020 and Sensation Seeking: r = −0.43, p < 0.001, while externalising correlated significantly with Sensory Sensitivity: r = −0.30, p = 0.013, Sensory Avoiding: r = −0.29, p = 0.016 and Sensation Seeking: r = −0.29, p = 0.016.
The relationship between associated behavioural problems with ASD and sensory processing difficulties was investigated in three studies. Mazurek et al. (2013) reported that those children with ASD who had chronic GI problems such as chronic constipation, chronic abdominal pain, chronic bloating, chronic nausea and chronic diarrhoea had significantly lower sensory overresponsivity scores (greater levels of overresponsivity) than those children with ASD who had no additional GI problems (d = −0.36 to −0.71, p < 0.0001). Nadon et al. (2011) did not find any significant associations between underresponsive/ seeks sensation subscale of the Short Sensory Profile and the mean number of eating problems in children with ASD. Reynolds et al. (2012) reported significant positive correlation between sensation avoiding and sleep problems (r = 0.502, p = 0.11); associations with other sensory processing patterns were not significant.
Affective and Cognitive Difficulties
Affective Symptoms
Six papers investigated the relationships between sensory processing patterns and affective symptoms such as dimensions of temperament, anxiety and depression. Brock et al. (2012) looked at how sensory atypicalities relate to temperament dimensions in children with ASD. Three out of the nine investigated dimensions were associated with only one particular pattern, namely hyporesponsiveness (adaptability, β = 0.38, p = 0.001; distractibility, β = −0.46, p < 0.0001; reactivity, β = −0.28, p = 0.04), reporting that children with ASD who show hyporesponsive behaviours may be more susceptible to various distractions and their optimal level of engagement with the environment may be narrower, elongating adjustment to change. In all five papers in which the relationship between anxiety and sensory patterns was examined (Green et al. 2012; Lane et al. 2012; Lidstone et al. 2014; Mazurek et al. 2013; Pfeiffer et al. 2005), correlations between hyperresponsiveness and anxiety were found and reported by four authors although a number of different measures were used across the studies (Green et al. 2012: r = 0.52, p < 0.001 (time 1) and r = 0.60, p < 0.001 (time 2); Lane et al. 2012: r = 0.18, p < 0.001; Mazurek et al. 2013: r = −0.45, p < 0.0001; Pfeiffer et al. 2005:r = 0.476, p < 0.001). Lidstone et al. (2014) looked at dimensions of hyperresponsiveness (both sensory sensitivity and sensation avoiding), and further moderate to strong correlations were reported (r = −0.61, p < 0.01 and r = −0.71, p < 0.01, respectively). Only Lidstone et al. (2014) stated a relationship between anxiety and low registration (r = −0.40, p < 0.01). Depression was associated with hyperresponsiveness (r = 0.394, p = 0.005 for the total sample, and for the younger children r = 0.449, p = 0.013, but not for the teenage group) as reported by Pfeiffer et al. (2005), but also with hyporesponsiveness (r = 0.214, p = 0.05 for the total sample, non-significant associations for the younger children and significant for the teenagers, r = 0.492, p = 0.027) and hyporesponsiveness dimensions (low registration was significantly associated with depression only in the teenage group r = 0.483, p = 0.031, and sensation seeking correlated with depression when the total sample was used r = 0.299, p = 0.035).
Cognitive Symptoms
The relationship between cognitive functioning and sensory abnormalities in children with ASD was examined in two studies. Chen et al. (2009) were interested in exploring the relationship between sensory difficulties and an individual’s detail-focused cognitive style. Only non-significant associations between the under responsive/seeks sensation subscale of the Short Sensory Profile and the Embedded Figure Test were reported. Liss et al. (2006) looked at both ability to shift attentional focus and exceptional memory for self-selected material in individuals with ASD. They showed that although underreactivity and sensory seeking were significantly correlated with Kinsbourne Overfocusing Scale (r = 0.293, p < 0.01 and r = 0.235, p < 0.01, respectively), the strongest positive correlation was found with overreactivity (r = 0.608, p < 0.01). Overreactivity was also negatively correlated with the reverse log of the exceptional memory score (r = −0.196, p < 0.05), showing an association between greater exceptional memory and individual’s overreactivity to sensory stimuli.
Physical Skills
Only one study investigated the relationship between sensory processing patterns and motor skills with daily living skills (as self-care skills) in children with ASD. Jasmin et al. (2009) reported significant correlations between only one sensory pattern, namely sensation avoiding and self-care domain of the WeeFIM (r = 0.388, p < 0.025), personal (r = 0.457, p < 0.011) and daily living skills (r = 0.372, p < 0.033) domains on the VABS-2. Also, sensation seeking was positively correlated with gross motor skills as measured by PDMS-2 (r = 0.39, p < 0.03). The authors also looked at the association separately for AD and PDD-NOS groups. For the AD group, significant correlations were reported between the sensation avoiding and self-care (r = 0.44, p < 0.04), personal (r = 0.56, p < 0.01) and daily living skills (r = 0.48, p < 0.02) domains, and between low registration and personal skills (r = 0.44, p < 0.05). For the PDD-NOS group, however, the only significant correlation was found between sensation seeking and the self-care domain (r = 0.71, p < 0.03).
Discussion
This systematic review focused on 21 studies that examined relationships between sensory processing patterns and psychological constructs in individuals with ASD.
Evaluation Grid—Papers’ Quality
The evaluation grid was designed for the purpose of this review, although it could be used in other reviews evaluating studies using correlational analysis methods in ASD research. The grid could be also easily adapted to be used in a wider context of developmental disorders research or even typical development. However, as it was used first time in the review, its validity is not established.
A confirmation of the diagnosis of ASD is provided in all the papers included in the review. Some authors selected participants with a particular ASD subtype, with most of the authors reporting their participants as children and/or young people with ASD. In the new DSM-V (APA 2013), all the ASD subtypes that were present in the previous version of the Manual (APA 1994), namely, autistic disorder, Asperger’s disorder and PDD-NOS (pervasive developmental disorder not otherwise specified), were merged together under the umbrella of one term—autism spectrum disorder. This is important to bear in mind because findings from those studies, in which participants with only one ASD subtype were included, might be less generalisable to future studies, in which participants from across the spectrum will be included. Interestingly, in the study in which the results were presented for a total sample, and for two subtypes separately—AD and PDD-NOS groups (Jasmin et al. 2009), the findings differed for each subtype and for the total sample. ASD is a very heterogeneous disorder, with a diverse presentation across individuals. It seems therefore important to report both basic participants’ characteristics such as gender and age, as well as features such as cognitive ability in order to make some comparisons and generalisations between and within such a varied population.
A wide variety of measures were used to assess sensory processing difficulties in individuals with ASD in the selected review papers. Some authors, however, did not report whether the selected tools were appropriate to use with this clinical population. Only a few were reported as widely used within the ASD population or were ASD specific. Also, reliability and particularly validity of the tools were poorly reported. There is a lack of reliable and valid measures of sensory processing designed for use with ASD individuals. By using measures developed with and for typically developing individuals in ASD research without at least reporting their psychometric properties in this population, we have little evidence that the tools selected are appropriate. Therefore, researchers should consistently report psychometric properties of the tools used in the sample selected. Moreover, there are a great number of questionnaires and observational measures of sensory atypicalities available for use for researchers. The decision regarding which tools should be used to examine a research question might be based on a number of reasons, e.g. the measures selected in the previous studies, common use of tools by particular research group. There is no consensus between researchers about which measures of sensory processing should be used in future studies. This lack of consensus on ‘best-measures’ makes the comparison and interpretation of the results, obtained by employing different measures, problematic. Time spent identifying and developing ‘gold-standard’ sensory processing measures would help in understanding and interpreting the findings. Some authors (Boyd et al. 2010; Brock et al. 2012; Watson et al. 2011), rather than using a single measure, developed a sensory processing model based on information obtained from a range of measures and informants. Through this approach, the authors tried to overcome some limitations associated with using single, mainly parent-report-based measures and they yielded stronger sensory constructs scores. Building the factor analytic models is an interesting suggestion in sensory atypicalities measurement field. The models not only conglomerate information from different measures but also have excellent structural validity scores. Researchers might consider implementing this form of measuring sensory processing patterns in their studies.
Across the nine instruments of sensory atypicalities used in the paper selected for this review, the Sensory Profile and Short Sensory Profile were most frequently used. It should be remembered, however, that the Short Sensory Profile provides very limited information in regards to sensory processing patterns of individuals with ASD. Researchers might consider using tools which provide information on at least hypo- and hyperresponsivity to follow the dimensions of sensory atypicalities as suggested by DSM-V (APA 2013).
Thirty two different measures were used in the reviewed papers to assess psychological constructs in the ASD samples studied. Similar to the sensory processing measures, the psychometric properties of the selected tools were poorly reported (particularly the validity of the measures). Also, their appropriateness for use with this particular population was not justified. If excluding those tools which were used for both diagnosis and outcome measurements, only eight were reported as appropriate for use in autism research. There is not only a lack of tools designed specifically to assess a number of problems associated with the ASD, but also a lack of consensus regarding which measures are best suited to each specific phenomenon. As a result, researchers use different measures to investigate the same constructs (e.g. anxiety). Interpretation of the results and their generalisability is therefore hampered. As already highlighted in the systematic review conducted by the MeASURe team (McConachie et al. 2015, in press), for children with ASD under 6, psychometric work still needs to be done in order to select those tools which are reliable and valid within autism research.
Sensory Processing Patterns and Correlates
Concentrating on two main dimensions of sensory responsiveness—hyper- and hyporesponsiveness, as distinguished and suggested in DSM-V (APA 2013), most of the measures of autism symptom severity were associated with hyporesponsiveness (GARS autism quotient in Ashburner et al. 2008, DSM-IV communication impairment in Liss et al. 2006, ADOS social-communicative algorithm score in Watson et al. 2011 and DBS ASA in Baker et al. 2008). What is notable, however, is that in those papers investigating the relationships between symptom severity and sensory atypicalities, associations were found despite a wide range of symptom severity outcome measures being used, different groups included (HFASD in Hilton et al. 2007; ASD in Ashburner et al. 2008 and Liss et al. 2006; AD in Watson et al. 2011) and different age groups of participating children (although they all were up to 10 years old). It might indicate that those sensory atypicalities were so prevalent that they could be detected across ASD subtypes and with different measures. However, when the SRS was used (Hilton et al. 2007), correlations were found with both hypo- and hyperresponsiveness, with the social awareness subscale correlating only with hyperresponsiveness. Also, DMS-IV social symptoms subscale (Liss et al. 2006) was associated solely with hyperresponsiveness. Language and socio-communication variables (Baranek et al. 2013; Pfeiffer et al. 2005; Watson et al. 2011), joint attention (Baranek et al. 2013), stereotyped movement (Gal et al. 2010), a number of cognitive and social problems (Ashburner et al. 2008), maladaptive behaviours (Baker et al. 2008; Lane et al. 2010), some mood dimensions (Brock et al. 2012), emotion dysregulation (Samson et al. 2013) and gross motor skills (Jasmin et al. 2009) were all associated with hyporesponsiveness. On the other hand, self-care variables (Jasmin et al. 2009), anxiety (Green et al. 2012; Lane et al. 2012; Lidstone et al. 2014; Mazurek et al. 2013; Pfeiffer et al. 2005), socialisation subscale on the VABS (Liss et al. 2006), GI problems (Mazurek et al. 2013) and sleep difficulties (Reynolds et al. 2012) were correlated with hyperresponsiveness. Some variables were also associated with both sensory patterns, repetitive motor behaviours (Lidstone et al. 2014), insistence on sameness (Lidstone et al. 2014), depression (Pfeiffer et al. 2005), anxiety in Lidstone et al. (2014), attention (Liss et al. 2006), community use and social skills in Pfeiffer et al. (2005) study, and internalising and externalising scores (Tseng et al. 2011).
This evidence suggests that sensory hyporesponsiveness is more often associated with core features of ASD such as communication impairment, emotional, cognitive and behavioural problems while social awareness difficulties and affective disorders are associated with hyperresponsiveness. Similarly, Gay et al. (2008) suggested that hyporesponsiveness and sensory seeking may be more associated with difficulties in socio-communication domains in children with ASD. That supports the findings of Baranek et al. (2006) proposing that sensory hyporesponsiveness discriminated individuals with autism from those diagnosed with other developmental disorders or typically developing individuals. However, investigating other sensory processing patterns in the light of the findings of this review seems as important. Not only are high frequencies of hyperresponsiveness also present in individuals with ASD but also hypo- and hyperresponsiveness were reported to be present in the same individuals (Baranek et al. 2006), and some associations between both hypo- and hyperresponsiveness and other ASD features remain unclear (e.g. repetitive behaviours). Hyperresponsiveness, nevertheless, seems to be an under-researched sensory pattern. For example, in the studies investigating association between sensory processing patterns and anxiety, primarily the relationship between anxiety and overresponsivity was examined. While the link between children’s sensory overresponsivity, negative reactivity to complex sensory events and anxiety has been made in the reviewed papers, other associations were not explored. Only Lidstone et al. (2014) investigated other sensory processing patterns’ associations with more sensory atypicalities than hyperresponsivity and did find significant associations between anxiety and other sensory processing difficulties. Furthermore, because researchers widely use the Short Sensory Profile which includes an underresponsive/seeks sensation subscale only, finding and reporting associations with hyperresponsiveness is impossible.
It should also be noted that in some papers relatively small sample sizes were used (Ashburner et al. 2008; Baker et al. 2008; Chen et al. 2009; Lane et al. 2012; Reynolds et al. 2012) and therefore type II error might have occurred and some of the associations might have not been detected although a relationship between sensory atypicalities and measured constructs could exist in the population (Field 2009).
Study Limitations
The current review evidenced the sample selection process is highly varied across studies. There was also a lack of consistency in the methods employed. First, in some reviewed areas, a small number of studies were included, which limits the conclusions that can be drawn. Secondly, studies with a wide age range of participants were often pooled together, ignoring possible age-related differences in the presentation of both sensory atypicalities and ASD-related difficulties. Thirdly, the wide variety of methods assessing sensory processing patterns and psychological constructs used in the reviewed studies made the interpretation of the results very difficult.
Conclusions
In summary, the current research reports a number of associations between sensory processing patterns and the clinical and non-clinical features of ASD, highlighting that sensory atypicalities play an important role in the disorder. However, there are several theoretical and measurement approaches to the classification of the sensory processing patterns. Consensus on using a singular theoretical framework and set measures would help with clarifying results, but should be preceded with more psychometric work. In the absence of the agreement on measurement tools, multiple informant measures and sensory processing models based on information obtained from a range of measures and informants might be a bridging alternative.
There are also several questions that require further investigation. Hyperresponsiveness remains an under-researched sensory processing pattern; hence, establishing its associations with psychological constructs is an apparent research need. The current evidence provided for some constructs (e.g. repetitive behaviours) has mixed findings. Further research examining these correlations and establishing whether there are clear associations with a particular processing pattern or whether some psychological constructs correlate with a number of sensory atypicalities would benefit our understanding of the complexity of sensory processing difficulties in ASD.
Finally, at present, the research focuses on children and adolescents with ASD, without including adult participants in the recruited samples. Investigating associations between sensory processing patterns and psychological constructs in adults might shed some light into developmental changes of ASD characteristics.
References
*Study included in the review
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington DC: American Psychiatric Association.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, fourth edition, text revision (DSM-IV-TR). Washington DC: American Psychiatric Association.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington: American Psychiatric Publishing.
Anello, A., Reichenberg, A., Luo, X., Schmeidler, J., Hollander, E., Smith, C. J., et al. (2009). Brief report: parental age and the sex ratio in autism. Journal of Autism and Developmental Disorders, 39, 1487–1492.
*Ashburner, J., Ziviani, J., & Rodger, S. (2008). Sensory processing and classroom emotional, behavioral, and educational outcomes in children with autism spectrum disorder. American Journal of Occupational Therapy, 62, 564–573.
*Baker, A. E., Lane, A., Angley, M. T., & Young, R. L. (2008). The relationship between sensory processing patterns and behavioural responsiveness in autistic disorder: a pilot study. Journal of Autism and Developmental Disorders, 38(5), 867–875.
Baranek, G. T., David, F. J., Poe, M. D., Stone, W. L., & Watson, L. R. (2006). Sensory experience questionnaire: discriminating sensory features in young children with autism, developmental delays, and typical development. Journal of Child Psychology and Psychiatry, 47(6), 591–601.
*Baranek, G. T., Watson, L. R., Boyd, B. A., Poe, M. D., David, F. J., & McGuire, L. (2013). Hyporesponsiveness to social and nonsocial sensory stimuli in children with autism, children with developmental delays, and typically developing children. Development and Psychopathology, 25(02), 307–320.
Baranek, G. T. (2002). Efficacy of sensory and motor interventions for children with autism. Journal of Autism and Developmental Disorders, 5, 397–422.
Ben-Sasson, A., Hen, L., Fluss, R., Cermak, S., Engel-Yeger, B., & Gal, E. (2009). A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1–11.
Bodfish, J. W., Symons, F. J., Parker, D. E., & Lewis, M. H. (2000). Varieties of repetitive behaviour in autism: comparisons to mental retardation. Journal of Autism and Developmental Disorders, 30(3), 237–243.
*Boyd, B. A., Baranek, G. T., Siders, J., Poe, M. D., Watson, L. R., Patten, E., & Miller, H. (2010). Sensory features and repetitive behaviors in children with autism and developmental delays. Autism Research, 3, 78–87.
Boyd, B. A., McBee, M., Holtzclaw, T., Baranek, G. T., & Bodfish, J. W. (2009). Relationships among repetitive behaviors, sensory features, and executive functions in high functioning autism. Research in Autism Spectrum Disorders, 3(4), 959–966.
*Brock, M., Freuler, A., Baranek, G., Watson, L., Poe, M., & Sabatino, A. (2012). Temperament and sensory features of children with autism. Journal of Autism and Neurodevelopmental Disorders, 42, 2271–2284.
*Chen, Y. H., Rodgers, J., & McConachie, H. (2009). Restricted and repetitive behaviors, sensory processing and cognitive style in children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 635–642.
Crane, L., Goddard, L., & Pring, L. (2009). Sensory processing in adults with autism spectrum disorders. Autism: The International Journal of Research and Practice, 13(3), 215–228.
Deeks, J.J., Dinnes, J., D’Amico, R., Sowden, A. J., Sakarovitch, C., Song, F. & Altman, D.G. (2003). Evaluating non-randomised intervention studies. Health Technology Assessment, 7(27).
Dunn, W. (1997). The impact of sensory processing abilities on the daily lives of young children and families: a conceptual model. Infants and Young Children, 9(4), 23–25.
Field, A. (2009). Discovering statistics using SPSS: (and sex and drugs and rock’n’ roll) (3rd ed.). Los Angeles: Sage.
*Gal, E., Dyck, M. J., & Passmore, A. (2010). Relationships between stereotyped movements and sensory processing disorders in children with and without developmental or sensory disorders. American Journal of Occupational Therapy, 64, 453–461.
Gay, E., Watson, L. R., Baranek, G. T., Poe, M., & Boyd, B. (2008). Sensory processing patterns in relation to social communicative skills in young children with autism. San Diego: Gatlinburg Conference on Research and Theory in Intellectual and Developmental Disabilities.
*Green, S. A., Ben-Sasson, A., Soto, T. W., & Carter, A. S. (2012). Anxiety and sensory over-responsivity in toddlers with autism spectrum disorders: bidirectional effects across time. Journal of Autism and Developmental Disorders, 42, 1112–1119.
*Hilton, C., Graver, K., & LaVesser, P. (2007). Relationship between social competence and sensory processing in children with high functioning autism spectrum disorders. Research in Autism Spectrum Disorders, 1(2), 164–173.
Iarocci, G., & McDonald, J. (2006). Sensory integration and the perceptual experience of persons with autism. Journal of Autism and Developmental Disorders, 36(1), 77–90.
Interdisciplinary Council on Developmental and Learning Disorders (ICDL-DMIC) Work Groups. (2005). Interdisciplinary Council on Developmental and Learning Disorders Diagnostic manual for infancy and early childhood mental health disorders, developmental disorders, regulatory-sensory processing disorders, language disorders, and learning challenges. Bethesda: Author.
*Jasmin, E., Couture, M., McKinley, P., Reid, G., Fombonne, E., & Gisel, E. (2009). Sensori-motor and daily living skills of preschool children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 231–241.
John, A. E., & Mervis, C. B. (2010). Sensory modulation impairments in children with Williams syndrome. American Journal of Medical Genetics. Part C, Seminars in Medical Genetics, 154, 229–248.
Kern, J. K., Garver, C. R., Carmody, T., Andrews, A. A., Trivedi, M. H., & Mehta, J. A. (2007). Examining sensory quadrants in autism. Research in Autism Spectrum Disorders, 1(2), 185–193.
*Lane, A. E., Young, R. L., Baker, A. E. Z., & Angley, M. T. (2010). Sensory processing subtypes in autism: association with adaptive behavior. Journal of Autism and Developmental Disorders, 40, 112–122.
*Lane, S. J., Reynolds, S., & Dumenci, L. (2012). Sensory overresponsivity and anxiety in typically developing children and children with autism and attention deficit hyperactivity disorder: cause or coexistence? American Journal of Occupational Therapy, 66, 595–603.
Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., & Gould, J. (2007). Describing the sensory abnormalities of children and adults with autism. Journal of Autism and Developmental Disorders, 37, 894–910.
*Lidstone, L., Uljaveric, M., Sullivan, J., Rodgers, J., McConachie, H., Freeston, M., et al. (2014). Relations among restricted and repetitive behaviors, anxiety and sensory features in children with autism spectrum disorders. Research in Autism Spectrum Disorders, 8, 82–92.
*Liss, M., Saulnier, C., Fein, D., & Kinsbourne, M. (2006). Sensory and attention abnormalities in autism spectrum disorders. Autism, 10, 155–172.
Lydon, S., Healy, O., Reed, P., Mulhern, T., Hughes, B.M., & Goodwin, M.S. (2014). A systematic review of physiological reactivity to stimuli in autism. Developmental Neurorehabilitation, 1–21. doi:10.3109/17518423.2014.971975.
*Mazurek, M. O., Vasa, R. A., Kalb, L. G., et al. (2013). Anxiety, sensory over-responsivity, and gastrointestinal problems in children with autism spectrum disorders. Journal of Abnormal Child Psychology, 41, 165–176.
McConachie H., Parr, J. R. , Glod, M., Hanratty, J., Livingstone, N., Oono, I. P. et al. (2015). Systematic review of tools to measure outcomes for young children with autism spectrum disorder. Health Technology Assessment. In press.
Miller, L. J., Anzalone, M. E., Lane, S., Cemak, S., & Osten, E. (2007). Concept evolution in sensory integration: a proposed nosology for diagnosis. American Journal of Occupational Therapy, 61, 135–140.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Open Medicine, 3(3), 123–130.
Mokkink, L. B., Terwee, C. B., Patrick, D. L., Alonso, J., Stratford, P. W., Knol, D. L., Bouter, L. M., & de Vet, H. C. W. (2010). The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Quality of Life Research, 19, 539–549.
*Nadon, G., Feldman, D. E., Dunn, W., & Gisel, E. (2011). Mealtime problems in children with autism spectrum disorder and their typically developing siblings: a comparison study. Autism, 15(1), 98–113.
O’Neill, M., & Jones, R. S. P. (1997). Sensory-perceptual abnormalities in autism: a case for more research. Journal of Autism and Developmental Disorders, 27(3), 283–293.
PDM Task Force. (2006). Psychodynamic diagnostic manual. Silver Spring: Alliance of Psychoanalytic Organizations.
*Pfeiffer, B., Kinnealey, M., Reed, C., & Herzberg, G. (2005). Sensory modulation and affective disorders in children and adolescents with Asperger disorder. American Journal of Occupational Therapy, 59, 335–345.
*Reynolds, S., Lane, S. J., & Thacker, L. (2012). Sensory processing, physiological stress, and sleep behaviors in children with and without autism spectrum disorders. Occupational Therapy Journal of Research, 32, 246–257.
Rogers, S. J., & Ozonoff, S. (2005). Annotation: what do we know about sensory dysfunction in autism? A critical review of the empirical evidence. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 46(12), 1255–1268.
*Samson, A. C., Phillips, J. M., Parker, K. J., Shah, S., Gross, J. J., & Hardan, A. Y. (2013). Emotion dysregulation and the core features of autism spectrum disorder. Journal of Autism and Developmental Disorders, 44, 1766–1772.
Scottish Intercollegiate Guidelines Network (SIGN) (2008). SIGN 50—a guideline developer’s handbook. Retrieved from www.sign.ac.uk (28th July 2014).
Sollaci, L. B., & Pereira, M. G. (2004). The introduction, methods, results, and discussion (IMRAD) structure: a fifty-year survey. Journal of the Medical Library Association, 92, 364–367.
*Tseng, M. H., Fu, C. P., Cermak, S. A., Lu, L., & Shieh, J. Y. (2011). Emotional and behavioral problems in preschool children with autism: relationship with sensory processing dysfunction. Research in Autism Spectrum Disorders, 5, 1441–1450.
Turner, M. (1999). Annotation: Repetitive behaviour in autism: a review of psychological research. Journal of Child Psychology and Psychiatry, 40(6), 839–849.
*Watson, L. R., Patten, E., Baranek, G. T., Poe, M., Boyd, B. A., Freuler, A., et al. (2011). Differential associations between sensory response patterns and social-communication measures in children with autism and developmental disorders. Journal of Speech, Language, and Hearing Research, 54, 1562–1576.
Whiting, P., Rutjes, A., Reitsma, J., Bossuyt, P., & Kleijnen, J. (2003). The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Medical Research Methodology, 3(25).
Zero to Three. (2005). Diagnostic classification of mental health and developmental disorders of infancy and early childhood, revised (DC:0–3R). Arlington: National Center for Clinical Infant Programs.
Acknowledgments
This research was supported by PhD funding from the Estate of David Murray Garside (awarded to author MG). The authors would like to thank Dr Sarah Wigham for her contribution in estimating inter-rater reliability of the evaluation grid used in the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Glod, M., Riby, D.M., Honey, E. et al. Psychological Correlates of Sensory Processing Patterns in Individuals with Autism Spectrum Disorder: A Systematic Review. Rev J Autism Dev Disord 2, 199–221 (2015). https://doi.org/10.1007/s40489-015-0047-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-015-0047-8