
Abstract
Background:
Despite several years of research and attempts to develop prognostic models a considerable fraction of stage II colon cancer patients will experience relapse within few years from their operation. The aim of the present study was to investigate the prognostic importance of miRNA-21 (miR-21), quantified by in situ hybridisation, in a unique, large population-based cohort.
Patients and methods:
The study included 764 patients diagnosed with stage II colon cancer in Denmark in the year 2003. One section from a representative paraffin-embedded tumour tissue specimen from each patient was processed for analysis of miR-21 and quantitatively assessed by image analysis.
Results:
The miR-21 signal was predominantly observed in fibroblast-like cells located in the stromal compartment of the tumours. We found that patients expressing high levels of miR-21 had significantly inferior recurrence-free cancer-specific survival (RF-CSS): HR=1.26; 95% CI: 1.15–1.60; P<0.001. In Cox regression analysis, a high level of miR-21 retained its prognostic importance and was found to be significantly related to poor RF-CSS: HR=1.41; 95% CI: 1.19–1.67; P<0.001.
Conclusion:
The present study showed that increasing miR-21 expression levels were significantly correlated to decreasing RF-CSS. Further investigations of the clinical importance of miR-21 in the selection of high-risk stage II colon cancer patients are merited.
Similar content being viewed by others
Main
Colon cancer represents a major challenge all over the Western World (Parkin et al, 2005). The incidence has been increasing for decades but screening holds the promise of a shift in distribution towards earlier stages (Gross et al, 2006). Surgery is a cornerstone in the treatment, but with operation alone a considerable fraction of patients will experience tumour recurrence, calling for adjuvant chemotherapy. Stage II (no lymph node metastases or distant metastases) patients represent about 25% of all cases and they have a 5-year overall survival (OS) of 73–85%, when surgically resected (O'Connell, 2004).
There is a general agreement on postoperative chemotherapy for stage III colon cancer patients, but there is still a debate on this approach for patients with stage II tumours. Meta-analyses, reviews and international guidelines agree that adjuvant chemotherapy should be offered to a subgroup of patients with high risk of recurrence, including T4 and T3 tumours with lymphovascular invasion, high malignancy grade, perforation and/or inadequate lymph node sampling (Benson III et al, 2004; Figueredo et al, 2008; Kopetz et al, 2008; Bastos et al, 2010; Gangadhar and Schilsky, 2010; Lombardi et al, 2010). Interestingly, the recent CALBG 9581 study of 24 000 stage II patients from the Medicare Registry found no improvement in 5-year survival in patients receiving adjuvant chemotherapy, irrespective of a division of patients into two groups with high- or low-risk characteristics (O’Connor et al, 2011). These results question the current clinical practice and underline the urgent need of new and reliable prognostic and predictive markers in stage II colon cancer.
MicroRNAs (miRNAs) comprise an abundant class of endogenous, small non-coding RNAs, 18–25 nucleotides in length, which regulates protein synthesis at the post-transcriptional level. MicroRNAs are highly conserved in sequence between distantly related organisms, indicating their participation in essential biological processes (Carrington and Ambros, 2003). Abnormal expression of cancer-related miRNAs is characterised by increased or decreased expression levels compared with their levels in the corresponding normal tissue. The miRNA-21 (miR-21) is consistently upregulated in many types of cancers including cancer of the colon (Slaby et al, 2007; Schetter et al, 2008), breast (Yan et al, 2008; Qian et al, 2009), lung (Markou et al, 2008), stomach (Chan et al, 2008) and glioblastoma (Gabriely et al, 2008). Among the reported mRNA targets of miR-21 are PTEN, PDCD4, Spry-1 and NF1B, suggesting that miR-21 is involved in regulation of apoptosis, proliferation and migration (Meng et al, 2007; Asangani et al, 2008; Gabriely et al, 2008; Yao et al, 2011). Additionally, miR-21 levels seem to increase with increasing stage of the tumour in, for example, colon and breast cancer, suggesting an important role of miR-21 in cancer invasion and dissemination (Slaby et al, 2007; Yan et al, 2008; Qian et al, 2009). These data taken together strongly suggest miR-21 as a potential prognostic marker in early-stage cancer such as stage II colon cancer. Studies have found high levels of miR-21 in colorectal cancer patients to be an indicator of poor prognosis, but so far none have been population based (Slaby et al, 2007; Schetter et al, 2008; Nielsen et al, 2011).
Most studies quantifying miRNAs for identification of differential expression have been based on microarrays (Lim et al, 2005), real-time PCR (RT-PCR) (Bandres et al, 2006) and deep sequencing (Ferdin et al, 2010). These quantitative miRNA expression analysis platforms are strong quantitative tools with a high level of precision and reproducibility and have been used to identify valuable biomarker candidates. However, important clinical information may be lost when focal miRNA expression is masked by non-cancerous tissue present in the samples, such as normal mucosa, submucosa and muscularis externa, mucous and necrotic tissue (Bandres et al, 2006). Additionally, RNA extraction from formalin-fixed paraffin-embedded (FFPE) tissue blocks is both time-consuming and suboptimal. Current pathological practice is based on FFPE tissue blocks, and the vast majority of archival material is preserved as such. Therefore, new methods should be considered. Recently, it has been reported that in situ hybridisation (ISH) using locked nucleic acid (LNA) modified DNA probes, raise the potential of evaluating tissue morphology and to quantitatively assess the miR-21 signal (Nielsen et al, 2011; Rask et al, 2011). The study by Nielsen et al also addressed the prognostic information of miR-21 expression and found that high miR-21 level was associated with poor disease-free survival. However, the patient material was limited (Nielsen et al, 2011).
The aim of the present study was to further investigate the prognostic importance of miR-21, quantified by ISH, in a unique, large, homogeneous, population-based cohort consisting of all patients with stage II colon cancer diagnosed and treated exclusively by surgical resection in Denmark in the year 2003.
Patients and methods
Patients
The study population was retrieved by a search in the nationwide registry administered by the Danish Colorectal Cancer Group (DCCG). This database contains prospectively collected surgical and pathological data. The search identified all surgically treated patients diagnosed with stage II colon cancer in 2003 (N=764). Patients dying within 30 days from their operation were excluded (N=66). All but two hospitals participated in the study and hence patients from those hospitals were not included (N=56), thus creating a highly representative cohort (93%) of the Danish population of stage II colon cancer patients in 2003. Furthermore, there were the following exclusions: tumour samples missing in archives (N=23); patients being categorised wrongly as stage II colon cancer (N=14); patients receiving adjuvant chemotherapy (N=16); lack of sufficient tissue for analysis (N=7); analysis exclusion criteria regarding number of images acquired <8 (N=41) and TR values <20 000 (N=21), see below. Thus, 520 patients were included in the statistical analysis. The study was approved by the Regional Scientific Ethical Committee of Southern Denmark according to Danish law. Postoperatively, patients were followed by the treating departments according to local guidelines. The patients were not routinely referred to a Department of Oncology. Thus, the majority of data on recurrence and death were obtained through Danish registries linked to the Danish social security number given to every Danish citizen at birth and to all ethnic immigrants.
The national registry holding all pathology reports in Denmark was used to identify patients with pathologically verified recurrence. Patients experiencing other malignancies were also identified using this registry and subsequently censored from survival analysis on the date of their new cancer diagnosis. To identify patients who had been in contact with the Department of Oncology or who had died, the national registry recording status on all Danish citizens as to their contact to the healthcare system and date of death was used. Patients with non-pathologically verified recurrence and patients receiving adjuvant chemotherapy were found by evaluating patient charts in the Departments of Oncology. A search in the ‘Cause of Death Registry’ identified patients registered with colon cancer as the cause of death. Follow-up was closed at 1 January 2010. From the study population of 520 patients, we identified the following: 206 patients had died and 73 patients had experienced disease recurrence. According to the registries, 90 patients had died from colon cancer, only 53 of these patients were also identified as having disease recurrence and in the analysis of recurrence-free cancer-specific survival (RF-CSS) events on the remaining 20 patients were added giving 110 events. The date registered was the first coming event of either disease recurrence or death from colon cancer. We also identified 16 patients who had received adjuvant chemotherapy and 23 patients who had been diagnosed with another cancer.
Pathology
One FFPE tissue block representing the invasive front of the tumour of each patient was collected from the Departments of Pathology in Denmark. Information on T-category, malignancy grade, nerve- and vascular-invasion, and the number of lymph nodes assessed was obtained from the pathology reports. Patients were scored as ‘not assessed’ if the pathological feature was not described. Data on localisation, tumour perforation, and tumour fixation was obtained from the DCCG registry and based on the surgeons’ reports.
In situ hybridisation
In situ hybridisation was performed essentially as described previously (Nielsen et al, 2011). In brief, the single 6-μm section from each tumour was processed in a Tecan Evo (Männedorf, Switzerland) automated ISH instrument. Predigestion with proteinase-K (15 μg ml−1) was performed at 37°C for 8 min. After pre-hybridisation for 15 min in hybridisation buffer (Exiqon, Vedbaek, Denmark), double-digoxigenin labelled 22’mer LNA probe specific for full-length miR-21 (Exiqon) was incubated at 30 nM for 1 h at 59°C. SSC stringent washes were performed at 59°C. Probe was detected with alkaline phosphatase-conjugated Fab fragments diluted 1 : 800 (Roche, Mannheim, Germany), followed by 1 h incubation with NBT-BCIP substrate (Roche). Sections were dehydrated and mounted using Eukitt (VWR, Herlev, Denmark). All reagents, including the proteinase-K, the DIG-labelled probe and the anti-DIG antibody were from the same batch and prepared identically each day. All steps in the Tecan were controlled regarding volumes, temperature and time.
Image analysis
Quantification of relative expression levels was obtained essentially as described earlier (Nielsen, 2012). In brief, the tumour area was identified on overview images and digitally selected as a region of interest. The areas containing normal mucosa and submucosa and ulcerating areas were not included. Within the selected area, 25 random images were collected per slide using a × 20 objective. Exposure of sample images was strictly controlled and locked at 6.993 ms with RGB (red–green–blue) values at 170–180 in non-stained blank areas. Sample images with staining artifacts were discarded, as were also images with <10% cancer cells in the image field. Thus, all images contained both cancer cells and stromal cells. A Bayesian pixel classifier to discriminate blue (B, ISH signal), red (R, nuclear counter stain), purple (P, blue ISH signal overlaying nuclear stain) and tissue background was designed based on three images from three different tumours that represented variations in blue and red colour. The following parameters were obtained for each sample image; B, R, P, total blue (TB=B+P), total red (TR=R+P) and TBR=TB/TR.
Series of 50 slides were analysed and included two control slides in each series to obtain a precision estimate of the measurements. The series also included replicates of adjacent sections obtained from three tumours (CV<49%). The variation of TBR between individuals was 215%, indicating that the precision of the measurements was sufficiently high to justify statistical analyses (25).
A test run, using four sections from each of 12 tumours was performed to adjust the probe concentration and the hybridisation temperature for optimal signal intensity.
Statistical analysis
Overall survival was defined as time from surgery until death from any cause. Recurrence-free cancer-specific survival (RF-CSS) was defined as the time from surgery until documented tumour recurrence or death from colon cancer, death from other causes was censored and also patients diagnosed with other malignancies were censored from the date of their new cancer diagnosis. Survival was estimated according to the Kaplan–Meier method, and the log-rank test was used to test for differences among groups. The Cox regression model was used to adjust for known prognostic factors; Gender, age, T-category, malignancy grade, localisation, perforation, fixation and number of lymph nodes (dichotomized into above and under 12). The proportional hazard assumption was tested for all variables used in the Cox model, using Schoenfeld residuals. All statistical calculations were carried out using the STATA 11.0 (StataCorp LP, College Station, TX, USA), and all statistical tests were two-sided with a significance level of 0.05.
By visual inspection of the relevant qq-plots, the log-transformed miR-21 values (TB and TBR) followed normal distributions.
Results
Patient characteristics
Patient characteristics are presented in Table 1. The majority of the patients were female patients with a medium differentiated T3 tumour. Location of the tumours was evenly distributed between left (left flexure, descendent, sigmoid) and right colon (coecum, ascendant, right flexure, transverse). Owing to the low number and uncertainty of the low malignancy grade classification, tumours of low and medium malignancy were pooled together in the survival analysis. No significant associations were found between miR-21 expression and patient characteristics.
Localisation of miR-21 ISH signal
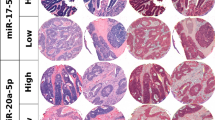
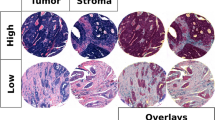
The miR-21 ISH signal intensity and prevalence varied considerably within the tumours and between patients, and it was predominantly seen in fibroblastic stromal cells (Figure 1C). We found that miR-21 was predominantly expressed in fibroblast-like cells in the stromal compartment of the tumour. In a smaller fraction of the samples (10–20%) some miR-21-positive cancer cells were also seen (Figure 1F), and in these cases only sub-populations of cancer cells were miR-21 positive. The miR-21-positive cancer cells also included budding cancer cells. The intensity varied from patient to patient and locally within the tumour slide. The miR-21 expression pattern was characterised by intense expression in the tumour area in contrast to the normal mucosa, where weakly stained mononuclear cells were observed.

Localisation and image analysis of miR-21 in situ hybridisation signal in colon cancer. Paraffin sections from two representative colon cancers (A–C and D–F) stained for miR-21 using LNA-based in situ hybridisation. The images, A and D, are selected random images obtained with a × 20 objective. A selected area in A and D has been enlarged in B and E, and is presented after colour segmentation in C and F. The miR-21 in situ hybridisation signal (blue, examples indicated by arrows in B and C) is seen in tumour-associated stromal fibroblast-like cells (B, arrows) in virtually all colon tumours, whereas miR-21 signal in cancer cells (E, arrows) was less frequently seen. For quantitation of the in situ hybridisation signal, the blue and purple stain in A/B and D/E are translated into green and yellow pixels in C and F. The nuclear red counterstain is likewise translated into red and the tissue background into black in C and F. Bars are 50 μm.
Quantification of miR-21 ISH signal
To quantify the ISH signal in the tissue sections, systematic random non-overlapping image fields were compiled from each tumour section. A mean of 16 image fields (range: 8–26) were compiled from each tumour. If the number of image fields was less than eight for one tumour section, the patient was excluded from the statistical analyses. All image fields that passed the inclusion criteria (see Patients and Methods) were processed with a pixel classifier that discriminated the blue ISH signal (B), the red nuclear stain (R), the blue signal located over red nuclear stain (P) and all other tissue structures (see Figures 1C and F). Total blue area (TB=B+P), total red area (TR=R+P) and total blue area per total red area (TBR=TB/TR) were obtained of which the TB and TBR values represent estimates of miR-21 expression, and TR the overall nuclear density. Sections cut too thin, samples fixed inadequately and tumours with poor cell density (prevalent in mucinous lesions) generally had low TR, and cases with TR <20 000 μm2 were excluded, see patients paragraph. As expected, substantial variation of both TB and TBR was observed; TB range=23.61–185 274 μm2; TBR range=0.0001814–13.085, as illustrated in Figure 2 where patients were divided into tertiles according to their mean log(TBR) value.

Box-plot of miR-21 expression levels in patients divided into tertiles of log(TBR). Substantial variation of both TB and TBR was observed; TB range=23.61–185 274 μm2; TBR range=0.0001814–13.085.
The prognostic value of miR-21
Results from the log-rank analysis of mean log(TBR) are listed in Table 2. Patients expressing high levels of miR-21 (high mean log(TBR)) had significantly inferior RF-CSS (HR=1.26; 95% CI: 1.15–1.60; P<0.001), and the same applied to mean log(TB) (HR=1.12; 95% CI: 1.0–1.42; P=0.05). Proportional hazard assumptions were tested for all variables. Results from the multiple Cox regression are outlined in Table 3 and included age, gender, T-category, malignancy grade, localisation, tumour perforation, tumour fixation and number of lymph nodes. Mean log(TBR) was found to be an independent predictive marker of poor RF-CSS (HR=1.41; 95% CI: 1.19–1.67; P<0.001), and the same applied to high levels of mean log(TB) (P=0.018). In addition to mean log(TBR), the following parameters were found to be predictive of a poor outcome regarding RF-CSS in the Cox regression analysis: male gender (P=0.033), T4-category (P<0.001), and tumour perforation (P<0.001). In the Cox regression analysis of OS, the following parameters were found to be prognostic of a poorer outcome; increasing age (P<0.001), male gender (P<0.001) and T4-category (P=0.017). We did not find any significant relation between miR-21 expression and OS.
Vascular and nerve invasion were not described in a large fraction of the patients (22.7% and 24.2%, respectively). Thus, the Cox regression analysis was only performed with respect to these two pathological features in the limited subsets of patients. However, high levels of mean log(TBR) was consistently found to be significantly related to poor RF-CSS (HR=1.52; 95% CI: 1.23–1.88; P<0.001). The same applied to log(TB) (P=0.008).
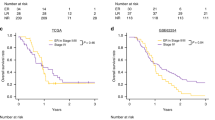
To illustrate the effect of increasing mean log(TBR), the population cohort was stratified into tertiles according to their mean log(TBR) value. As illustrated in Figure 3, patients with mean log(TBR) values in the upper tertile had significantly shorter RF-CSS (HR=1.92; 95% CI: 1.19–3.09; P=0.008) compared with patients with mean log(TBR) values in the lower tertile.

Kaplan–Meier plot illustrating recurrence-free cancer-specific survival (RF-CSS) of the patients divided into tertiles of log(TBR). Patients with mean log(TBR) values in the upper tertile had significantly shorter RF-CSS (HR=1.92; 95% CI: 1.19–3.09; P=0.008) compared with patients with mean log(TBR) values in the lower tertile.
Discussion
At present, the decision on adjuvant chemotherapy for stage II colon cancer patients is based on clinical and pathological markers of risk, which are inadequately informative in most of the patients, and better methods are certainly needed (Tournigand and de Gramont, 2011). For several years, new prognostic markers of significant importance have been a central topic in cancer research with the perspective of individualised treatment.
Most studies have been retrospective and included small numbers of highly selected patients. The risk of such studies being false positive is very high, and it has become evident that most biomarker studies have failed verification in new independent patient series (Locker et al, 2006). However, the present study included nearly all stage II patients in a population of 5 million people and can thus be considered unbiased with regard to selection.
The present study shows that increasing mean log(TB) (representing the relative miR-21 expression level) and mean log(TBR) (representing values normalised to the nuclear density) are significantly related to decreasing RF-CSS. These results thus confirm the prognostic importance of miR-21 independently from prognostic markers, proven to be inadequate, for example, T-category, malignancy grade, tumour perforation, tumour fixation, invasion of nerves and invasion of veins. Our results are in agreement with the previous study by Nielsen et al (2011) reporting that high miR-21 levels determined by ISH in 130 cases of stage II colon cancer is correlated with poor disease-free survival. The findings were based on a sample cohort as part of the RANX study and contained patient samples collected from 1991 to 1993 (Nielsen et al, 2011). They also found a significant impact on OS. In contrast, we found no prognostic value of miR-21 in analyses of OS. At the cut-off point set to 1 January 2010, 116 patients had died from other causes than colon cancer, whereas 110 patients had experienced relapse or had died from colon cancer. This indicates that at least half of stage II colon cancer patients die from causes other than colon cancer. Hence, OS analyses will be diluted, calling for endpoint analyses focusing on recurrence of the disease.
Our results are also in keeping with previous studies using PCR to quantify miR-21 in CRC tissue. Schetter et al (2008) studied the profile of the miRNA expression in paired tumour and normal tissue samples from 84 patients with colon cancer (29 stage II patients) as a training set and paired samples from another 113 patients with colon cancer (37 stage II patients) as a validation set. Among the 37 miRNAs that were differentially expressed, miR-21 was selected for validation. They found that high expression of miR-21 was significantly associated with poor prognosis, independent of T-category, age, sex and tumour location (Schetter et al, 2008). Slaby et al (2007) also reported that miR-21 upregulation in CRC patients was associated with lymph node positivity and development of distant metastasis based on their study of 29 patients.
In this study, the majority of tumours expressed the miR-21 ISH signal in fibroblast-like stromal cells. However, miR-21-positive cancer cells were also found in a small fraction of the tumours. Previous studies using identical probes to visualise miR-21 report the same distribution (Nielsen et al, 2011; Rask et al, 2011), while other groups using different probes describe miR-21-positive tumour cells in the majority of the tumours (Schetter et al, 2008; Yamamichi et al, 2009). The reason for the discrepancies could be explained by cross-reaction of the probe to ‘similar sequences’ allowed under suboptimal hybridisation conditions as well as different reagents employed to detect the labelled probe. However, it can not be excluded that a different probe could influence the results. It is noteworthy that miR-21 demonstrates prognostic impact despite the fact that it is found in the stroma cells and not in the tumour cells. Explanations are speculative but it can not be excluded that signals from stroma to the tumour cells, including paracrine signalling, influence the behaviour of the tumour.
Because of the exclusion criterion that each slide should be evaluated by at least eight images, 41 patients were excluded. This is most likely explained by the fact that we collected the tumour block representing the invasive front from each patient. Therefore, some of the blocks had small tumour content and as the software did not allow image fields to overlap, fewer images were available for analysis.
Using image quantified ISH we were able to assess miR-21 on archival FFPE tissue in this unique population. The results showed that increasing mean log(TBR) is an independent prognostic marker of poor RF-CSS in a stage II colon cancer population consisting of nearly all patients diagnosed with this disease in Denmark in the year 2003. Our findings strongly suggest that miR-21 measured by ISH is a robust and valuable indicator of adverse prognosis in stage II colon cancer. The results call for evaluation together with other variables to generate a fully specified prognostic index, pointing out the individuals, in this group of patients, in need of adjuvant chemotherapy. Eventually, such an index should be tested in a prospective, randomised trial setting for conclusive evaluation of the clinical impact.
Change history
10 September 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Asangani IA, Rasheed SA, Nikolova DA, Leupold JH, Colburn NH, Post S, Allgayer H (2008) MicroRNA-21 (miR-21) post-transcriptionally downregulates tumor suppressor Pdcd4 and stimulates invasion, intravasation and metastasis in colorectal cancer. Oncogene 27: 2128–2136
Bandres E, Cubedo E, Agirre X, Malumbres R, Zarate R, Ramirez N, Abajo A, Navarro A, Moreno I, Monzo M, Garcia-Foncillas J (2006) Identification by Real-time PCR of 13 mature microRNAs differentially expressed in colorectal cancer and non-tumoral tissues. Mol Cancer 5: 29
Bastos DA, Ribeiro SC, de FD, Hoff PM (2010) Combination therapy in high-risk stage II or stage III colon cancer: current practice and future prospects. Ther Adv Med Oncol 2: 261–272
Benson AB, Schrag D, Somerfield MR, Cohen AM, Figueredo AT, Flynn PJ, Krzyzanowska MK, Maroun J, McAllister P, Van CE, Brouwers M, Charette M, Haller DG (2004) American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol 22: 3408–3419
Carrington JC, Ambros V (2003) Role of microRNAs in plant and animal development. Science 301: 336–338
Chan SH, Wu CW, Li AF, Chi CW, Lin WC (2008) MiR-21 microRNA expression in human gastric carcinomas and its clinical association. Anticancer Res 28: 907–911
Ferdin J, Kunej T, Calin GA (2010) Non-coding RNAs: identification of cancer-associated microRNAs by gene profiling. Technol Cancer Res Treat 9: 123–138
Figueredo A, Coombes ME, Mukherjee S (2008) Adjuvant therapy for completely resected stage II colon cancer. Cochrane Database Syst Rev 3:, CD005390
Gabriely G, Wurdinger T, Kesari S, Esau CC, Burchard J, Linsley PS, Krichevsky AM (2008) MicroRNA 21 promotes glioma invasion by targeting matrix metalloproteinase regulators. Mol Cell Biol 28: 5369–5380
Gangadhar T, Schilsky RL (2010) Molecular markers to individualize adjuvant therapy for colon cancer. Nat Rev Clin Oncol 7: 318–325
Gross CP, Andersen MS, Krumholz HM, McAvay GJ, Proctor D, Tinetti ME (2006) Relation between Medicare screening reimbursement and stage at diagnosis for older patients with colon cancer. JAMA 296: 2815–2822
Kopetz S, Freitas D, Calabrich AF, Hoff PM (2008) Adjuvant chemotherapy for stage II colon cancer. Oncology (Williston Park) 22: 260–270
Lim LP, Lau NC, Garrett-Engele P, Grimson A, Schelter JM, Castle J, Bartel DP, Linsley PS, Johnson JM (2005) Microarray analysis shows that some microRNAs downregulate large numbers of target mRNAs. Nature 433: 769–773
Locker GY, Hamilton S, Harris J, Jessup JM, Kemeny N, Macdonald JS, Somerfield MR, Hayes DF, Bast RC (2006) ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol 24: 5313–5327
Lombardi L, Morelli F, Cinieri S, Santini D, Silvestris N, Fazio N, Orlando L, Tonini G, Colucci G, Maiello E (2010) Adjuvant colon cancer chemotherapy: where we are and where we'll go. Cancer Treat Rev 36 (Suppl 3): S34–S41
Markou A, Tsaroucha EG, Kaklamanis L, Fotinou M, Georgoulias V, Lianidou ES (2008) Prognostic value of mature microRNA-21 and microRNA-205 overexpression in non-small cell lung cancer by quantitative real-time RT-PCR. Clin Chem 54: 1696–1704
Meng F, Henson R, Wehbe-Janek H, Ghoshal K, Jacob ST, Patel T (2007) MicroRNA-21 regulates expression of the PTEN tumor suppressor gene in human hepatocellular cancer. Gastroenterology 133: 647–658
Nielsen BS (2012) MicroRNA in situ hybridization. Methods Mol Biol 822: 67–84
Nielsen BS, Jorgensen S, Fog JU, Sokilde R, Christensen IJ, Hansen U, Brunner N, Baker A, Moller S, Nielsen HJ (2011) High levels of microRNA-21 in the stroma of colorectal cancers predict short disease-free survival in stage II colon cancer patients. Clin Exp Metastasis 28: 27–38
O’Connell MJ (2004) Current status of adjuvant therapy for colorectal cancer. Oncology (Williston Park) 18: 751–755
O’Connor ES, Greenblatt DY, Loconte NK, Gangnon RE, Liou JI, Heise CP, Smith MA (2011) Adjuvant chemotherapy for stage ii colon cancer with poor prognostic features. J Clin Oncol 29 (25): 3381–3388
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55: 74–108
Qian B, Katsaros D, Lu L, Preti M, Durando A, Arisio R, Mu L, Yu H (2009) High miR-21 expression in breast cancer associated with poor disease-free survival in early stage disease and high TGF-beta1. Breast Cancer Res Treat 117: 131–140
Rask L, Balslev E, Jorgensen S, Eriksen J, Flyger H, Moller S, Hogdall E, Litman T, Nielsen BS (2011) High expression of miR-21 in tumor stroma correlates with increased cancer cell proliferation in human breast cancer. APMIS 119: 663–673
Schetter AJ, Leung SY, Sohn JJ, Zanetti KA, Bowman ED, Yanaihara N, Yuen ST, Chan TL, Kwong DL, Au GK, Liu CG, Calin GA, Croce CM, Harris CC (2008) MicroRNA expression profiles associated with prognosis and therapeutic outcome in colon adenocarcinoma. JAMA 299: 425–436
Slaby O, Svoboda M, Fabian P, Smerdova T, Knoflickova D, Bednarikova M, Nenutil R, Vyzula R (2007) Altered expression of miR-21, miR-31, miR-143 and miR-145 is related to clinicopathologic features of colorectal cancer. Oncology 72: 397–402
Tournigand C, de Gramont A (2011) Chemotherapy: is adjuvant chemotherapy an option for stage II colon cancer? Nat Rev Clin Oncol 8: 574–576
Yamamichi N, Shimomura R, Inada K, Sakurai K, Haraguchi T, Ozaki Y, Fujita S, Mizutani T, Furukawa C, Fujishiro M, Ichinose M, Shiogama K, Tsutsumi Y, Omata M, Iba H (2009) Locked nucleic acid in situ hybridization analysis of miR-21 expression during colorectal cancer development. Clin Cancer Res 15: 4009–4016
Yan LX, Huang XF, Shao Q, Huang MY, Deng L, Wu QL, Zeng YX, Shao JY (2008) MicroRNA miR-21 overexpression in human breast cancer is associated with advanced clinical stage, lymph node metastasis and patient poor prognosis. RNA 14: 2348–2360
Yao Q, Cao S, Li C, Mengesha A, Kong B, Wei M (2011) Micro-RNA-21 regulates TGF-beta-induced myofibroblast differentiation by targeting PDCD4 in tumor-stroma interaction. Int J Cancer 128: 1783–1792
Acknowledgements
We are thankful for the initial work on the database conducted by the DCCG and for the help on the search in this database. We are also thankful for the technical assistance provided by Birgit Roed Sørensen and proof reading by Karin Larsen.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
SJ and BSN held a full-time employment at the time of analysis for an entity (name of entity: Exiqon A/S) having a commercial interest in the subject matter under consideration in the manuscript. The remaining authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Kjaer-Frifeldt, S., Hansen, T., Nielsen, B. et al. The prognostic importance of miR-21 in stage II colon cancer: a population-based study. Br J Cancer 107, 1169–1174 (2012). https://doi.org/10.1038/bjc.2012.365
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2012.365
Keywords
This article is cited by
-
Novel insights on perils and promises of miRNA in understanding colon cancer metastasis and progression
Medical Oncology (2023)
-
Prognostic Value of MicroRNAs in Stage II Colorectal Cancer Patients: A Systematic Review and Meta-Analysis
Molecular Diagnosis & Therapy (2020)
-
Circulating inflammation signature predicts overall survival and relapse-free survival in metastatic colorectal cancer
British Journal of Cancer (2019)
-
Overexpression of miR-21-5p promotes proliferation and invasion of colon adenocarcinoma cells through targeting CHL1
Molecular Medicine (2018)
-
Effect of dietary components on miRNA and colorectal carcinogenesis
Cancer Cell International (2018)
