
Abstract
Background:
Podocalyxin-like 1 (PODXL) is a cell-adhesion glycoprotein and stem cell marker that has been associated with an aggressive tumour phenotype and poor prognosis in several forms of cancer. In this study, we investigated the prognostic impact of PODXL expression in colorectal cancer (CRC).
Methods:
Using tissue microarrays and immunohistochemistry, PODXL expression was evaluated in 536 incident CRC cases from a prospective, population-based cohort study. Kaplan–Meier analysis and Cox proportional hazards modelling were used to assess the impact of PODXL expression on cancer-specific survival (CSS) and overall survival (OS).
Results:
High PODXL expression was significantly associated with unfavourable clinicopathological characteristics, a shorter CSS (hazard ratio (HR)=1.98; 95% confidence interval (CI) 1.38–2.84, P<0.001) and 5-year OS (HR=1.85; 95% CI 1.29–2.64, P=0.001); the latter remaining significant in multivariate analysis (HR=1.52; 95% CI 1.03–2.25, P=0.036). In addition, in curatively resected stage III (T1–4, N1–2, M0) patients (n=122) with tumours with high PODXL expression, a significant benefit from adjuvant chemotherapy was demonstrated (pinteraction =0.004 for CSS and 0.015 for 5-year OS in multivariate analysis).
Conclusion:
Podocalyxin-like 1 expression is an independent factor of poor prognosis in CRC. Our results also suggest that PODXL may be a useful marker to stratify patients for adjuvant chemotherapy.
Similar content being viewed by others

Main
Colorectal cancer (CRC) is one of the most common types of human cancer worldwide with ∼1 million new cases detected every year (Parkin et al, 2005). Early detection, adequate surgical excision and optimal use of adjuvant treatment are of critical importance for the clinical outcome. Currently, tumour stage at diagnosis is the most important prognostic factor in CRC. Adjuvant treatment is recommended for patients with stage III and high-risk stage II disease (e.g. T4, tumour perforation, insufficient lymph node staging). Many efforts have been made to find molecular markers to identify high-risk disease and to select patients for adjuvant treatment, but so far, none of them have proven good enough for use in clinical routine.
Podocalyxin-like 1 (PODXL) is an anti-adhesive transmembrane protein belonging to the CD34 family. Podocalyxin-like 1 inhibits cell–cell interaction through charge-repulsive effects and has classically been ascribed to haematopoetic progenitor cells (Doyonnas et al, 2005), vascular endothelial cells (Horvat et al, 1986) and in the renal glomerular podocytes where it has a vital part in maintaining filtration pathways (Doyonnas et al, 2001). In recent years, overexpression of PODXL has been found in several different forms of cancer including breast and prostate cancer, malignant brain tumours, testicular, hepatocellular and renal cell carcinoma (Gregoire et al, 1995; Schopperle et al, 2003; Chen et al, 2004; Somasiri et al, 2004; Casey et al, 2006; Hayatsu et al, 2008; Koch et al, 2008; Hsu et al, 2010; Cheung et al, 2011). In breast cancer and renal cell carcinoma, high expression of PODXL has been demonstrated to be an independent predictor of poor prognosis (Somasiri et al, 2004; Hsu et al, 2010). The mechanisms behind these observations are not fully understood, but PODXL has been shown to interact with other proteins such as ezrin, an established mediator of metastasis, in prostate cancer cells (Casey et al, 2006) and to induce actin recruitment and microvillus formation in breast cancer cells (Nielsen et al, 2007). In addition, a recent study demonstrated that PODXL is a target of the tumour suppressive miRNA-199a and that cellular depletion of PODXL in testicular tumours results in suppression of cancer invasion (Cheung et al, 2011). Podocalyxin-like 1 also has an important role in epithelial-mesenchymal transition (EMT), a process involved in initiating the invasive and metastatic behaviour of epithelial cancer cells, by regulating and interacting with collagen type 1, E-cadherin and vimentin (Meng et al, 2011).
Podocalyxin-like 1 has been found to be expressed in several CRC cell lines (Ito et al, 2007), but we are not aware of any previous publication describing the prognostic impact of PODXL expression in human CRC. In this study, we examined the prognostic value of PODXL expression in tissue microarrays (TMAs) representing tumours from 536 incident cases of CRC in the prospective, population-based cohort Malmö Diet and Cancer Study. The results demonstrate that PODXL expression is associated with unfavourable clinicopathological characteristics and an independent predictor of poor prognosis.
Materials and methods
The Malmö Diet and Cancer Study
The Malmö Diet and Cancer Study (MDCS) is an ongoing population-based prospective cohort study with the primary aim to examine whether a Western diet rich in fat and low in fruit and vegetables increases the risk of certain forms of cancer (Berglund et al, 1993). Between 1991 and 1996, a total number of 28 098 individuals, 11 063 (39.4%) men and 17 035 (60.6%) women between 44 and 74 years where enrolled (from a background population of 74 138). Follow-up is done annually by record linkage to national registries for cancer and cause of death.
Approval for the MDCS (Ref. 51/90) and the present study (Ref. 530/2008) were obtained from the Ethics Committee at Lund University.
Incident cases of CRC until 31 December 2008
Until the end of follow-up 31 December 2008, 626 incident cases of CRC had been registered in the study population. Cases were identified from the Swedish Cancer Registry up until 31 December 2007, and from The Southern Swedish Regional Tumour Registry for the period of 1 January to 31 December 2008. All tumours with available slides and/or paraffin blocks were histopathologically re-evaluated on haemotoxylin and eosin-stained slides. Histopathological, clinical and treatment data were obtained from clinical and/or pathology records. TNM staging was performed according to the American Joint Committee on Cancer (AJCC).
Information on vital status and cause of death were obtained from the Swedish Cause of Death Registry up until 31 December 2009. Follow-up started at the date of diagnosis and ended at death, emigration or 31 December 2009, whichever came first. Patient and tumour characteristics are summarised in Supplementary Table 1.
TMA construction
Tumours with an insufficient amount of material were excluded, and a total number of 557 (89%) tumours were suitable for TMA construction. Areas representative of cancer were then marked on haematoxylin and eosin-stained slides and TMAs were constructed as previously described (Kononen et al, 1998). In brief, two 1.0 mm cores were taken from each tumour and mounted in a new recipient block using a semi-automated arraying device (TMArrayer, Pathology Devices, Westminster, MD, USA).
Immunohistochemistry and antibody validation
For immunohistochemical analysis, 4 μm TMA sections were automatically pre-treated using the PT-link system (DAKO, Glostrup, Denmark) and then stained in an Autostainer Plus (DAKO) with the affinity-purified polyclonal anti-PODXL antibody HPA 2110 (Atlas Antibodies, Stockholm, Sweden, diluted 1:250). The Envision Flex/HRP (K8010) kit (DAKO) was used for visualisation of the staining. The specificity of this antibody, originally generated within the Human Protein Atlas (HPA) project, has been validated using western blotting and protein arrays and PODXL protein expression has been mapped by immunohistochemistry in 48 types of normal tissues and 20 common cancers (Uhlen et al, 2005; Ponten et al, 2008) (www.proteinatlas.org). The same antibody has also been used to detect PODXL expression in testicular carcinoma in a recent study (Cheung et al, 2011).
To control for heterogenous expression patterns, IHC was also performed on full-face sections from 10 randomly selected cases denoted as having negative PODXL expression and 10 cases with high (score 3–4) PODXL expression.
Evaluation of PODXL staining
Podocalyxin-like 1 was expressed in the cytoplasm of the tumour cells, with an accentuation towards the membrane in some cases. No expression was seen in the nuclei. The expression was recorded as negative (0), weakly positive in any proportion of cells (1), moderately positive in any proportion (2), positive with distinct membranous pattern in ⩽50% of cells (3) and positive with distinct membranous pattern in > 50% of cells (4). The staining was evaluated by two independent observers (AL and KJ) who were blinded to clinical and outcome data. Scoring differences were discussed in order to reach consensus.
Statistical analysis
For statistical purposes, categories of PODXL expression were trichotomised into negative (0), weak-moderate (1–2) and strong (3–4) PODXL staining or dichotomised into low (0–2) and high (3–4). Spearman's Rho and χ2-tests were used for comparison of PODXL expression and relevant clinicopathological characteristics. Kaplan–Meier analysis and log rank test were used to illustrate differences in cancer specific survival (CSS) and overall survival (OS) according to PODXL expression. Cox regression proportional hazards models were used for estimation of hazard ratios (HRs) for death from CRC and overall causes according to PODXL expression in both uni- and multivariate analysis, adjusted for age, gender, TNM status, differentiation grade and vascular invasion. A backward conditional selection method was used for variable selection by the model. The interaction between PODXL expression and adjuvant chemotherapy was explored by a Cox model including a treatment variable and an interaction variable. All tests were two-sided. A P-value <0.05 was considered significant. All statistical analyses were performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA).
REMARK criteria
A description of the fulfilment of REMARK criteria (McShane et al, 2005) for biomarker studies is provided in Supplementary Table 2.
Results
PODXL expression in CRC
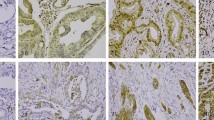
Following antibody optimisation and staining, PODXL expression could be evaluated in 536 of the 557 (96.2%) of the tumours represented in the TMA. A total of 268 tumours (50.0%) were negative for PODXL, 196 (36.6%) displayed weak-moderate staining and 72 (13.4%) strong staining for PODXL. As endothelial cells express PODXL, entrapped vessels served as internal positive control. Representative IHC images are shown in Figure 1 A–F. Notably, in the majority of cases denoted as positive, PODXL was distinctly expressed in scattered invasive cells at the tumour front, corresponding morphologically with tumour budding (Prall, 2007) (Figure 1D and E). Only one tumour (0.2%) had a strong, distinct positive staining in >50% of tumour cells, as visualised in Figure 1F. Podocalyxin-like 1 expression in full-face sections (n=20) correlated with the TMA-based scoring in all cases, including the tumour in Figure 1F, further supporting the selective distribution of PODXL-expressing cells in the majority of positive tumours.

Immunohistochemical images of PODXL staining representing colorectal tumours with (A) negative, (B) weak, (C) moderate, and (D–F) strong, membranous staining in a varying proportion of tumour cells. All images are captured at × 20 magnification.
Association between PODXL expression and clinicopathological characteristics
Analysis of the relationship between PODXL expression and established clinicopathological parameters revealed a strong correlation between high PODXL expression and more advanced T-stage (P<0.001), N-stage (P<0.001), M-stage (P=0.009), low differentiation grade (P<0.001) and presence of vascular invasion (P=0.008) (Table 1). There was no significant association between PODXL expression and age at diagnosis, gender or tumour location (Table 1).
Association between PODXL expression and survival
Kaplan–Meier analysis revealed that PODXL expression correlated with a significantly shorter CSS and OS, with the worst outcome for tumours with high PODXL expression (Figure 2). These findings were confirmed in univariate Cox regression analysis using a dichotomised variable of low (0–2) and high (3–4) PODXL expression (HR=1.98; 95% confidence interval (CI) 1.38–2.84, P<0.001 for CSS and HR=1.85; 95% CI 1.29–2.64, P=0.001 for 5-year OS), and remained significant for 5-year OS in multivariate analysis (HR=1.52; 95% CI 1.03–2.25, P<0.036) and borderline significant for CSS (HR=1.57; 95% CI 0.99–2.18, P=0.055), adjusted for age, gender, TNM status, differentiation grade and vascular invasion (Table 2). Podocalyxin-like 1 expression was also significantly associated with long-term OS, both in univariate analysis (HR=1.97; 95% CI 1.41–2.74, P<0.001) and multivariate analysis (HR=1.57; 95% CI 1.10–2.25, P=0.014).

High expression of PODXL is associated with a poor outcome in colorectal cancer patients. Kaplan–Meier analysis of (A) colorectal cancer-specific survival and (B) overall survival according to PODXL expression.
Impact of PODXL expression on survival in relation to adjuvant chemotherapy
The impact of PODXL expression on survival in relation to adjuvant treatment was analysed in 122 curatively resected stage III (T1–4, N1–2, M0) patients, of whom 62 (50.8%) had received adjuvant treatment and 60 (49.2%) had not. Kaplan–Meier analysis in strata according to treatment and PODXL expression demonstrated that patients having tumours with high PODXL expression who were treated with adjuvant chemotherapy had a similar CSS (Figure 3A) and OS (Figure 3B) as patients with low PODXL-expressing tumours. Untreated patients with tumours with high PODXL expression, however, had a significantly shorter CSS and OS (Figure 3A and B). Cox interaction analysis (Table 3) demonstrated that the P-value for the unadjusted interaction variable between treatment and PODXL status was 0.044 for 5-year OS, suggesting that patients having tumours with high expression of PODXL had benefited from adjuvant chemotherapy, whereas patients with low PODXL-expressing tumours did not benefit from adjuvant treatment. In addition, when adjusted for established prognostic factors, the term of interaction was significant for both CSS (P=0.004) and 5-year OS (P=0.015) (Table 3). The treatment benefit was similar for 5-fluorouracil alone or in combination with oxaliplatin (data not shown).

Kaplan–Meier estimates of (A) colorectal cancer-specific and (B) overall survival according to combinations of PODXL expression (high or low) and adjuvant chemotherapy (CT). Log rank P-values correspond to pairwise comparisons of PODXL high and untreated tumours with the other strata. Log rank P-values for overall survival (B) are given both for 5-year survival (in parentheses) and long-term survival.
In patients with stage II disease (n=205), high PODXL expression was associated with a significantly shorter OS (HR=3.03; 95% CI 1.45–6.34, P=0.003) and 5-year OS (HR=2.83; 95% CI 1.14–7.16, P=0.025), whereas the association with CSS did not reach significance (HR=2.19; 95% CI 0.84–5.75, P=0.11). Information on adjuvant chemotherapy was available for 170 patients with stage II disease, of whom only 13 (6.2%) had received treatment, an insufficient number to allow for analysis of a potential treatment benefit related to PODXL status in this group.
Discussion
Our results demonstrate that overexpression of PODXL in CRC is associated with unfavourable clinicopathological characteristics and an independent factor of poor prognosis. This is to our knowledge the first report on the prognostic value of PODXL expression in human CRC and the results are based on a large number of patients (n=536) from a prospective cohort study.
In our study, 13% of the tumours were denoted as having high expression of PODXL. In a previous study on breast cancer, using a somewhat different cutoff, high expression of PODXL was found in 6% of the tumours (Somasiri et al, 2004). These data, together with the results from the antibody-based screening in the Human Protein Atlas, demonstrate that, in most cancer types, while upregulated compared with the corresponding normal tissue, PODXL is overexpressed in a relatively small proportion of cases.
In the vast majority of tumours with high PODXL expression, defined as a distinct cytoplasmic/membranous staining pattern, this was predominantly observed in a subset of scattered and infiltrating cells at the invasive tumour front. These findings are substantiated by previous studies demonstrating that overexpression of PODXL enhances migratory and invasive properties of tumour cells (Casey et al, 2006; Nielsen et al, 2007). Notably, the only patient in this study with a tumour displaying PODXL expression in >50% of the cells had generalised disease and died within a month of diagnosis, further supporting that PODXL expression is associated with an invasive and metastatic cellular phenotype in CRC in vivo. Moreover, the upregulation of PODXL expression observed at the infiltrating edge of the tumour corresponds well to the morphological term ‘tumour budding’, which has been demonstrated to be of prognostic importance (Hase et al, 1993; Prall, 2007), and biologically closely related to EMT (Prall, 2007). Studies have demonstrated that cancer cells at the invasive front of primary tumours can convert to a motile mesenchymal phenotype (Yang and Weinberg, 2008) and these cells are considered to be the cells with metastatic potential. Along this line, a high expression of PODXL has been recorded in TGFβ-induced EMT (Meng et al, 2011) indicating that PODXL has an integral role in cancer progression.
Moreover, studies have illustrated a link between EMT and the gain of stem cell-like properties such as mobility, anti-apoptosis circuitry and low level of differentiation, which are traits of great value for a malignant tumour (Mani et al, 2008). The PODXL has previously been suggested as a marker for embryonal carcinoma stem cells and haematopoietic stem cells (Schopperle et al, 2003) and found to be upregulated in tumour stem cells in glioblastoma (He et al, 2010).
In the light of these results, the development of therapies targeting PODXL has been proposed as a new treatment strategy (Chen et al, 2004; Somasiri et al, 2004). Our results, however, indicate that colorectal tumours with high expression of PODXL also respond well to standard chemotherapy. Adjuvant chemotherapy reduces the risk of relapse but it also has side effects and can be difficult to tolerate, especially for older patients. In CRC Stage III, the recurrence-free survival increases with 10–20% by adding adjuvant chemotherapy and in stage II the incremental gain is only around 5%. Thus, only a minority of patients receiving adjuvant chemotherapy have any benefit from it. Therefore, it would be of great clinical value to find predictive tools for a better selection of patients to such treatment.
The present study indicates that PODXL might be used as a predictive marker for adjuvant treatment of CRC. In stage III, patients with high tumour PODXL expression were the ones who benefited from adjuvant chemotherapy, whereas patients having tumours with low PODXL expression did not seem to have any effect from the treatment. Whether the same is true in stage II could not be determined in our study, as the number of stage II patients that received adjuvant chemotherapy was too low for statistical analyses.
Even though the positive impact of chemotherapy in the tumours with high PODXL expression remained significant in multivariate analysis after correction for other prognostic factors, our findings must be interpreted with caution as this was an observational cohort study in which a potential selection bias compared with the general population must be taken into consideration (Berglund et al, 1993). The distribution of clinical stages at diagnosis was, however, in line with the expected.
It is notable that only ∼half of the patients with stage III tumours in our study received adjuvant treatment, which is on the low side compared with modern therapeutic guidelines. The main reason for this is most likely that this study started already in the mid 90s, during which time adjuvant chemotherapy was not yet standard of care in Sweden.
In this study, CRC-specific survival and OS were used as endpoints as this information had been recorded prospectively and therefore was available for all patients. In future studies, the impact of PODXL expression on recurrence free survival should also be assessed, preferably in cohorts where this information has been recorded prospectively. It will also be of value to correlate PODXL expression to other relevant molecular characteristics of CRC, for example, microsatellite instability status, KRAS, BRAF and PIK3C mutations.
In summary, the results from this large cohort study suggest that PODXL expression is independently associated with a poor prognosis in CRC. Our findings also suggest that adjuvant chemotherapy should be given to patients with tumours expressing high levels of PODXL, whereas patients with low PODXL-expressing tumours could be spared such treatment. Future prospective studies are needed to confirm this association as well as to elucidate the exact mechanisms by which PODXL affects tumour behaviour.
References
Berglund G, Elmstahl S, Janzon L, Larsson SA (1993) The malmo diet and cancer study. Design and feasibility. J Intern Med 233: 45–51
Casey G, Neville PJ, Liu X, Plummer SJ, Cicek MS, Krumroy LM, Curran AP, McGreevy MR, Catalona WJ, Klein EA, Witte JS (2006) Podocalyxin variants and risk of prostate cancer and tumor aggressiveness. Hum Mol Genet 15: 735–741
Chen X, Higgins J, Cheung ST, Li R, Mason V, Montgomery K, Fan ST, van de Rijn M, So S (2004) Novel endothelial cell markers in hepatocellular carcinoma. Mod Pathol 17: 1198–1210
Cheung HH, Davis AJ, Lee TL, Pang AL, Nagrani S, Rennert OM, Chan WY (2011) Methylation of an intronic region regulates miR-199a in testicular tumor malignancy. Oncogene; e-pub ahead of print 7 March 2011; doi: 10.1038/onc.2011.60
Doyonnas R, Kershaw DB, Duhme C, Merkens H, Chelliah S, Graf T, McNagny KM (2001) Anuria, omphalocele, and perinatal lethality in mice lacking the CD34-related protein podocalyxin. J Exp Med 194: 13–27
Doyonnas R, Nielsen JS, Chelliah S, Drew E, Hara T, Miyajima A, McNagny KM (2005) Podocalyxin is a CD34-related marker of murine hematopoietic stem cells and embryonic erythroid cells. Blood 105: 4170–4178
Gregoire M, Schopperle WM, DeWolf WC (1995) Distinct glycoforms of a tumor specific glycoprotein, gp200, in human testis and testicular tumors. J Urol 154: 275–277
Hase K, Shatney C, Johnson D, Trollope M, Vierra M (1993) Prognostic value of tumor ‘budding’ in patients with colorectal cancer. Dis Colon Rectum 36: 627–635
Hayatsu N, Kaneko MK, Mishima K, Nishikawa R, Matsutani M, Price JE, Kato Y (2008) Podocalyxin expression in malignant astrocytic tumors. Biochem Biophys Res Commun 374: 394–398
He J, Liu Y, Xie X, Zhu T, Soules M, DiMeco F, Vescovi AL, Fan X, Lubman DM (2010) Identification of cell surface glycoprotein markers for glioblastoma-derived stem-like cells using a lectin microarray and LC-MS/MS approach. J Proteome Res 9: 2565–2572
Horvat R, Hovorka A, Dekan G, Poczewski H, Kerjaschki D (1986) Endothelial cell membranes contain podocalyxin--the major sialoprotein of visceral glomerular epithelial cells. J Cell Biol 102: 484–491
Hsu YH, Lin WL, Hou YT, Pu YS, Shun CT, Chen CL, Wu YY, Chen JY, Chen TH, Jou TS (2010) Podocalyxin EBP50 ezrin molecular complex enhances the metastatic potential of renal cell carcinoma through recruiting Rac1 guanine nucleotide exchange factor ARHGEF7. Am J Pathol 176: 3050–3061
Ito T, Maki N, Hazeki O, Sasaki K, Nekooki M (2007) Extracellular and transmembrane region of a podocalyxin-like protein 1 fragment identified from colon cancer cell lines. Cell Biol Int 31: 1518–1524
Koch LK, Zhou H, Ellinger J, Biermann K, Holler T, von Rucker A, Buttner R, Gutgemann I (2008) Stem cell marker expression in small cell lung carcinoma and developing lung tissue. Hum Pathol 39: 1597–1605
Kononen J, Bubendorf L, Kallioniemi A, Barlund M, Schraml P, Leighton S, Torhorst J, Mihatsch MJ, Sauter G, Kallioniemi OP (1998) Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat Med 4: 844–847
Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan A, Zhou AY, Brooks M, Reinhard F, Zhang CC, Shipitsin M, Campbell LL, Polyak K, Brisken C, Yang J, Weinberg RA (2008) The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell 133: 704–715
McShane LM, Altman DG, Sauerbrei W, Taube SE, Gion M, Clark GM (2005) Reporting recommendations for tumor marker prognostic studies. J Clin Oncol 23: 9067–9072
Meng X, Ezzati P, Wilkins JA (2011) Requirement of podocalyxin in TGF-beta induced epithelial mesenchymal transition. PLoS ONE 6: e18715
Nielsen JS, Graves ML, Chelliah S, Vogl AW, Roskelley CD, McNagny KM (2007) The CD34-related molecule podocalyxin is a potent inducer of microvillus formation. PLoS One 2: e237
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55: 74–108
Ponten F, Jirstrom K, Uhlen M (2008) The Human Protein Atlas--a tool for pathology. J Pathol 216: 387–393
Prall F (2007) Tumour budding in colorectal carcinoma. Histopathology 50: 151–162
Schopperle WM, Kershaw DB, DeWolf WC (2003) Human embryonal carcinoma tumor antigen, Gp200/GCTM-2, is podocalyxin. Biochem Biophys Res Commun 300: 285–290
Somasiri A, Nielsen JS, Makretsov N, McCoy ML, Prentice L, Gilks CB, Chia SK, Gelmon KA, Kershaw DB, Huntsman DG, McNagny KM, Roskelley CD (2004) Overexpression of the anti-adhesin podocalyxin is an independent predictor of breast cancer progression. Cancer Res 64: 5068–5073
Uhlen M, Bjorling E, Agaton C, Szigyarto CA, Amini B, Andersen E, Andersson AC, Angelidou P, Asplund A, Asplund C, Berglund L, Bergstrom K, Brumer H, Cerjan D, Ekstrom M, Elobeid A, Eriksson C, Fagerberg L, Falk R, Fall J, Forsberg M, Bjorklund MG, Gumbel K, Halimi A, Hallin I, Hamsten C, Hansson M, Hedhammar M, Hercules G, Kampf C, Larsson K, Lindskog M, Lodewyckx W, Lund J, Lundeberg J, Magnusson K, Malm E, Nilsson P, Odling J, Oksvold P, Olsson I, Oster E, Ottosson J, Paavilainen L, Persson A, Rimini R, Rockberg J, Runeson M, Sivertsson A, Skollermo A, Steen J, Stenvall M, Sterky F, Stromberg S, Sundberg M, Tegel H, Tourle S, Wahlund E, Walden A, Wan J, Wernerus H, Westberg J, Wester K, Wrethagen U, Xu LL, Hober S, Ponten F (2005) A human protein atlas for normal and cancer tissues based on antibody proteomics. Mol Cell Proteomics 4: 1920–1932
Yang J, Weinberg RA (2008) Epithelial-mesenchymal transition: at the crossroads of development and tumor metastasis. Dev Cell 14: 818–829
Acknowledgements
This study was supported by grants from the Knut and Alice Wallenberg Foundation, the Swedish Cancer Society, Gunnar Nilsson's Cancer Foundation, the Crafoord Foundation and the Research Funds of Skåne University Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on British Journal of Cancer website
Supplementary information
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Larsson, A., Johansson, M., Wangefjord, S. et al. Overexpression of podocalyxin-like protein is an independent factor of poor prognosis in colorectal cancer. Br J Cancer 105, 666–672 (2011). https://doi.org/10.1038/bjc.2011.295
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2011.295
Keywords
This article is cited by
-
Podocalyxin promotes the formation of compact and chemoresistant cancer spheroids in high grade serous carcinoma
Scientific Reports (2024)
-
CAR T cells redirected against tumor-specific antigen glycoforms: can low-sugar antigens guarantee a sweet success?
Frontiers of Medicine (2022)
-
Impact of histological response after neoadjuvant therapy on podocalyxin as a prognostic marker in pancreatic cancer
Scientific Reports (2021)
-
PODXL might be a new prognostic biomarker in various cancers: a meta-analysis and sequential verification with TCGA datasets
BMC Cancer (2020)
-
Additive clinical impact of epidermal growth factor receptor and podocalyxin-like protein expression in pancreatic and periampullary adenocarcinomas
Scientific Reports (2020)
