



Introduction
Informal care-givers represent an essential pillar of care for individuals with dementia worldwide. Informal care-giving means providing, usually unpaid, assistance with personal care, basic functional and instrumental activities of daily living, or supervision of a family member or another related person. Dementia and cognitive impairment are the leading contributors to care dependence among older people (Prince et al., Reference Prince, Bryce, Albanese, Wimo, Ribeiro and Ferri2013). In 2015, the number of people living with dementia globally was approximately 47 million and the number is predicted to rise to over 131 million by 2050. This is due to the ageing of populations, and will affect low- and middle-income countries in particular (Prince et al., Reference Prince, Wimo, Guerchet, Ali, Wu and Prina2015). Most persons with dementia (PwD) worldwide live in the community in their own homes with support from informal care-givers who enable them to stay at home as long as possible (Erol et al., Reference Erol, Brooker and Peel2015).
Informal care-giving for PwD is often associated with considerable consequences for the personal and professional life of informal care-givers. First, the particular care needs of PwD often require a large time commitment on the part of the care-giver to provide supervision and support, particularly during the day. Moreover, behavioural disturbances often increase the intensity of care-giving and put pressure on care-givers’ wellbeing (Chiao et al., Reference Chiao, Wu and Hsiao2015; Feast et al., Reference Feast, Moniz-Cook, Stoner, Charlesworth and Orrell2016; Pinquart, Reference Pinquart and Suhr2016). Second, if the care-giver works, they are likely to face career disadvantages because of both the restrictions care-giving may put on their availability for work, as well as the intensity of caring. As a consequence, a productivity loss among informal care-givers of PwD arises which should be taken into account when measuring the costs of dementia (Deb et al., Reference Deb, Thornton, Sambamoorthi and Innes2017). The costs of informal care constitute the majority of total costs associated with PwD living in the community (König et al., Reference König, Leicht, Brettschneider, Bachmann, Bickel, Fuchs, Jessen, Köhler, Luppa, Mösch, Pentzek, Werle, Weyerer, Wiese, Scherer, Maier and Riedel-Heller2014; Lenox-Smith et al., Reference Lenox-Smith, Reed, Lebrec, Belger and Jones2016).
From a policy-making viewpoint, it is worthwhile developing an in-depth understanding of the interplay between informal care-giving in dementia and employment. This is important to alleviate not only the societal burden, but also the personal and economic burden on care-givers, by establishing or promoting suitable services to support their care-giving role. It is in the interest of employers that care-givers are able to maintain their working role with minimal interruptions whilst also fulfilling their responsibilities as informal care-givers.
The interplay between informal care-giving and employment has been examined by two reviews in the last decade (Lilly et al., Reference Lilly, Laporte and Coyte2007; Bauer and Sousa-Poza, Reference Bauer and Sousa-Poza2015). Findings on the overall effect of informal care-giving on employment remain ambiguous. Most studies have found evidence of a negative correlation between informal care-giving and employment. The magnitude of these effects appears to be rather small. However, stronger effects can be observed for very intense care-giving. If the care-giving responsibilities exceed ten hours per week, care-givers commit fewer hours to the labour market than non-care-givers (Lilly et al., Reference Lilly, Laporte and Coyte2007). In addition, very intense care-giving is provided primarily by females of working age, who are less likely to be fully employed and generally earn lower wages (Bauer and Sousa-Poza, Reference Bauer and Sousa-Poza2015). However, both these reviews focused on informal care-givers in general, and not specifically on informal care-givers of PwD.
To the best of our knowledge, to date, no study has systematically reviewed the interplay of informal care-giving for PwD and care-givers’ employment. This study aims to answer the following research questions:
(1) Which care-giving-related factors influence the work-life of informal care-givers of PwD?
(2) What kind of impact do these influencing factors have on care-givers’ employment?
The literature has demonstrated that the interplay between informal care-giving and work is complex due to their mutual dependence, and different research approaches have explored it. Thus, our objective is to identify the factors related to care-giving that influence employment, and to describe their impact on dementia care-givers’ employment, based on a mixed-study approach.
Materials and methods
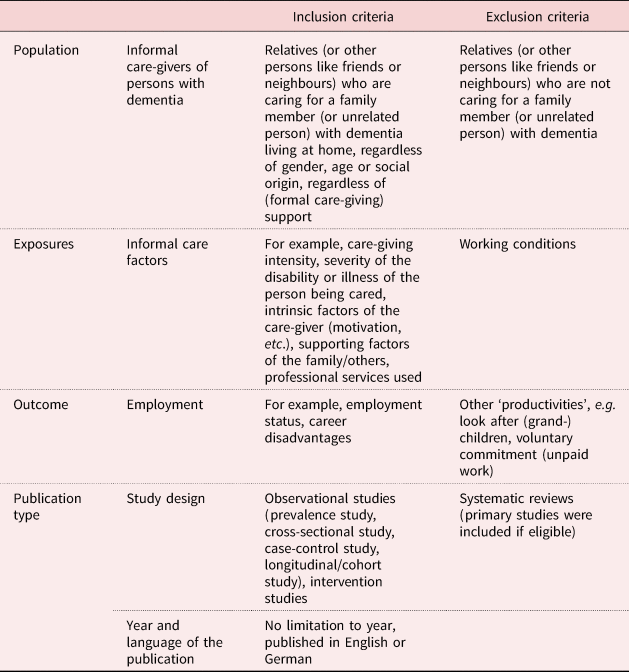
Conducting a mixed-studies review, researchers integrate qualitative, quantitative and mixed-methods studies to gain an increased understanding of complex interventions, programmes or phenomena (Pluye and Hong, Reference Pluye and Hong2014). Mixed-studies reviews follow the standard systematic review steps, which are described below. In advance, the inclusion criteria were summarised in a checklist (Table 1).
Table 1. Checklist of inclusion and exclusion criteria
Literature search
A systematic search was conducted in four electronic bibliographic databases (PubMed, CINAHL, PsycINFO and NHS Economic Evaluation Database) and one meta-database (LIVIVO) by one reviewer (LN) in September/October 2016 and January 2018. Using database-specific keywords and standard vocabulary (e.g. MeSH, if applicable), the search terms included ‘informal care’, ‘caregiver’, ‘elderly care’, ‘family’, ‘relatives’, ‘dementia’, ‘employment’, ‘work’ and ‘labo?r’. Additionally, an online-search for grey literature was conducted by one reviewer (LN). References were not limited to publication year. Only studies published in English or German were considered.
Selection of studies
Titles and abstracts of all identified records were screened independently by two reviewers (LN, CM). In the subsequent in-depth screening of the full texts, the potentially eligible full-text articles were assessed independently for final study inclusion again by both reviewers. Reasons for exclusion were documented. All relevant references of the included manuscripts were scanned for suitable studies; identified studies also underwent the procedure described above. Disagreements between the two reviewers were resolved by consensus or by consulting a third person (CB).
Structured form sheets were used for data extraction by one reviewer (LN). The extracted findings were divided into three types of evidence: qualitative (indicates narrative), quantitative descriptive and quantitative analytical. The completed form sheets were checked by a second reviewer (CM).
Quality assessment
The appraisal of the methodological quality of included studies was based on the validated Mixed Methods Appraisal Tool (MMAT-v2011) (Pluye et al., Reference Pluye, Robert, Cargo, Bartlett, O'Cathain, Griffiths, Boardman, Gagnon and Rousseau2011). The MMAT has been developed for systematic mixed-studies reviews that include qualitative, quantitative and mixed-methods studies. The MMAT has been tested for its content validity, efficiency and reliability (inter-rater reliability varied by criterion from fair (k = 0.21–0.40) to perfect (k = 0.81–1.00); the former only in two items pertaining to the section on qualitative research) (Pace et al., Reference Pace, Pluye, Bartlett, Macaulay, Salsberg, Jagosh and Seller2012; Souto et al., Reference Souto, Khanassov, Hong, Bush, Vedel and Pluye2015). Here, the appraisal was conducted by two independent researchers, with appropriate expertise for conducting the appraisal (LN, CM), who documented their decisions. Disagreements between the two researchers were resolved by consensus or by consulting a third person (CB). Authors were contacted when implausibility or inconsistencies in the published findings were identified.
The appraisal starts with two screening questions for all study types. When the answer is ‘no’ or ‘cannot tell’ to one or both screening questions, further appraisal may not be feasible or appropriate. In this case, articles that failed the appraisal of methodological quality according to MMAT were excluded. Included articles were assessed with one of five sections. The development team of the MMAT proposed scoring metrics (Pluye et al., Reference Pluye, Robert, Cargo, Bartlett, O'Cathain, Griffiths, Boardman, Gagnon and Rousseau2011) that were also applied.
Synthesis design
A parallel-results convergent synthesis design was chosen for synthesising included studies, to allow for a complementary analysis of the mixed evidence identified (Pluye and Hong, Reference Pluye and Hong2014; Hong et al., Reference Hong, Pluye, Bujold and Wassef2016). Data synthesis was conducted by one reviewer (LN), with regular discussions with a second reviewer (CB), and was checked by a third reviewer (CM). The process of synthesising was supported by applying MAXQDA (version 12; VERBI Software GmbH, Berlin, Germany). This software supports collection, organisation and analysis of literature in literature reviews. Here, evidence from all studies of qualitative, mixed and quantitative research approaches was thematically synthesised through the assignment of the textual data to categories (Thomas and Harden, Reference Thomas and Harden2008). For qualitative studies, a categorical system of themes and sub-themes emerged through deductive and inductive approaches. This analysis included 13 articles of qualitative research approaches and one mixed research approach.
The categorical system that was developed for qualitative evidence provided the basis for the synthesis of the quantitative studies. First, based on quantitative studies with only descriptive evidence, care-giving-related exposures and employment-related outcomes were summarised and organised into the already existing or new emerging categories. This analysis included evidence of 15 articles that undertook quantitative research approaches. Second, study findings based on analytical statistics of the remaining 26 articles were examined according to the same procedure.
The final categorical system comprised four themes: (a) exposures of the care recipient with dementia, (b) the care-giver, (c) care-giving context, and (d) employment-related outcomes – and different sub-themes. The selected articles were heterogeneous concerning study design, samples, methods and examined purposes. Therefore, pooling of data was not possible.
The results of the syntheses are not compared in the Results section. The results of both syntheses are interpreted in the Discussion section of this paper. Figure 1 demonstrates the performed parallel-results convergent synthesis design.
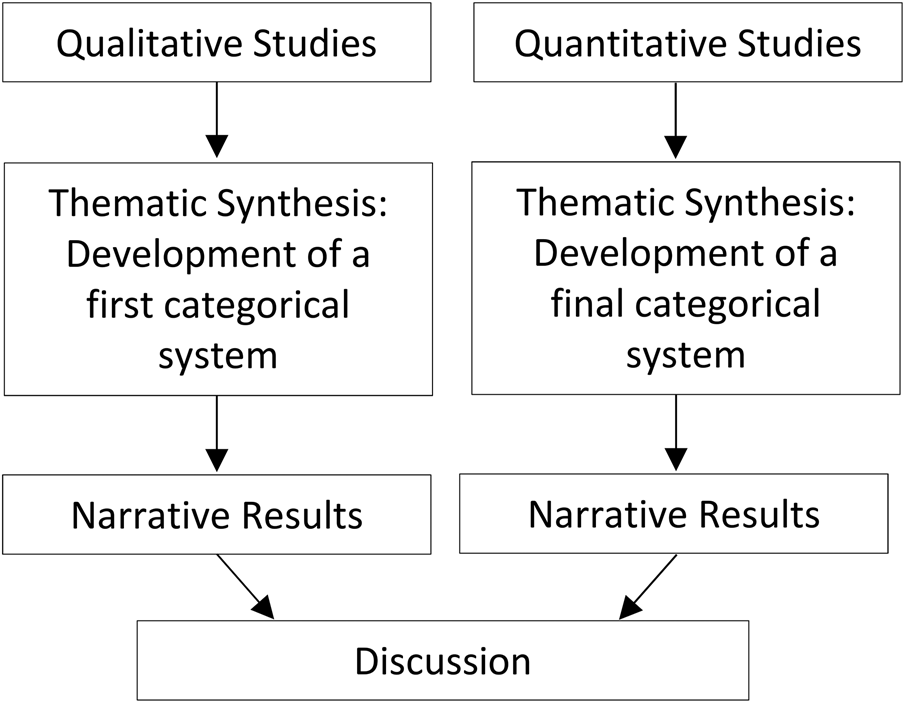
Figure 1. Used parallel-results convergent synthesis design of included mixed evidence.
Results
Through systematic online and database searching, 3,910 records were initially identified. These were published up to October 2016. Through an updated literature search we identified an additional 580 records that had been published between October 2016 and January 2018. Fifty-five primary studies met the inclusion criteria (Figure 2).
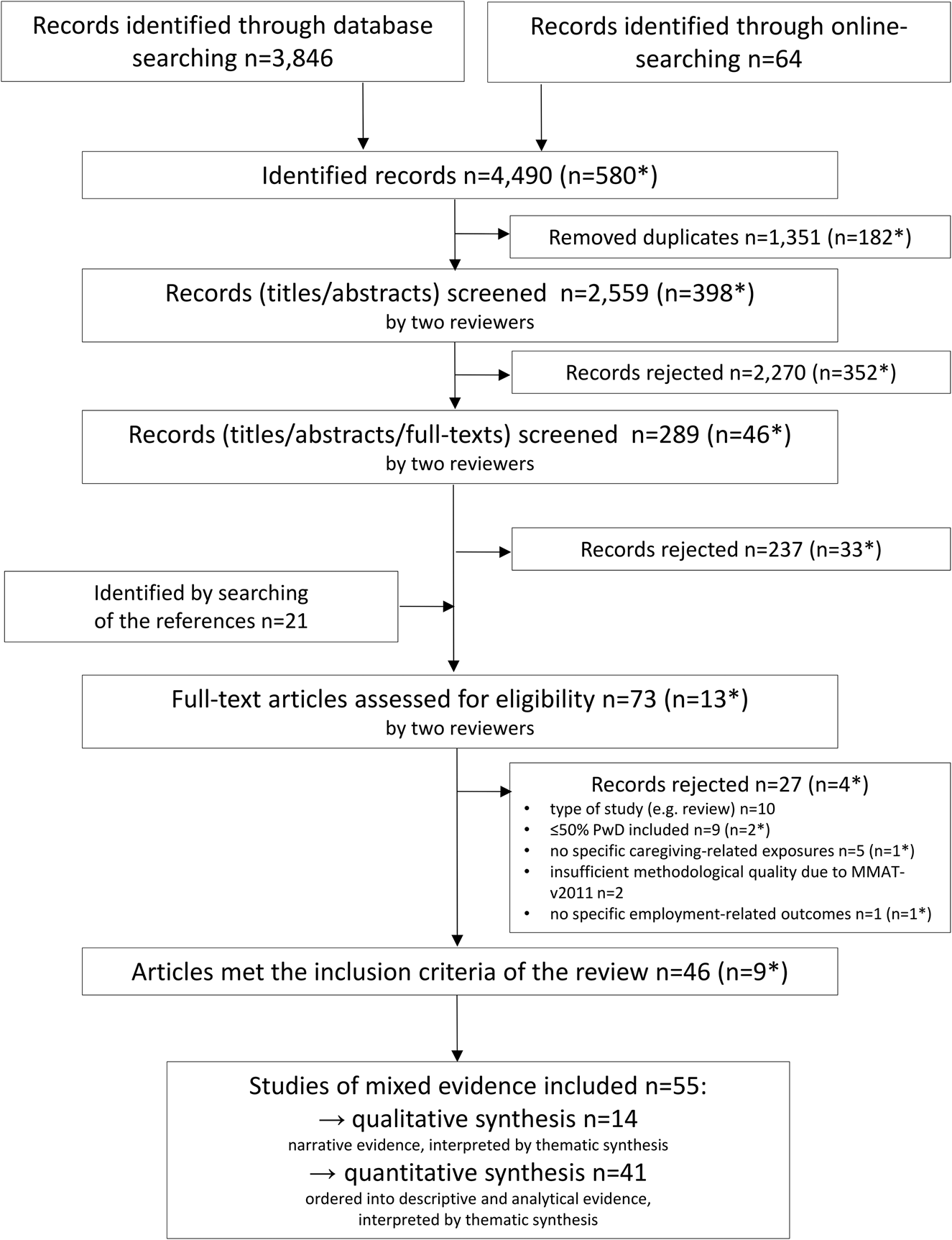
Figure 2. Process of study selection (according to the PRISMA flow diagram).
Notes: PWD: persons with dementia. MMAT-v2011: Mixed Methods Appraisal Tool. *Records published between October 2016 and January 2018.
General study characteristics
The majority of the studies under review were published from 2011 onwards (Table 2). The studies analysed data from North America (N = 20), the European Union (N = 21), Asia (N = 6), South America (N = 4) and Australia (N = 2). Two studies analysed data from more than one country or nation. With respect to the dementia subtype of care recipients in the included articles, Alzheimer's disease was the most reported dementia subtype, followed by non-specified dementia subtypes, subtypes due to another undeclared cause and the vascular/multi-infarct dementia subtype. Six articles explicitly mentioned patients diagnosed with frontotemporal dementia within their samples. Others indicated whether dementia subtypes were early onset, Lewy body and/or mixed dementia without any further specification.
Table 2. Summary of the 55 articles included in the mixed-studies review
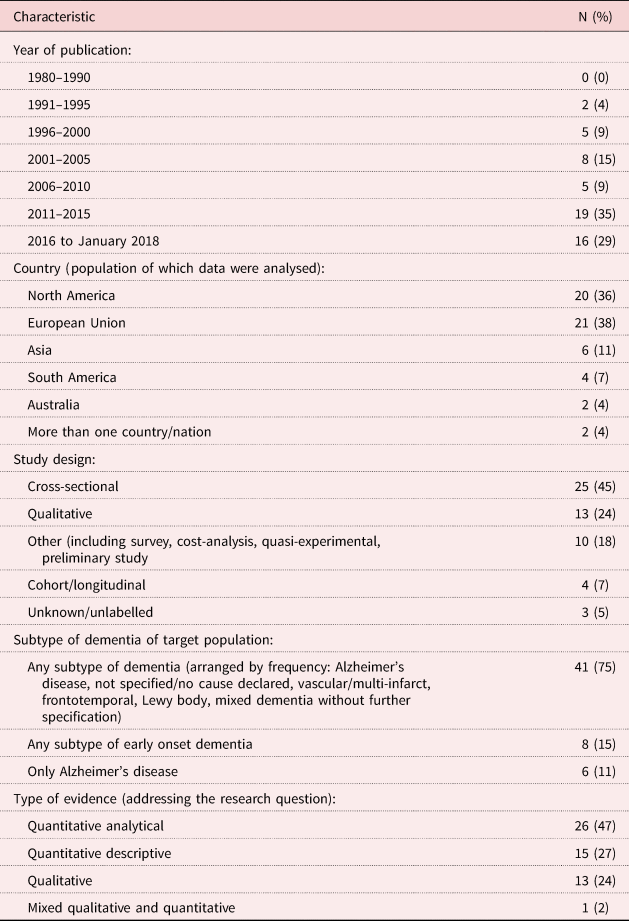
The type of evidence synthesised by the included quantitative studies (N = 41) was more analytical (47%, N = 26) than descriptive (27%, N = 15), however, this evidence was based almost exclusively on cross-sectional studies. The remainder of the studies presented qualitative (24%, N = 13) and mixed (qualitative and quantitative) evidence (2%, N = 1).
Methodological aspects
The methodological quality of all included studies varied, and the overall quality was rated as limited to sufficient in view of the study designs (Figure 3).
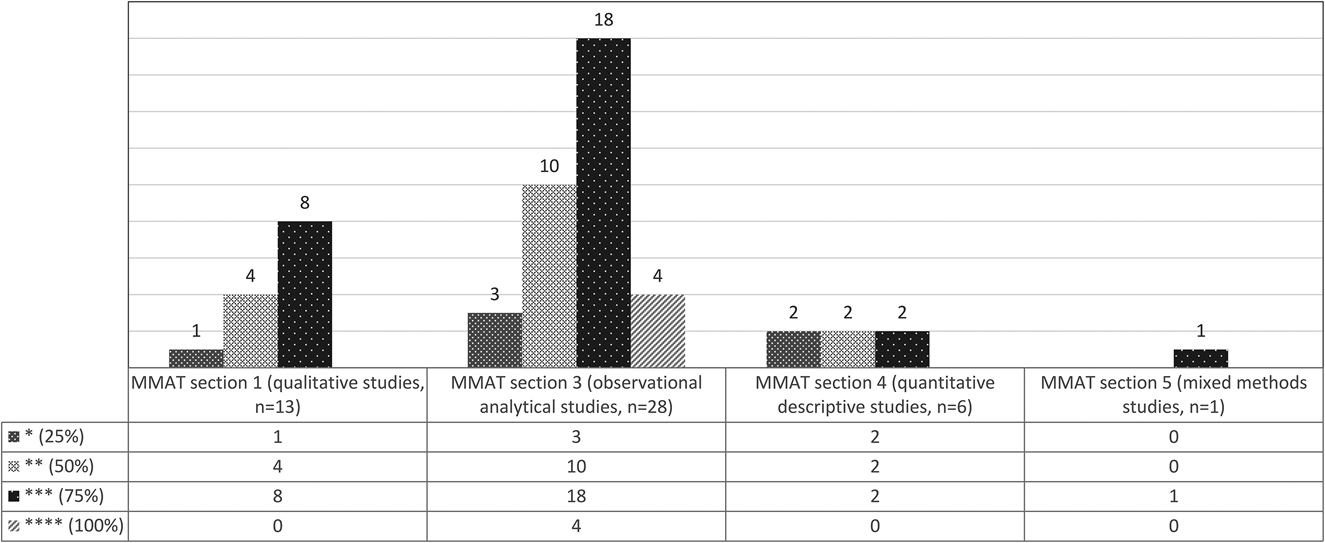
Figure 3. Overview of the appraisal of methodological quality for articles included in the review using the Mixed Methods Appraisal Tool (MMAT-v2011).
Synthesised findings
The following findings extracted from qualitative and quantitative studies describe care-giving factors that influence care-givers’ employment status and work-life. We trisected these influencing factors into factors concerning (a) the care recipient with dementia, (b) the informal care-giver and (c) the context of care-giving. First, we present the influencing factors found by qualitative and quantitative evidence (Research Question 1). Following this, to complement the interplay between informal care-giving and working, we present the employment-related effects we collected based on qualitative and quantitative evidence (Research Question 2).
For the first part of the data synthesis (Figure 1), we considered 13 articles with qualitative research approaches and one mixed research approach. Often spouses, children or children-in-law care for PwD as the primary or main care-giver. Three studies focused on care recipients suffering from early onset dementia (i.e. onset of dementia and time of diagnosis are under the age of 65 years (Harris and Keady, Reference Harris and Keady2004; Ducharme et al., Reference Ducharme, Kergoat, Coulombe, Lévesque, Antoine and Pasquier2014; Kimura et al., Reference Kimura, Maffioletti, Santos, Baptista and Dourado2015). The findings of the second part of the data synthesis were based on 41 studies. First, we considered 15 articles of quantitative research approaches with descriptively analysed results addressing the research question of this review. Additionally, we considered 26 studies with analytical statistics to complement the presented quantitative evidence. In line with the first data synthesis, most primary care-givers were the close relatives. However, other unpaid care-givers with a familial and non-familial relationship (e.g. friends) to the care recipient were also included. Five studies exclusively focused on patients with Alzheimer's disease (Cavallo and Fattore, Reference Cavallo and Fattore1997; Small et al., Reference Small, McDonnell and Papadopoulos2002; Gustavsson et al., Reference Gustavsson, Brinck, Bergvall, Kolasa, Wimo, Winblad and Jonsson2011; Søgaard et al., Reference Søgaard, Sørensen, Waldorff, Eckermann, Buss and Waldemar2014; Darbà and Kaskens, Reference Darbà and Kaskens2015) and six studies exclusively focused on patients with early onset dementia (Delany and Rosenvinge, Reference Delany and Rosenvinge1995; Luscombe et al., Reference Luscombe, Brodaty and Freeth1998; Bakker et al., Reference Bakker, de Vugt, van Vliet, Verhey, Pijnenburg, Vernooij-Dassen and Koopmans2013; Gibson et al., Reference Gibson, Anderson and Acocks2014; Cintra et al., Reference Cintra, Rezende and Torres2016; Ducharme et al., Reference Ducharme, Lachance, Kergoat, Coulombe, Antoine and Pasquier2016).
Influencing factors based on qualitative and quantitative evidence
To address the first research question, we collected care-giving factors that influence care-givers’ employment status and work-life. We trisected them into factors concerning the care recipient with dementia, the informal care-giver and the context of care-giving. Table 3 summarises all care-giving factors that influence care-givers’ employment.
Table 3. Influencing factors by qualitative and quantitative evidence
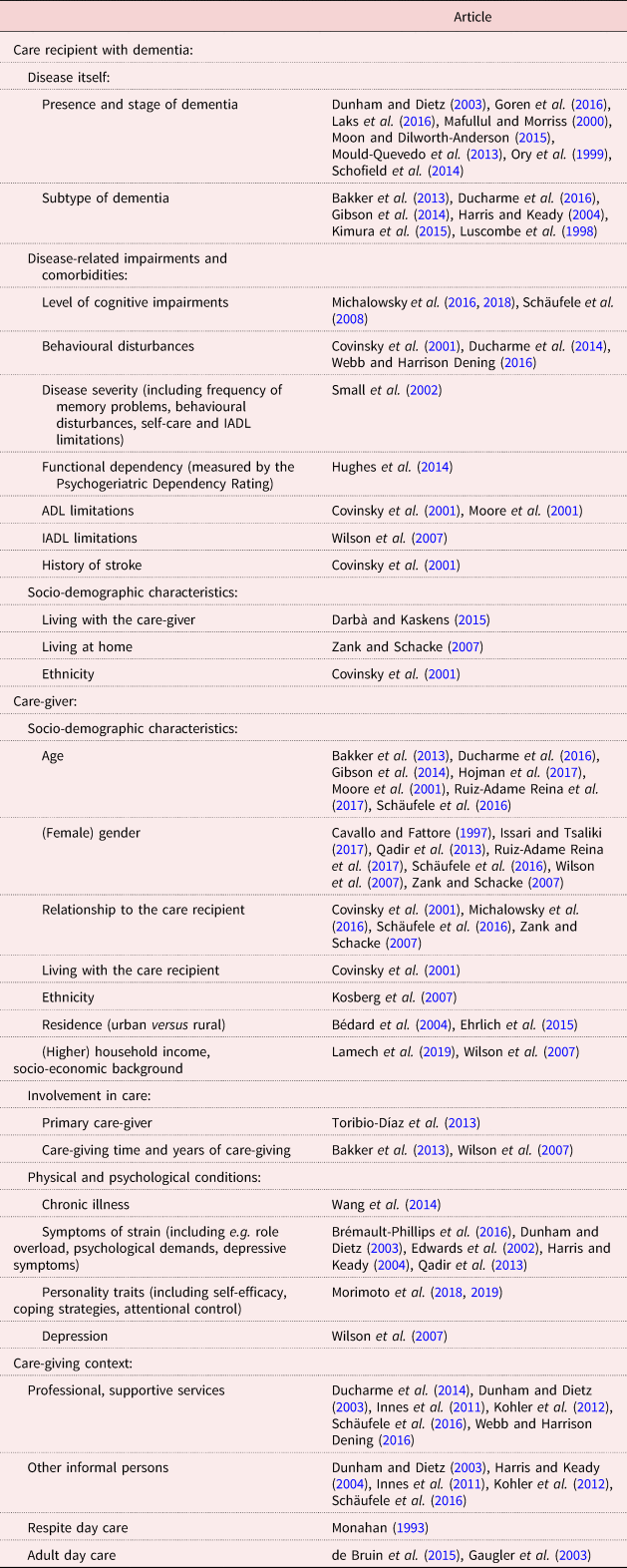
Notes: ADL: activities of daily living. IADL: instrumental activities of daily living.
Factors related to the care recipient with dementia
Based on qualitative evidence, the care-givers’ employment status was affected by the severity of the care recipient's impairments, behavioural disturbances, as well as the extent to which the care-giver considered the PwD able to be unsupervised during the day (Dunham and Dietz, Reference Dunham and Dietz2003; Ducharme et al., Reference Ducharme, Kergoat, Coulombe, Lévesque, Antoine and Pasquier2014; Webb and Harrison Dening, Reference Webb and Harrison Dening2016). Furthermore, had an employed relative been diagnosed with early onset dementia and lost his job (Harris and Keady, Reference Harris and Keady2004; Kimura et al., Reference Kimura, Maffioletti, Santos, Baptista and Dourado2015), the family had to adjust to the reduced household income by continuing to work, or by managing the financial loss.
To study the impact of care-giving for PwD, we considered two studies of quantitative evidence which compared care-givers of individuals with Alzheimer's disease with non-care-givers, defined as those who were currently not caring for an adult relative (Goren et al., Reference Goren, Montgomery, Kahle-Wrobleski, Nakamura and Ueda2016; Laks et al., Reference Laks, Goren, Duenas, Novick and Kahle-Wrobleski2016). With respect to employment status, the results are inconsistent. In one study, care-givers were less likely employed (Goren et al., Reference Goren, Montgomery, Kahle-Wrobleski, Nakamura and Ueda2016), however, in the other study they were more likely to be employed than non-care-givers (Laks et al., Reference Laks, Goren, Duenas, Novick and Kahle-Wrobleski2016). With respect to job performance, care-givers reported higher absenteeism, presenteeism-related impairment and greater overall work impairment than non-care-givers (Goren et al., Reference Goren, Montgomery, Kahle-Wrobleski, Nakamura and Ueda2016; Laks et al., Reference Laks, Goren, Duenas, Novick and Kahle-Wrobleski2016). To examine the impact related to dementia itself, we considered three studies which compared care-givers of PwD with care-givers of individuals without dementia (Ory et al., Reference Ory, Hoffman, Yee, Tennstedt and Schulz1999; Mafullul and Morriss, Reference Mafullul and Morriss2000; Moon and Dilworth-Anderson, Reference Moon and Dilworth-Anderson2015). Although both groups report that the care-giving role had adverse effects on their jobs (Mafullul and Morriss, Reference Mafullul and Morriss2000), dementia care-givers were less likely to be employed and more likely to be retired than non-dementia care-givers (Ory et al., Reference Ory, Hoffman, Yee, Tennstedt and Schulz1999). The former also experienced employment complications and a higher care-giving–work conflict than non-dementia care-givers (Ory et al., Reference Ory, Hoffman, Yee, Tennstedt and Schulz1999; Moon and Dilworth-Anderson, Reference Moon and Dilworth-Anderson2015).
Regarding the subtype of dementia, we can summarise that in samples of persons with early onset dementia, significantly more of the correspondingly younger care-givers were gainfully employed (Bakker et al., Reference Bakker, de Vugt, van Vliet, Verhey, Pijnenburg, Vernooij-Dassen and Koopmans2013; Ducharme et al., Reference Ducharme, Lachance, Kergoat, Coulombe, Antoine and Pasquier2016). They also often even worked full-time rather than part-time (Gibson et al., Reference Gibson, Anderson and Acocks2014). This could mean that the effect is not merely caused by the subtype of dementia, but rather because of the age of care-givers. With respect to all other factors, including the stage of dementia, disease-related impairments and socio-demographic characteristics, we found that they influenced care-givers’ employment negatively (Table 3). For example, the more severe the cognitive impairments of the PwD were, the more likely a care-giver's employment status was affected (i.e. reducing work hours or ceasing employment) (Schäufele et al., Reference Schäufele, Köhler, Teufel, Weyerer, Schneekloth and Wahl2008; Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016, Reference Michalowsky, Flessa, Eichler, Hertel, Dreier, Zwingmann, Wucherer, Rau, Thyrian and Hoffmann2018). In this context, the share of employed care-givers declined from 33 per cent, if care-givers cared for a person without cognitive impairments, to 20 per cent, if they cared for a person with severe cognitive impairments (Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016, Reference Michalowsky, Flessa, Eichler, Hertel, Dreier, Zwingmann, Wucherer, Rau, Thyrian and Hoffmann2018).
Factors related to the care-giver
Qualitative studies reported perceived tiredness, lack of time, and worry about balancing family, care and work responsibilities, as some signs of strain that affected care-givers’ employment situation (Dunham and Dietz, Reference Dunham and Dietz2003; Harris and Keady, Reference Harris and Keady2004; Qadir et al., Reference Qadir, Gulzar, Haqqani and Khalid2013; Brémault-Phillips et al., Reference Brémault-Phillips, Parmar, Johnson, Huhn, Mann, Tian and Sacrey2016). Male and female care-givers experienced a double burden of caring and working (Issari and Tsaliki, Reference Issari and Tsaliki2017). For some female care-givers, a threefold burden appeared if they were also responsible for child care (Qadir et al., Reference Qadir, Gulzar, Haqqani and Khalid2013). The employed care-givers from both a lower and a higher socio-economic background reported challenges at their workplaces, such as adapting work schedules (Lamech et al., Reference Lamech, Raghuraman, Vaitheswaran and Rangaswamy2019). Shared household income allowed female care-givers to continue part-time employment, and a partner who supported them with care responsibilities allowed them to maintain full-time employment (Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012). Thus, having a family and the costs of child care implied an additional strain, on the one hand. However, it could also also be a relief when other family members replaced the primary care-giver during working hours (Dunham and Dietz, Reference Dunham and Dietz2003; Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012; Qadir et al., Reference Qadir, Gulzar, Haqqani and Khalid2013; Brémault-Phillips et al., Reference Brémault-Phillips, Parmar, Johnson, Huhn, Mann, Tian and Sacrey2016).
The relationship between the listed influencing factors of quantitative evidence (Table 3) and their effect on care-givers’ employment was unambiguous and conclusive in many instances. For example, younger care-givers of PwD were more gainfully employed and worked more hours than older care-givers (Moore et al., Reference Moore, Zhu and Clipp2001; Bakker et al., Reference Bakker, de Vugt, van Vliet, Verhey, Pijnenburg, Vernooij-Dassen and Koopmans2013; Gibson et al., Reference Gibson, Anderson and Acocks2014; Ducharme et al., Reference Ducharme, Lachance, Kergoat, Coulombe, Antoine and Pasquier2016; Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016; Hojman et al., Reference Hojman, Duarte, Ruiz-Tagle, Budnich, Delgado and Slachevsky2017; Ruiz-Adame Reina et al., Reference Ruiz-Adame Reina, González-Camacho, Romero-García and Sánchez-Reyes Fernández2017). Other aspects require further analysis.
Regarding gender, ambiguous results due to sample characteristics were reported. Employed care-givers of PwD were more likely female and more likely to modify their employment status (Cavallo and Fattore, Reference Cavallo and Fattore1997; Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016). However, female care-givers were younger than men in both these studies. Additionally, female care-givers were less likely to be employed full-time than men, and considered care-giving constrains their opportunities for job promotion (Ruiz-Adame Reina et al., Reference Ruiz-Adame Reina, González-Camacho, Romero-García and Sánchez-Reyes Fernández2017).
Regarding the relationship to the PwD, employed care-givers were often the children (-in-law) or grandchildren of the care recipient. Therefore, they were more likely to be younger than non-employed family care-givers. In contrast, fewer spousal care-givers were employed (Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016; Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016). Also, female relatives of the care recipient with dementia reported more employment complications than male relatives. For example, daughters (-in-law) were more likely to reduce work hours than were sons (-in-law) (Covinsky et al., Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001). The wives and daughters of relatives with dementia frequently reported more strain due to the care-giving–work conflict than sons, daughters-in-law and husbands (Zank and Schacke, Reference Zank and Schacke2007). Here, the crucial points seemed to be age and gender rather than the relationship to the PwD.
Care-givers who lived with the patient and with no other care-giver remained at the highest risk for reducing work hours (Covinsky et al., Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001). With respect to the place of residence of the care-giver, we found inconsistent results. Not statistically significantly, more care-givers living in an urban area than in a rural area were employed in one study (Ehrlich et al., Reference Ehrlich, Boström, Mazaheri, Heikkilä and Emami2015), whereas more rural care-givers were employed in another study (Bédard et al., Reference Bédard, Koivuranta and Stuckey2004); however, this finding was not generalisable due to a small sample size.
For employed care-givers, strong correlations indicated a relationship between care-giving–work interactions and psychological symptoms of strain. Work conflicts were strongly associated with role overload, worry and strain, and depressive symptoms. Nevertheless, positive work experiences were weakly associated with lower depressive symptoms, time constraints and psychological demands. Employed care-givers experienced role conflicts, but they may have adapted in various ways to their double role of working and care-giving (Edwards et al., Reference Edwards, Zarit, Stephens and Townsend2002). Morimoto et al. (Reference Morimoto, Furuta, Kono and Kabeya2018, Reference Morimoto, Furuta, Kono and Kabeya2019) examined care-givers’ self-efficacy, coping strategies and attentional control under the assumption that these personality traits can moderate role conflicts. However, self-efficacy did not relieve the effect of care-giving demands on role conflict for employed care-givers of PwD in Japan (Morimoto et al., Reference Morimoto, Furuta, Kono and Kabeya2018), whereas coping strategies, especially formal support seeking, had a stress-buffering effect on role conflict. This effect was moderated by attentional control (it refers to a person's capacity to focus and shift attention flexibly when necessary; this means, individuals with high attentional control focus their attention on appropriate stimuli and ignore distractions, whereas reduced attentional control has been implicated in psychopathologies such as depression, e.g. Morimoto et al., Reference Morimoto, Furuta, Kono and Kabeya2019). This finding indicates that greater use of formal support seeking can relieve role conflict in employed care-givers with high attentional control and, thus, reduce psychological strain (Morimoto et al., Reference Morimoto, Furuta, Kono and Kabeya2019). Finally, care-giver depression had a significant and positive association with time missed at work (Wilson et al., Reference Wilson, Van Houtven, Stearns and Clipp2007).
Factors related to the care-giving context
Based on qualitative evidence (Table 3), other members of the family, or acquaintances of the primary care-givers, were a considerable resource for managing the care-giving situation (Dunham and Dietz, Reference Dunham and Dietz2003; Harris and Keady, Reference Harris and Keady2004; Innes et al., Reference Innes, Abela and Scerri2011; Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012). A ‘social front of family coping’, meaning how the family organised dementia care-giving (e.g. rotating the care among family members), allowed family care-givers to maintain their professional as well as social life (Innes et al., Reference Innes, Abela and Scerri2011). Fellow workers with similar care-giving experiences and support groups for informal care-givers were further sources of social support (Dunham and Dietz, Reference Dunham and Dietz2003). Paid community and formal supportive services included Meals on Wheels, home health care, household helpers and, in particular, respite care services, whereby the home-dwelling relative with dementia was cared for during the day (Dunham and Dietz, Reference Dunham and Dietz2003; Innes et al., Reference Innes, Abela and Scerri2011; Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012; Ducharme et al., Reference Ducharme, Kergoat, Coulombe, Lévesque, Antoine and Pasquier2014; de Bruin et al., Reference de Bruin, Stoop, Molema, Vaandrager, Hop and Baan2015). If the care recipient enjoyed attending an adult day service, the spousal care-givers were still able to continue working without feelings of guilt and worries (de Bruin et al., Reference de Bruin, Stoop, Molema, Vaandrager, Hop and Baan2015). A case study presented the work of an Admiral Nurse who helped navigate a care-giving son ‘through the various transitions points along the journey’ of his father with dementia (Webb and Harrison Dening, Reference Webb and Harrison Dening2016). However, paid services required an appropriate household income in the caring family (Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012).
Regarding the quantitative evidence (Table 3), we identified only three studies which investigated the interplay between the care-giving context and care-givers’ employment. With respect to the informal resources and the supportive services used, employed care-givers were more likely to use professional, supportive services to maintain the household than non-employed care-givers. Both groups of care-givers in this sample reported that they felt similarly as strongly supported by other persons (Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016). There was no explanation for this observation. Therefore, we reserve this observation for later discussion. However, another small study on care-givers who used a dementia-specific respite day care reported adverse effects on their workplace due to caring (Monahan, Reference Monahan1993). A quasi-experimental interventional study analysed the short- and long-term cost implications of a community-based adult day care programme (Gaugler et al., Reference Gaugler, Zarit, Townsend, Stephens and Greene2003). In the short-term analysis, the employment costs, measured as the difference in earnings caused by changed work conditions due to care-giving, were significantly higher among adult day service users than non-users. However, in the long-term cost analysis, the employment costs were significantly lower for adult day service users. This finding indicated a reduced loss of income when the adult day care programme was used for a longer period of time (Gaugler et al., Reference Gaugler, Zarit, Townsend, Stephens and Greene2003).
Effects on employment status and work-life based on qualitative and quantitative evidence
To address the second research question, we considered the effects of particular influencing factors on the work-life of informal care-givers of PwD. The effects are mostly negative. Only a few effects could be evaluated as being neutral or even positive. For example, continued employment and positive work experiences were found in quantitative studies. Based on qualitative studies, positive work experiences include, for example, enhanced job performance, organisational skills and increased stress resilience towards other persons. Qualitative evidence also suggested that working provides a possibility of refuge to informal care-givers of PwD. In studies with quantitative evidence, reduced work hours were determined to be the most common effect of care-giving on work-life. Ceasing employment to care for a PwD was frequently reported, and represented a last resort for informal care-givers in cases where rearrangement of work conditions was insufficient. Table 4 summarises these effects for all studies, including qualitative and quantitative studies.
Table 4. Effects on care-givers’ employment by qualitative and quantitative evidence
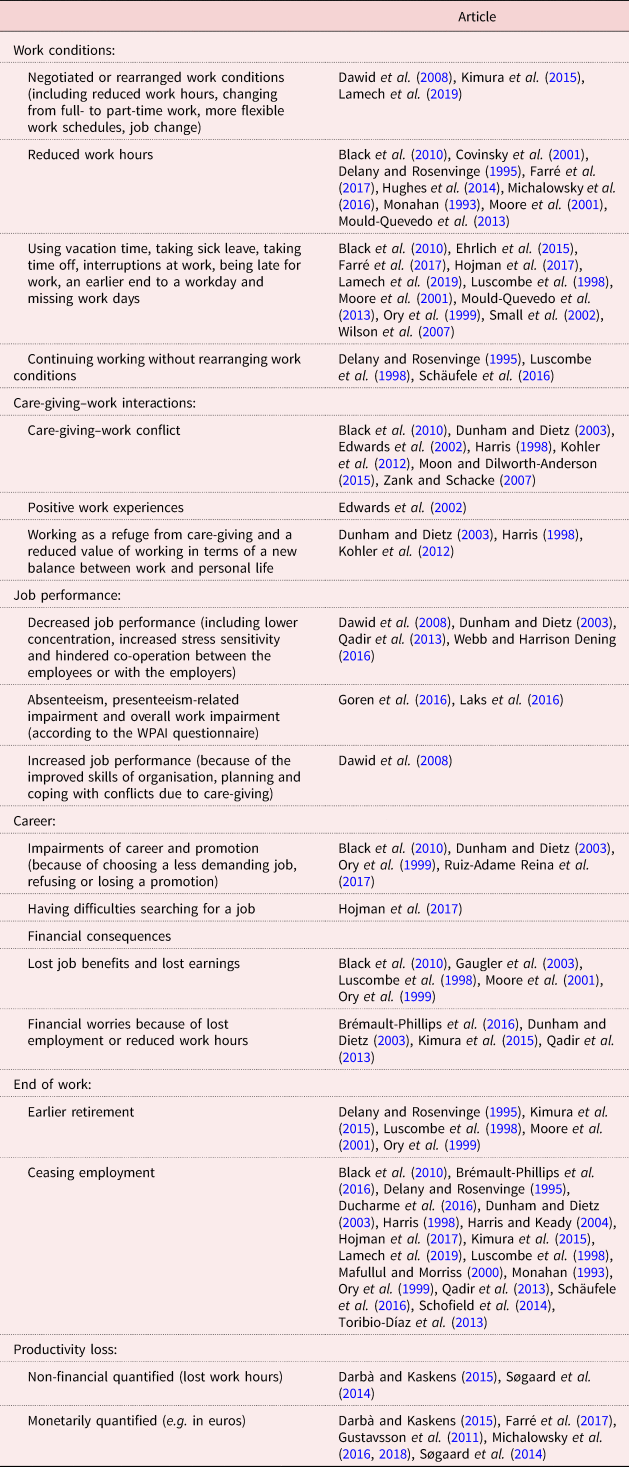
Note: WPAI: Work Productivity and Activity Impairment Questionnaire.
Furthermore, we looked closely at employment rates and productivity loss of informal care-givers of PwD.
The employment rates in examined studies primarily depended on the age of dementia care-givers. Higher employment rates from 37 to 72 per cent were reported in studies including younger care-givers (Luscombe et al., Reference Luscombe, Brodaty and Freeth1998; Ory et al., Reference Ory, Hoffman, Yee, Tennstedt and Schulz1999; Small et al., Reference Small, McDonnell and Papadopoulos2002; Kosberg et al., Reference Kosberg, Kaufman, Burgio, Leeper and Sun2007; Hughes et al., Reference Hughes, Black, Albert, Gitlin, Johnson, Lyketsos and Samus2014; Goren et al., Reference Goren, Montgomery, Kahle-Wrobleski, Nakamura and Ueda2016; Laks et al., Reference Laks, Goren, Duenas, Novick and Kahle-Wrobleski2016). Lower employment rates of nearly 30 per cent were described in studies including older care-givers (Cavallo and Fattore, Reference Cavallo and Fattore1997; Moore et al., Reference Moore, Zhu and Clipp2001; Gaugler et al., Reference Gaugler, Zarit, Townsend, Stephens and Greene2003; Zank and Schacke, Reference Zank and Schacke2007; Schäufele et al., Reference Schäufele, Köhler, Teufel, Weyerer, Schneekloth and Wahl2008, Reference Schäufele, Köhler, Hendlmeier and Suhr2016; Toribio-Díaz et al., Reference Toribio-Díaz, Medrano-Martínez, Moltó-Jordá and Beltrán-Blasco2013; Søgaard et al., Reference Søgaard, Sørensen, Waldorff, Eckermann, Buss and Waldemar2014; Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016). Employment rates are also affected by the care-givers’ involvement in care, the family relationship with the individual with dementia and having chronic illnesses (Cavallo and Fattore, Reference Cavallo and Fattore1997; Toribio-Díaz et al., Reference Toribio-Díaz, Medrano-Martínez, Moltó-Jordá and Beltrán-Blasco2013; Wang et al., Reference Wang, Robinson and Carter-Harris2014; Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016). Two German studies have examined the relation between employment rates and the presence and severity of dementia. Both confirmed that the percentage of employed care-givers decreased with an increased level of cognitive impairments (Michalowsky et al., Reference Michalowsky, Flessa, Eichler, Hertel, Dreier, Zwingmann, Wucherer, Rau, Thyrian and Hoffmann2018, Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016 used the Mini Mental State Examination; Schäufele et al., Reference Schäufele, Köhler, Teufel, Weyerer, Schneekloth and Wahl2008 used the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) and Clinical Dementia Rating to measure the severity of dementia).
Productivity loss, based on decreased employment rates and reduced work hours due to informal care-giving, is a considerable consequence experienced by employed care-givers and their employers. The productivity loss of employed care-givers of persons with Alzheimer's disease in Spain amounted to, on average, seven reduced hours per week, or one lost workday in the last month, or almost two partial workdays lost in the last month (Darbà and Kaskens, Reference Darbà and Kaskens2015). Monetarily quantified productivity loss differed according to the level of impairment of the PwD (Gustavsson et al., Reference Gustavsson, Brinck, Bergvall, Kolasa, Wimo, Winblad and Jonsson2011; Darbà and Kaskens, Reference Darbà and Kaskens2015; Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016, Reference Michalowsky, Flessa, Eichler, Hertel, Dreier, Zwingmann, Wucherer, Rau, Thyrian and Hoffmann2018). For example, a German study found that productivity loss (in euros) was greater in patients with mild and moderate cognitive impairment (Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016, Reference Michalowsky, Flessa, Eichler, Hertel, Dreier, Zwingmann, Wucherer, Rau, Thyrian and Hoffmann2018). Simultaneously, the care-givers’ average working hours per week decreased from 34 to 30 hours with the progression of the patients’ cognitive impairments in this German sample. In a Spanish sample, the cost of productivity loss was €378 per month; however, costs associated with the institutional setting were also included, making comparisons difficult (Farré et al., Reference Farré, Kostov, Haro, Cabrera, Risco, Alvira, Miguel and Zabalegui2017). A study comparing productivity loss of care-givers of community-dwelling patients with Alzheimer's disease living in Spain, Sweden, the United Kingdom and the United States of America (USA) revealed in the Swedish sample a considerable linear increase in productivity loss from mild to severe dementia (Gustavsson et al., Reference Gustavsson, Brinck, Bergvall, Kolasa, Wimo, Winblad and Jonsson2011).
Figure 4 visualises the emerging model of influencing factors and their impact on care-givers’ employment.
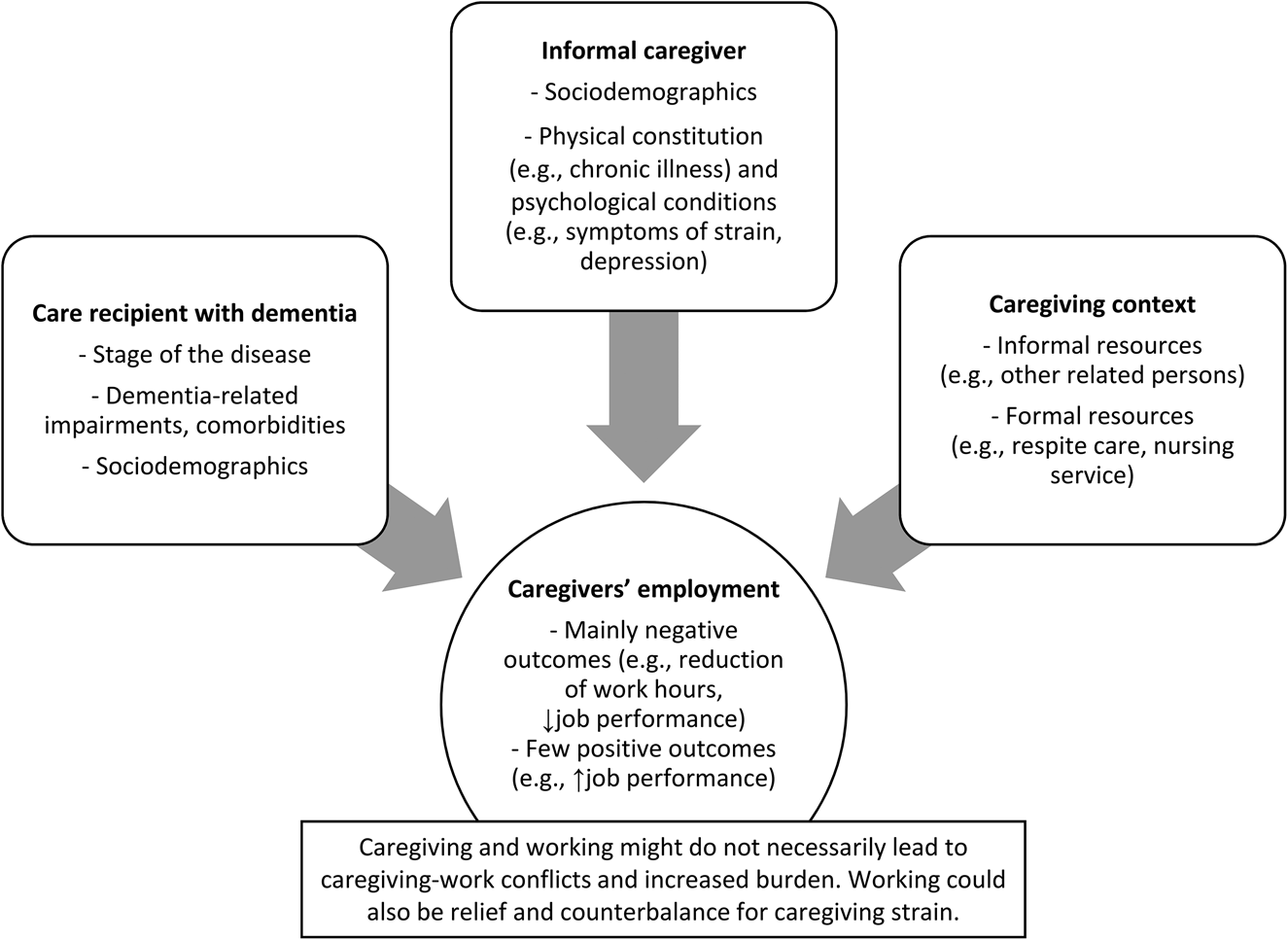
Figure 4. Model of the themes which emerged in this review.
Discussion
For the first time, by reviewing the existing literature of mixed evidence, our work points to care-giving factors that influence the employment status and work-life of informal care-givers of PwD. The emerging model (Figure 4) contains influencing factors trisected into factors regarding (a) the care recipient with dementia, (b) the care-giver, and (c) factors within the care-giving context. The impact of these factors on care-givers’ employment is mostly negative. However, a few studies reported that positive work experiences, and that working itself, can be a relief and counterbalance for care-giving strain at home.
The findings are discussed below by merging the interpreted qualitative and quantitative findings. As appropriate, we cite studies focusing on care-giving in general to broaden the perspective.
How strong is the impact of the disease itself?
Compared to non-care-givers (Goren et al., Reference Goren, Montgomery, Kahle-Wrobleski, Nakamura and Ueda2016, Laks et al., Reference Laks, Goren, Duenas, Novick and Kahle-Wrobleski2016) and informal care-givers of individuals without dementia (Ory et al., Reference Ory, Hoffman, Yee, Tennstedt and Schulz1999; Mafullul and Morriss, Reference Mafullul and Morriss2000; Moon and Dilworth-Anderson, Reference Moon and Dilworth-Anderson2015), care-givers of PwD experienced decreased work productivity, more care-giving–work conflicts or they stopped working. The subtype of dementia, the care recipient's stage of disease (Schäufele et al., Reference Schäufele, Köhler, Teufel, Weyerer, Schneekloth and Wahl2008, Reference Schäufele, Köhler, Hendlmeier and Suhr2016; Mould-Quevedo et al., Reference Mould-Quevedo, Tang, Harary, Kurzman, Pan, Yang and Qiao2013), the level of dementia-related impairments in general (e.g. Moore et al., Reference Moore, Zhu and Clipp2001; Small et al., Reference Small, McDonnell and Papadopoulos2002; Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016) or the need for supervision during the day in particular (Webb and Harrison Dening, Reference Webb and Harrison Dening2016) conflicted with the care-giver's work-life, leading to reduced work hours followed by lost earnings. Therefore, caring for PwD implies an emotional, social and financial burden on care-givers, as a consequence of its restricting influence on their employment. However, this also depends on the individual characteristics of the care recipient, their care-givers and how they organise the care. For example, according to the literature, managing the care of individuals with severe cognitive impairment can foster care-giving satisfaction (de Labra et al., Reference de Labra, Millán-Calenti, Buján, Núñez-Naveira, Jensen, Peersen, Mojs, Samborski and Maseda2015) and lead to personal growth among care-givers (Leipold et al., Reference Leipold, Schacke and Zank2006; Ott et al., Reference Ott, Sanders and Kelber2007; Shim et al., Reference Shim, Barroso, Gilliss and Davis2013). It is possible that these developments can also positively affect the work-life of the care-givers, as the few neutral or even positive employment-related outcomes demonstrated.
The finding that patients’ ethnicity influenced the risk of reduced employment in a US sample (Covinsky et al., Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001) points to cultural aspects of care-giving. These are also important in terms of the relationship between informal care and care-givers’ working. We consider this aspect in the next section by discussing the impact of a care-giver's ethnicity.
Notably, we cannot entirely quantify the impact of the disease itself, as well as the direction of causality, due to the included study designs. The quantitative studies quoted above are cross-sectional. Further research should be prospective and include care-givers of individuals with and without dementia, to compare both groups and to determine causality.
Which conditions favour or detract from care-giving and concurrent employment?
First, the socio-demographic factors identified in our study on informal care-givers for PwD are in line with the results of previous studies on informal care-givers in general. These studies concluded that socio-demographic factors are likely associated with less labour force participation, or workplace adjustments of informal care-givers in general (Lilly et al., Reference Lilly, Laporte and Coyte2007). Additionally, in informal care-givers of PwD, employment rates vary by age. Namely younger care-givers are more frequently gainfully employed than older care-givers. Gender differences were considered in several studies focusing on care-giving in general, where, in particular for women, a negative impact on employment was reported (e.g. Arber and Ginn, Reference Arber and Ginn1995; Wakabayashi and Donato, Reference Wakabayashi and Donato2005; Lilly et al., Reference Lilly, Laporte and Coyte2007; Viitanen, Reference Viitanen2010; Bauer and Sousa-Poza, Reference Bauer and Sousa-Poza2015). Notably, the majority of care-givers are female (Colombo et al., Reference Colombo, Llena-Nozal, Mercier and Tjadens2011). The reason for this gender difference may be their own conceptions, or gendered cultural and societal expectations, of caring for people in need such as children, elderly or disabled persons (Erol et al., Reference Erol, Brooker and Peel2015). Conceptions and expectations must also be considered in light of the history and structure of their family (Gröning and Kunstmann, Reference Gröning, Kunstmann, Bauer and Gröning2008). Female care-givers experience career disadvantages more often (Ruiz-Adame Reina et al., Reference Ruiz-Adame Reina, González-Camacho, Romero-García and Sánchez-Reyes Fernández2017), and we showed that this also extends to informal female care-givers of PwD. We note that the presented findings related to socio-demographic factors should be cautiously considered as interaction effects may exist. For instance, care-givers’ gender may influence the employment status, but a possible interaction effect of age can be assumed based on two studies included in this review (Cavallo and Fattore, Reference Cavallo and Fattore1997; Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016). Due to the assumed interrelations among gender, age and kinship, future research should examine the relationship between informal care-giving and employment by taking all potential influencing factors into account. This is all the more critical if further growth in the number of people who balance employment with other roles, such as care-giving, is expected due to increasing employment rates of older persons and women (Kröger and Yeandle, Reference Kröger and Yeandle2013). With respect to income, our review reveals a result specific to dementia. Families with higher incomes are more likely to spend more time absent from work (Wilson et al., Reference Wilson, Van Houtven, Stearns and Clipp2007). Contradictory results, namely care-givers with low income being more absent from work, were found by a previous review that focused on care-giving in general (Lilly et al., Reference Lilly, Laporte and Coyte2007). However, the authors indicated that the impact was not solely related to care-giving, but, instead, was a common effect that can also be observed in the general population. Therefore, the conclusion that high-earning dementia care-givers are more likely to perform fewer work hours should be viewed as preliminary, and further research is recommended. We note that working care-givers in this US sample were older female spouses of veterans with dementia (who thus benefited from pensions for veterans) and were not representative of the general US population (Wilson et al., Reference Wilson, Van Houtven, Stearns and Clipp2007).
Care-giving-specific factors that enhance the adverse employment-related effects in care-givers include a close relationship, co-residence with the PwD, and being the primary care-giver or having more burdensome care-giver commitments (Lilly et al., Reference Lilly, Laporte and Coyte2007; Bauer and Sousa-Poza, Reference Bauer and Sousa-Poza2015). These factors also apply to care-givers of PwD (e.g. Covinsky et al., Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001; Bakker et al., Reference Bakker, de Vugt, van Vliet, Verhey, Pijnenburg, Vernooij-Dassen and Koopmans2013; Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016). Again, interaction effects should be considered. Here, possible interrelations may occur among relationship, co-residence and care-giving intensity. Spousal care-givers living with the PwD often bear the care-giver responsibilities on their own if no other engaged care-giver lives nearby (Michalowsky et al., Reference Michalowsky, Thyrian, Eichler, Hertel, Wucherer, Flessa and Hoffmann2016). However, shared care-giving responsibilities between a spouse and a child of a PwD can relieve the affected household and maintain employment opportunities (Covinsky et al., Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001). Even after ruling out the endogeneity of the care-giving intensity, care-giving has a deterrent effect on a care-giver's employment, and this effect is mainly seen in the primary care-giver (Nguyen and Connelly, Reference Nguyen and Connelly2014). Additionally, in our review, evidence indicated that more hours of care-giving per day, and the duration of care-giving, led to a reduction of work in care-givers of PwD (Wilson et al., Reference Wilson, Van Houtven, Stearns and Clipp2007; Bakker et al., Reference Bakker, de Vugt, van Vliet, Verhey, Pijnenburg, Vernooij-Dassen and Koopmans2013). This finding is consistent with some studies focusing on care-giving in general, but contradicts others. For instance, if the caring responsibilities exceed ten hours per week, care-givers were more likely to reduce their work hours or to withdraw from the labour market (Lilly et al., Reference Lilly, Laporte and Coyte2007). On the other hand, Carr et al. (Reference Carr, Murray, Zaninotto, Cadar, Head, Stansfeld and Stafford2016) found no evidence of an association between the hours of care provided and exit from employment for both women and men. However, women who are responsible for high-intensity care (i.e. exceeding ten hours per week) are more likely to stop working over time than non-care-givers (Carr et al., Reference Carr, Murray, Zaninotto, Cadar, Head, Stansfeld and Stafford2016). In order to draw clear conclusions, further research is needed to clarify the association between the intensity of dementia care-giving and possible career disadvantages.
The burden of informal care-givers is one of the most well-studied outcome variables (Merrilees, Reference Merrilees2016). Burden also affects the work-life of employed care-givers. Psychological burdens such as role overload, worries and depression cause absence from work and conflicts at work (Edwards et al., Reference Edwards, Zarit, Stephens and Townsend2002; Dunham and Dietz, Reference Dunham and Dietz2003; Wilson et al., Reference Wilson, Van Houtven, Stearns and Clipp2007). Beyond this, perceived care-giving–work conflicts exert a significant influence on the burden of care-givers of PwD. Concurrent chronic illnesses of care-givers may exacerbate the situation (Wang et al., Reference Wang, Robinson and Carter-Harris2014). To prevent care-givers’ burden, dementia care-givers can derive benefit from leisure social activities (Schüz et al., Reference Schüz, Czerniawski, Davie, Miller, Quinn, King, Carr, Elliott, Robinson and Scott2015). Taking leave from care-giving is another common strategy to manage the burden (de la Cuesta-Benjumea, Reference de la Cuesta-Benjumea2011). To this end, working offers an opportunity because employment provides both a reprieve from care-giving and fulfilment (Eldh and Carlsson, Reference Eldh and Carlsson2011). Nevertheless, the experience of care-givers depends on internal factors such as resilience, self-efficacy, coping strategies and how they evaluate their responsibilities (Merrilees, Reference Merrilees2016). Employment may mean an additional strain, or a counterbalance for the care-giving burden at home. Based on the provided evidence of this review, care-givers of PwD who have high attentional control and seek formal support can experience fewer role conflicts (Morimoto et al., Reference Morimoto, Furuta, Kono and Kabeya2019). Moreover, they can gain positive work experiences (Edwards et al., Reference Edwards, Zarit, Stephens and Townsend2002) despite their perceived and evident strain from combining care-giving and working. Ties to other colleagues or clients at the workplace promote social participation of care-givers, which can positively influence their wellbeing (Cannuscio et al., Reference Cannuscio, Colditz, Rimm, Berkman, Jones and Kawachi2004; Nay et al., Reference Nay, Bauer, Fetherstonhaugh, Moyle, Tarzia and McAuliffe2015). Being capable of managing both roles enhances the satisfaction and happiness of care-givers in general (Eldh and Carlsson, Reference Eldh and Carlsson2011; van Campen et al., Reference van Campen, de Boer and Iedema2013). Care-givers of PwD also stated that working is a refuge from the demands of care-giving (Harris, Reference Harris1998; Dunham and Dietz, Reference Dunham and Dietz2003; Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012). For some women, the reduced value of work is an enrichment that re-aligns the balance between work and family life (Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012).
To summarise, socio-demographic factors have no specific relevance for care-givers of PwD, as they can also be observed in care-givers of persons without dementia as well as in the general population. However, care-giving-specific factors, in particular the intensity of care, apparently lead to greater career disadvantages among care-givers of PwD. Studies measured the intensity of care as the relational and local closeness to the care recipient, e.g. Covinsky et al. (Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001). Future studies should consider the time-commitment aspect of care-giving in greater depth, which can be permanent, as well as the availability and presence of all potential care-givers. Additionally, the interdependence between dementia care-giver burden and conflicts based on other responsibilities should be considered. Furthermore, informal care-giving should be seen in light of the cultural or religious background of those involved. In this review, we identified only one study (Kosberg et al., Reference Kosberg, Kaufman, Burgio, Leeper and Sun2007) that considered care-giver's ethnicity, which found no statistically significant influence on care-givers’ employment status. Another study found that the patient's ethnicity had a significant impact on the care-giver's employment status (Covinsky et al., Reference Covinsky, Eng, Lui, Sands, Sehgal, Walter, Wieland, Eleazer and Yaffe2001). Since care-giving dyads’ ethnicities and culture may influence dementia care-giving and care-givers’ outcomes such as burden (Etters et al., Reference Etters, Goodall and Harrison2008, Sun et al., Reference Sun, Ong and Burnette2012), country-specific or societal aspects might also affect care-givers’ work-life. Recently published literature on the reconciliation between informal care-giving and working has originated from different countries (e.g. New Zealand (Alpass et al., Reference Alpass, Keeling, Allen, Stevenson and Stephens2017) and Japan (Honda et al., Reference Honda, Date, Abe, Aoyagi and Honda2014)). Cross-national, original studies or reviews seem to be lacking. However, it might be of interest to examine in future research the impact of ethnicity, culture or religion on the reconciliation between informal (dementia) care-giving and working in more detail. This is because employment may not always be an additional strain for informal care-givers, but rather a counterbalance for care-giving strain at home. This possibility raises the questions as to which care-givers’ conditions affect concurrent care-giving and working, as well as boost or relieve dementia care-givers’ burden. In addition to care-givers’ characteristics and their potential interrelations, characteristics of the care recipient and circumstances of the care-giving context should also be considered, in order to account for the complexity of care-giving.
The facilitating effect of the care-giving context
Although different responsibilities within family and social life can be challenging, we emphasise the potential of other informal network members. Since care-givers value informal support more than formal support (Pinquart, Reference Pinquart and Suhr2016), the focus shifts to the involvement of family and social resources. Notably, the supportive potential of the family or other persons within the social environment has seldom been considered in studies using quantitative evidence (only in Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016), whereas qualitative studies have granted deeper insights into the topic. The family members of PwD share the same experiences within caring or supervision (Innes et al., Reference Innes, Abela and Scerri2011). Also, acquaintances who are going, or have gone, through similar situations can act as understanding and consoling partners (Dunham and Dietz, Reference Dunham and Dietz2003).
Various professional, supportive services exist and are used by informal care-givers of PwD. Employed care-givers of PwD are more likely to use paid services than non-employed care-givers (Schäufele et al., Reference Schäufele, Köhler, Hendlmeier and Suhr2016). This may indicate that employed care-givers are more able to afford these services, or that they appreciate continuing to work. In the long term, the utilisation of supportive services also has the potential to reduce the income losses of the care-giver (Gaugler et al., Reference Gaugler, Zarit, Townsend, Stephens and Greene2003). This finding emphasises the relevance of formal supportive services supplementing informal care, and even more so, where care-givers have used supportive services for a longer period of time. However, the service use of dementia care-givers depends not only on the care-giving requirements but also on their characteristics and needs, which may change over time. Care-givers who perceived a greater burden also use more services for themselves (Martindale-Adams et al., Reference Martindale-Adams, Nichols, Zuber, Burns and Graney2016). Thus, from a societal perspective, additional health care and service use by care-givers themselves must be reflected in measurements of dementia care costs (Deb et al., Reference Deb, Thornton, Sambamoorthi and Innes2017).
Finally, positive influencing factors may lie more in the care-giving context than in the affected care-givers or PwD. Detailed knowledge of these contextual factors of care-giving, which can usually be influenced, could lead to effective approaches to support informal care-givers if they are also employed. Satisfaction with social support enhances informal care-givers’ perceptions of dementia care-giving (Lee and Choi, Reference Lee and Choi2013), and self-help groups promote dementia care-givers’ mental health in general (Schüz et al., Reference Schüz, Czerniawski, Davie, Miller, Quinn, King, Carr, Elliott, Robinson and Scott2015). However, for employed care-givers of PwD, extensive evidence is still lacking. We conclude that the relevance of the informal network, including family members, has not been sufficiently investigated, although evidence to date suggests that they would hold a pivotal role in the support of care-givers. However, before researchers approach this particular topic, the implications of dementia on family life should be considered in more detail.
Successful combining of care-giving and employment contributes to sustaining informal care-giving in dementia
The effects on employment are evident, although we did not quantify their size due to the descriptive nature of this review. The many negative consequences described above illuminated the predominantly adverse impact of dementia care-giving on work-life; neutral or positive consequences were seldom reported. However, we would like to emphasise once again that some qualitative studies describe the compensatory and restorative effect of employment in informal dementia care-giving if both responsibilities can be combined (e.g. Dunham and Dietz, Reference Dunham and Dietz2003; Kohler et al., Reference Kohler, Döhner, Kofahl and Lüdecke2012). This integration of qualitative evidence yielded several nuanced findings that should be pursued by further mixed-methods or quantitative research approaches.
Despite the predominantly adverse impact of dementia care-giving on work-life, the overall employment rate is similar to the employment rates of care-givers in general. For example, the labour force participation rates of all informal care-givers in Germany grew between 2001 and 2012. In particular, the employment rate of female care-givers rose from approximately 37 per cent to 61 per cent, whereas the male employment rate increased from approximately 46 per cent to 67 per cent (Geyer and Schulz, Reference Geyer and Schulz2014). Although these increased employment rates were lower than those of non-care-givers’ employment rates, the difference was not statistically significant in all observed years. The number of both full-time and part-time or marginally working care-givers increased in the same period. The percentages of part-time and marginally employed care-givers were even higher than the percentages of the overall population of working age (Geyer and Schulz, Reference Geyer and Schulz2014). In contrast to the increased labour force participation rates, the average amount of time per day spent care-giving remained at almost three hours in this representative national sample of general care-givers (Geyer and Schulz, Reference Geyer and Schulz2014). We assume that increased working despite care-giving is compensated by the sacrifice of leisure time, with which comes potential consequences for the care-givers’ health. Therefore, this development is worthy of further investigation with a specific focus on dementia care-givers. However, further studies must consider interaction effects, such as the effects of care-giving and age, and control for these factors to avoid overestimating any effect. Decreased labour force participation and impaired working of care-givers of employment age not only imply financial productivity loss for care-givers of PwD but also losses for society in general. Dementia care-givers’ productivity loss from a societal perspective has already been covered in the literature using different measurements (e.g. Leicht and König, Reference Leicht and König2012; Lenox-Smith et al., Reference Lenox-Smith, Reed, Lebrec, Belger and Jones2016; Deb et al., Reference Deb, Thornton, Sambamoorthi and Innes2017).
Policy implications
To draw practical implications regarding the sub-group of dementia care-givers, we note that, on the one hand, these care-givers experience considerable career disadvantages. This effect has great importance because perceived care-giving–work conflicts are one of the greatest stressors leading to burden (Pinquart, Reference Pinquart and Suhr2016). This stressor is particularly seen, as we have shown, among working care-givers of PwD with severe cognitive impairments and who lived with the care recipient. In addition, they were mostly female, but this does not apply specifically to care-givers of PwD, but in general due to the gender distribution of care-giving responsibilities nowadays (Erol et al., Reference Erol, Brooker and Peel2015). On the other hand, concurrent working does not necessarily lead to exacerbated burden. Admittedly, more time at work may provide relief and counterbalance the adverse effects of care-giving (Pinquart, Reference Pinquart and Suhr2016). Combining care-giving with a paid job is associated with greater happiness (van Campen et al., Reference van Campen, de Boer and Iedema2013). Our results – based on the qualitative evidence – also hint at this effect in care-givers of PwD. Care-givers’ priorities are providing care, followed by paid employment and the ability to maintain a healthy and balanced life (Horrell et al., Reference Horrell, Breheny and Stephens2014). So, politicians and employers are asked to minimise career disadvantages caused by care-to-work or work-to-care conflicts, and to promote the counterbalancing effect of combining care-giving and working (e.g. Colombo et al., Reference Colombo, Llena-Nozal, Mercier and Tjadens2011).
Legal regulations should protect care-givers of PwD, so they do not fear adverse consequences of career disadvantages due to their care-giving responsibilities. Policies and laws greatly differ among different countries (Arksey and Morée, Reference Arksey and Morée2008; Hoff and Hamblin, Reference Hoff and Hamblin2011; Lilly, Reference Lilly2011). In Germany, for example, the regulations on Care-giver Leave and Family Care-giver Leave recently became effective. They offer family care-givers the right to take time off work for a specific period and to arrange work more flexibly during care-giving (Federal Minister for Family Affairs, Senior Citizens, Women and Youth, 2016). Similar regulations are included in the Family and Medical Leave Act in the USA, although they are considered improvable (Chen, Reference Chen2016). In contrast, legal regulations and workplace policies to support working family care-givers in China are still missing (Pei et al., Reference Pei, Luo, Lin, Keating and Fast2017). The dissemination of legislative efforts, comparable to those implemented in Germany, is desirable, and their efficacy should be scientifically assessed.
Furthermore, workplaces are and will be an essential source of support for employed care-givers. We have shown that employment provides reprieve and distraction from care-giving, fulfilment, self-confidence and social participation to care-givers of PwD. Employers should aim at developing and implementing care-giver-supportive work environments in which all employees enjoy the same degrees of respect and appreciation. Such care-giver-friendly workplace policies (CFWPs) are ‘intentional organisational changes, whether in practices, policies or culture, to support employees’ lives outside of work by reducing work–family conflict’ (Ramesh et al., Reference Ramesh, Ireson and Williams2017). Components of such a workplace can include (a) support services (e.g. resource and referral services, information services, counselling, support groups, workshops and seminars on care-giving issues), (b) flexible work arrangements (e.g. flexible work schedules, reduction of hours to part-time, job sharing, working from home or telecommuting-work), (c) financial assistance and relief (e.g. subsidised care-giving services), and (d) unpaid and paid leaves (Arksey, Reference Arksey2002; Hoff et al., Reference Hoff, Reichert, Hamblin, Perek-Bialas and Principi2014; Ireson et al., Reference Ireson, Sethi and Williams2016, Ramesh et al., Reference Ramesh, Ireson and Williams2017). Care-giver-friendly employers should have in mind that employees aged 40 or more, especially women, could be faced with already existing or future care-giving responsibilities. They should inform them of their options and support them. Especially among women (Schneider et al., Reference Schneider, Trukeschitz, Mühlmann and Ponocny2013) and care-givers with intermittent care responsibilities (Brown and Pitt-Catsouphes, Reference Brown and Pitt-Catsouphes2013), flexible work arrangements play an important role in experiencing fewer care-giving–work interactions and reduced burden. Further recommendations can include training for managers and supervisors to promote a friendly atmosphere for employed care-givers. For instance, open-door and guaranteed confidentiality policies between employers and employees can be established to foster communication between them, and reduce possible prejudices and reservations regarding CFWPs. Visible CFWPs will become an increasingly important part of business and management plans geared towards sustainability (Ramesh et al., Reference Ramesh, Ireson and Williams2017). However, more detailed knowledge of how workplaces can be transformed into care-giver-supportive work environments is necessary (Lilly, Reference Lilly2011; Ramesh et al., Reference Ramesh, Ireson and Williams2017).
Reducing the burden of dementia care-givers is a global political objective and promising efforts already exist (Livingston et al., Reference Livingston, Sommerlad, Orgeta, Costafreda, Huntley, Ames, Ballard, Banerjee, Burns, Cohen-Mansfield, Cooper, Fox, Gitlin, Howard, Kales, Larson, Ritchie, Rockwood, Sampson, Samus, Schneider, Selbæk, Teri and Mukadam2017). Employed care-givers of PwD are a sub-group of critical importance because of the presumed double burden if political and social actors do not address care-to-work or work-to-care conflicts. The common goal of legal regulations and workplace policies should be the successful combination of care-giving and working. When we achieve this, it may enhance care-givers’ satisfaction, sustain informal care-giving in dementia and reduce productivity loss.
Strengths and weaknesses
The first strength of this mixed-studies review is the provision of rich contextual details of this complex topic for the first time, in a systematic manner. By considering mixed evidence, we highlight the qualitative results that are available that complement quantitative results. The second strength is that we have identified two neglected research areas related to the interplay between informal care-giving and employment. Firstly, if we understand informal care-giving as a societal task with shared responsibilities, we should look in depth at the potential of the informal network (i.e. relatives, friends, neighbours) to influence the balance of employment and care-giving among informal care-givers. Their support could be a valuable contribution to the mitigation of the strain arising from care-giving and could facilitate the care-givers’ participation in the labour market. Secondly, care-givers’ characteristics, such as personality traits and coping skills, play an essential role in the mastering of both care-giving and working. Recently published findings provided initial evidence for this role (Morimoto et al., Reference Morimoto, Furuta, Kono and Kabeya2019); based on this, further research is needed. Perspectives on care-giving should be broadened to account for the fact that informal care-giving in dementia also offers the opportunity for personal growth (Leipold et al., Reference Leipold, Schacke and Zank2006; Ott et al., Reference Ott, Sanders and Kelber2007; Shim et al., Reference Shim, Barroso, Gilliss and Davis2013). Both practical and psychological services – particularly counselling and educational services (Piersol et al., Reference Piersol, Canton, Connor, Giller, Lipman and Sager2017), but also specialist support (Bunn et al., Reference Bunn, Goodman, Pinkney and Drennan2016) for informal care-givers of PwD, are necessary to support their highly valuable care responsibilities.
Weaknesses of this mixed-studies review include the narratively synthesised evidence provided, limitations of the included studies, the possibility of publication bias and the sensitivity of the literature search approach, as well as study selection. We provided interpretive evidence derived from narrative data synthesis. Based on the enormous heterogeneity of the designs, methods and sample characteristics of the included studies, fair comparisons were not possible and pooling of data was not feasible. The included studies are limited given the majority of quantitative studies used cross-sectional data. Therefore, no causalities between care-giving-related exposures and employment-related outcomes could be drawn. Future studies with longitudinal follow-up are suggested to explore causal relationships. Publication bias could also have influenced our results, as the results of no effects of informal care-giving on care-givers’ employment are less likely to be published. We can further presume that the researchers’ perspective has been focused more on the adverse effects on employment than on positive work experiences due to the presumed care-giving–work conflict. The sensitivity of our search strategy and study selection was high in order to gain a broader picture. Therefore, we accounted for the complexity of this topic, rather than providing a brief outline enabled by higher specificity. We built search terms on limited phrases, screened a considerable number of electronic databases (which was simplified by using one meta-database including 11 internal databases and ten external databases) and all screening steps were conducted by two reviewers. Nevertheless, we cannot exclude the possibility of unidentified studies. Additionally, we did not assess the disease severity of the observed care recipients with Alzheimer's disease or related dementia, how informal care-giving was defined by the studies nor how the observed care arrangements were organised. The majority of included studies originated from North American and European countries. However, how health-care systems and circumstances arrange informal care for an elderly or impaired related person differ strikingly from country to country. Thus, our conclusions should be interpreted with caution in terms of country-specific conclusions. Lastly, we solely focused on informal care-giving factors and excluded working conditions that also influence care-givers’ employment.
Conclusion
The results of this mixed-studies review suggest that the effects of care-giving for PwD on care-givers’ work-life are mostly negative. However, they also include a promising finding that care-giving and working at the same time does not necessarily lead to care-giving–work conflicts and increased burden. Employment can appear as a relief or a counterbalance for care-giving strain. Managing both care-giving and working can be satisfying and improve care-givers’ self-efficacy. Additionally, new important questions arise. For example, (a) how strong is the effect of care recipients’ dementia on care-givers’ work-life compared to care-givers of patients without dementia? (b) Which internal and external factors are responsible for the successful combination of care-giving and employment or for increasing or relieving the burden of employed care-givers of PwD? Future research could concentrate on the impact of other informal network members on the work-life of informal care-givers, as this group has not been considered in many investigations to date. Furthermore, future longitudinal studies are also suggested to analyse the relationship between informal care-giving in dementia and care-givers’ employment in greater detail. The relevance of such research is evidenced by the urgent need to develop interventions aimed at the successful combination of care-giving and employment to ensure that informal care-giving in dementia and care-givers’ labour force participation can be sustained.
Author contributions
LN and CB developed the concept of the study. LN and CM designed and conducted the literature search and data extraction. LN, H-HK, CM and CB contributed to the analysis and interpretation of the information. LN drafted the manuscript. H-HK, CM and CB revised the manuscript critically for important intellectual content. All authors approved the final version of the manuscript.
Financial support
This work was supported by the German Federal Ministry of Education and Research (grant number 01EH1601A). The funding source took no part in the design of the study or collection, analysis and interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication. The views expressed are those of the authors.
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
Not applicable.









 Open access
Open access