
Abstract
Background:
Clear cell renal cancer frequently harbours von Hippel–Lindau (VHL) gene mutations, leading to stabilisation of the hypoxia-inducible factors (HIFs) and expression of their target genes. We investigated HIF-1 and HIF-2 in the regulation of microRNA-210 (miR-210), and its clinical relevance in renal tumours.
Methods:
RCC4 and 786-O renal cancer cell lines transfected with either an empty vector or functional VHL and incubated in normoxia or hypoxia were examined for miR-210 expression. Hypoxia-inducible factor siRNAs were used to examine their regulation of miR-210. Seventy-one clear cell renal tumours were sequenced for VHL mutations. Expression of miR-210, VHL, CA9, ISCU and Ki-67 were determined by immunohistochemistry and qRT–PCR.
Results:
In addition to HIF-1 regulating miR-210 in renal cancer, HIF-2 can regulate this microRNA in the absence of HIF-1. MicroRNA-210 is upregulated in renal cancer compared with normal renal cortex tissue. MicroRNA-210 correlates negatively with its gene target ISCU at the protein and mRNA level. MicroRNA-210 correlated with positive outcome variables and negatively with Ki-67.
Conclusion:
We provide further evidence of miR-210 activity in vivo, and show that high miR-210 expression is associated with better clinico-pathological prognostic factors.
Similar content being viewed by others


Main
MicroRNAs (miRNAs) are non-coding oligonucleotides, which bind to complementary sites on target genes, leading to translational inhibition or mRNA degradation (Pillai, 2005). MicroRNA-210 (miR-210) is the most ubiquitously upregulated miRNA in multiple cancer cell lines in hypoxia (Camps et al, 2008; Gee et al, 2010; Ho et al, 2010; McCormick et al, 2010). It is upregulated in many tumour types, presumably because of the inherently hypoxic nature of many expanding tumours, as disordered angiogenesis does not maintain adequate blood supply to the lesions (Kulshreshtha et al, 2007). Tumour hypoxia has been shown to correlate with poorer response to radiotherapy and chemotherapy, and poor outcome regardless of modality. Our group and others have shown miR-210 to correlate with poorer prognosis in breast and head and neck cancer (Camps et al, 2008; Gee et al, 2010).
Renal cancer is the third most common urological malignancy, and represents 5% of cancer diagnoses. Clear cell renal cell cancer (CCRCC) is the most common histological subtype, which is characterised by mutations of the von Hippel–Lindau (VHL) gene in 75% of tumours. The VHL gene is responsible for degrading the hypoxia-inducible factor (HIF) transcription factors. In normoxia, HIF-α molecules are hydroxylated, leading to binding to VHL, ubiquitination, and proteasomal degradation. In hypoxia, lack of HIF-α hydroxylation leads to stabilisation of the molecules, which are able to bind to HIF-β (also known as the aryl hydrocarbon nuclear translocator), translocate to the nucleus, and mediate gene transcription. Inactivating mutations of the VHL gene lead to constitutive stabilisation of the HIF-α molecules, and overexpression of the HIF target genes involved in processes such as angiogenesis, the shift to glycolysis, invasion, metastasis and proliferation. Hypoxia-inducible factor exists in two major isoforms – HIF-1α and HIF-2α (referred to henceforth as HIF-1 and HIF-2, respectively), which lead to transcription of overlapping but distinct sets of gene targets (Harris, 2002).
We, and others, have shown that miR-210 targets ISCU (iron sulphur cluster homologue), which acts as a scaffold protein for the formation of iron sulphur (Fe–S) clusters (Chan et al, 2009; Chen et al, 2010; Favaro et al, 2010). Fe–S clusters function as electron transporters and are key components of complexes I and II of the mitochondrial electron transport chain, and also of TCA cycle enzymes (Rouault and Tong, 2008). We showed that miR-210 knockdown of ISCU led to reduction in complex I and aconitase activity, leading to an increase in the lactate:pyruvate ratio and an increase in reactive oxygen species production (Favaro et al, 2010). Thus, some of the phenotypes of HIF induction may be regulated by the miR-210 response.
We therefore investigated the regulation of miR-210 in renal cancer cell lines, and showed that both HIF-1 and HIF-2 can contribute to its overexpression. We assessed whether in primary tumours there was reciprocal regulation of ISCU expression with miR-210, which would support the in vitro studies. Finally, we demonstrated that miR-210 expression correlates with clinico-pathological data corresponding to better prognosis, in contrast to other cancer types, potentially reflecting the more potent effect of HIF-1 than HIF-2.
MATERIALS AND METHODS
Cell lines
RCC4 and 786-O cell lines were a generous gift from Dr William G Kaelin, Farber Institute. They had previously been transfected with either an empty vector control or a vector containing the functional wild-type VHL gene (Iliopoulos et al, 1995). They have been authenticated through determination of HIF-1 and HIF-2 expression status by western blotting. Papillary and CCRCC renal tumours, and matched normal renal cortex from patients who underwent nephrectomy, were obtained from the Oxford Radcliffe Biobank. RNA and DNA were extracted from the tumours in parallel. Tumours were homogenised using FastPrep Lysing System Matrix D (MP Biomedicals, Solon, OH, USA), and then lysed in Trizol Reagent (Invitrogen, Paisley, UK). Extraction of RNA and DNA was carried out as per the manufacturer’s protocol. RNA from 30 tumours was also obtained from the Leeds biobank (Young et al, 2009). Ethical approval for use of clinical samples has been obtained from the local research ethics committee, reference 09/H0606/5.
Tissue microarray
A tissue microarray (TMA) containing 40 CCRCCs was constructed, containing three replicate cores of each tumour. Immunohistochemistry was carried out with antibodies to ISCU (Novus Biologicals, Cambridge, UK), CA9 (murine M75 monoclonal antibody (Saarnio et al, 1998)) and VHL (BD Biosciences, Oxford, UK). Staining was scored using the percentage-intensity method (Chia et al, 2001).
qRT–PCR
MicroRNA-210 analysis was carried out by qRT–PCR using TaqMan reagents (Applied Biosystems, Austin, TX, USA). MicroRNA-210 was normalised to the average expression of three small-nucleolar RNA control genes: RNU44, RNU48 and RNU6B. qRT–PCR for CA9 and VHL were carried out using the Roche probe system (Roche, Burgess Hill, UK), using SensiMix PCR mastermix (Bioline, London, UK). Data were normalised to beta-actin expression. The VHL primers left: 5′-ATCCGTAGCGGTTGGTGAC-3′, right: 5′-CTCACGGATGCCTCAGTCTT-3′. CA9 primers left: 5′-CTTGGAAGAAATCGCTGAGG-3′, right: 5′-TGGAAGTAGCGGCTGAAGTC-3′. Statistical analysis of the data from tumour samples was normally performed with non-parametric Mann–Whitney tests because of the increased variability of data in the tumour samples.
Western blotting
Cells were lysed with 8 M urea lysis buffer, and run on 12% SDS–PAGE gels. They were probed with antibodies for ACTB (Sigma-Aldrich, St Louis, MO, USA), HIF-1α (BD Biosciences) and HIF-2α (Abcam, Cambridge, UK).
Results
MicroRNA-210 is upregulated in renal cancer cell lines
RCC4 and 786-O renal cancer cell lines were selected for analysis of miR-210 expression. Both harbour an inactivating mutation of VHL, with constitutive HIF overexpression. 786-O cells lack functional HIF-1, whereas RCC4 cells express both HIF-1 and -2. Both cell lines had been transfected with either an empty vector (referred to as ‘VHL−’) or a vector containing functional VHL (referred to as ‘VHL+’) (Iliopoulos et al, 1995). RCC4 cells were incubated in normoxia or 0.1% O2 for 24 h, and expression of HIF-1 and HIF-2 protein was determined by western blotting. As expected, the RCC4 VHL+ cells demonstrated expression of HIF-1 and -2 in hypoxia alone, whereas the VHL− cells constitutively overexpressed HIF in normoxia with further increased expression in hypoxia (Figure 1A).

The hypoxic regulation of miR-210 in RCC4 cells. (A) Hypoxia-inducible factor-1α and -2α expression in RCC4 cells. RCC4 cells were transfected with an empty vector (VHL−) or vector coding for functional VHL (VHL+) and cultured in normoxia or 0.1% O2 for 24 h. Protein was immunoblotted on SDS–PAGE gels. (B) MicroRNA-210 is upregulated six-fold in hypoxia in RCC4 VHL+ cells, and constitutively expressed in VHL− cells. (C) MicroRNA-210 is upregulated in 786-O cells expressing HIF-1-only. 786-O VHL+ and VHL− cells were cultured in normoxia or 0.1% O2 for 24 h. Hypoxic upregulation of 2.5-fold was observed in VHL+ cells. VHL− cells showed constitutive upregulation of miR-210 in normoxia, with further upregulation in hypoxia. The degree of overexpression was lower than in RCC4 cells. *P<0.05, **P<0.01, unpaired t-test.
786-O cells also demonstrated the expected hypoxia-induced expression of HIF-2 in the VHL+ cells, and constitutive expression in normoxia in the VHL− cells (Figure 2A). Hypoxia-inducible factor was not detected in this cell line. MicroRNA-210 expression was determined by qRT–PCR in both cell lines following culture in normoxia and 0.1% O2 for 24 h. RCC4 VHL+ cells demonstrated a six-fold induction of miR-210 in hypoxia (P<0.05, two-tailed t-test), whereas the VHL− cells constitutively overexpressed miR-210 approximately 15-fold in both normoxia and hypoxia (P<0.01, t-test) (Figure 1B). The 786-O VHL+ cells showed increased expression of miR-210 in hypoxia by 2.5-fold (P<0.05, t-test). The VHL− cells demonstrated constitutive overexpression of miR-210 in normoxia (P<0.05, t-test) (Figure 1C).

Hypoxia-inducible factor-2 mediates hypoxic miR-210 regulation in 786-O cells. (A) Validation of si-HIF-2α. 786-O VHL+ and VHL− cells were transfected with si-HIF-2α or a control molecule and incubated in normoxia or 0.1% O2 for 24 h. Hypoxia-inducible factor-2α was induced in hypoxia in the VHL+ cells, and constitutively expressed in the VHL− cells. Treatment with si-HIF-2α reduced expression to baseline. (B) MicroRNA-210 is regulated by HIF-2α in 786-O cells. 786-O cells were cultured as in the experiment in A. Hypoxic induction of miR-210 was almost completely reversed by si-HIF-2α in VHL+ cells. Constitutive overexpression of miR-210 in VHL− cells in normoxia was reduced to basal levels in VHL+ cells in normoxia. In hypoxia, si-HIF-2α only partially inhibited miR-210 expression. *P<0.05, **P<0.01, unpaired t-test.
Hypoxia-inducible factor-2 α regulates miR-210 in 786-O cells
MicroRNA-210 has been shown to be a HIF-1α target in many previous in vitro experiments (Huang et al, 2009). To explain miR-210 overexpression in 786-O VHL− cell lines, which do not express HIF-1α, we investigated HIF-2α as a potential regulator in this cell line.
786-O VHL+ and VHL− cells were incubated in normoxia or 0.1% O2 for 24 h, following transfection with either a scrambled control or siRNA to HIF-2 (si-HIF-2). The si-HIF-2 blocked the induction of HIF-2 in VHL+ cells in hypoxia, and reduced it to undetectable levels in the VHL− cell lines (Figure 2A). In the VHL+ cells, hypoxic miR-210 overexpression was inhibited by si-HIF-2. In the VHL− cells in normoxia, si-HIF-2 reduced miR-210 to baseline levels. In the VHL− cells in hypoxia, there was reduction in miR-210 expression by si-HIF-2, but not to baseline levels, and was not statistically significant (Figure 2B).
Further evidence for the ability of HIF-2 to substitute for HIF-1 in 786-O cells was provided through a pan-genomic analysis of HIF-2α and HIF-1β binding by chromatin immunoprecipitation coupled to high-throughput sequencing (CHIP-seq). This showed strong HIF-2 binding centred on a hypoxia response element (HRE, the core RCGTG motif recognised by HIF) contained within both a DNase-hypersensitivity cluster and a CpG island approximately 420 bp from the miR-210-coding region (Figure 3). Previous work by collaborators on MCF7 cells, which express both HIF-1 and -2, demonstrated that only HIF-1 knockdown inhibited the hypoxic induction of miR-210 (Camps et al, 2008). Nevertheless, as shown in Figure 3, the miR-210 locus in these cells has binding sites for both HIF-1 and HIF-2.

CHIP-seq data for HIF-binding sites. A combination of chromatin immunoprecipitation of the HIF isoforms and high-throughput sequencing was used. 786-O cells showed strong HIF-2 binding at a HRE motif near the miR-210-coding sequence. MCF7 cells, which express functional HIF-1 and -2, demonstrate binding of both isoforms at the HRE near the miR-210-coding sequence.
MicroRNA-210 is upregulated in renal cancer
Three types of renal tumour were obtained from our biobank, in Oxford, of snap-frozen nephrectomy specimens: CCRCCs, papillary renal tumours and benign oncocytomas, along with paired normal renal cortex controls. The tumours were collected between 2005 and 2008, with up to 5 years of follow-up. The clinical details of the patients are summarised in Table 1. Compared with normal tissue controls, miR-210 was overexpressed over 10-fold greater in the CCRCCs (N=32, P<0.001, Mann–Whitney test), 2.8-fold in the papillary tumours (N=9, P<0.05, Mann–Whitney test), and there was no change in the oncocytomas (N=4) (Figure 4A).

Expression of mir-210 in renal cancer. (A) MicroRNA-210 expression was measured by qPCR in renal tumours and normal controls. MicroRNA-210 was overexpressed 9-fold in CCRCCs (N=43), 2.7-fold in papillary tumours (N=9), and was not upregulated in oncocytomas (N=4). *P<0.05 and ***P<0.001, Mann–Whitney test. (B) MicroRNA-210 expression in normal and CCRCC tissue in tumours with, and without, VHL mutation. In tumours with VHL mutations, there was a 16-fold upregulation of miR-210 compared with normal control tissue (N=49), ****P<0.0001.
Forty-one CCRCC tumours were sequenced for VHL mutations. In all, 78% of the tumours initially sequenced had VHL mutations, with the majority (39%) occurring in exon 1.
RNA from a further 30 CCRCC tumours was obtained from the Leeds bank of frozen tissues, which had been characterised for loss of heterozygosity, promoter methylation and VHL mutations. These tumours were collected between 2000 and 2007, with up to 10 years of follow-up. All but one of the 30 tumours showed VHL inactivation by one of these processes (Young et al, 2009). Combining this with our set resulted in a total of 71 CCRCC tumours, in which miR-210 expression was analysed by qRT–PCR. The CCRCCs with (N=49), and without VHL gene mutations (N=22), both showed miR-210 overexpression of approximately 16-fold compared with normal controls (P<0.0001, Mann–Whitney test). However, there was no significant difference in expression of miR-210 between the CCRCCs with and without detected VHL mutations (Figure 4B).
MicroRNA-210 expression correlates with CA9 and VHL mRNA in renal tumours
The expression of CA9 in CCRCC tumours was measured by qRT–PCR (N=43). There was a significant but weak correlation of CA9 with miR-210 expression (R2=0.16, P<0.05, F-test) (Figure 5A). VHL mRNA was also measured by qRT–PCR, using primers designed to the 3′ UTR. There was a negative correlation of VHL mRNA expression with miR-210 (R2=0.2, P<0.01, F-test) (Figure 5B).

Correlation of CA9 and VHL mRNA expression with miR-210 in renal tumours. MicroRNA-210 correlates positively with CA9 expression and negatively with VHL expression. Expression of mRNA in 43 tumours was measured by qRT–PCR. (A) CA9 correlates with miR-210 expression. R2=0.16, P<0.05, F-test. (B) VHL correlates negatively with miR-210 expression. R2=0.2, P<0.01, F-test (Fisher’s linear regression).
MicroRNA-210 correlates inversely with ISCU expression in CCRCCs
It has been previously published by our group and others that ISCU is a miR-210 target (Chan et al, 2009; Chen et al, 2010; Favaro et al, 2010). We sought to determine whether miR-210 expression correlated with ISCU expression in clear cell renal tumours. ISCU mRNA expression was measured in 46 CCRCC tumours, along with matched normal controls. Normal renal tissue expressed 1.83-fold more ISCU mRNA compared with the tumours (N=23 in each group, P<0.0001, Mann–Whitney test) (Figure 6A). A TMA of 40 CCRCCs and 40 matched normal controls was stained for ISCU by immunohistochemistry and scored for cytoplasmic expression using a percentage-intensity score (PIS). The tumours expressed 40% less ISCU than the normal controls (P<0.001, Wilcoxon matched-pairs signed-rank test) (Figure 6B). The tumours were placed into two groups based on whether they expressed high (PIS score 4–12) or low (PIS 0–3) levels of ISCU. The analysis was performed in two groups as the PIS scoring does not return a continuous variable; the cut-offs selected for each PIS score range resulted in two equal-sized groups (N=20 each). MicroRNA-210 expression of the tumours in each group was plotted (Figure 6C). MicroRNA-210 expression was 2.7-fold higher in the low ISCU-scoring group, indicating a negative correlation of miR-210 with ISCU expression (P<0.001, Mann–Whitney test). The TMAs also contained eight papillary tumours. The CCRCCs displayed approximately half the ISCU expression of the papillary tumours (P<0.05, two-tailed t-test because of small sample size) (Figure 6D).

Correlation of ISCU and miR-210 expression in renal tumours. ISCU is downregulated in tumours. (A) ISCU mRNA was downregulated two-fold in the tumours compared with the normal renal cortex. ***P<0.001, Mann–Whitney test. (B) ISCU protein expression was measured by IHC in renal TMAs, using a PIS system. Tumours expressed 40% less ISCU than the normal cortex. ***P<0.001, Unpaired t-test. (C) Tumours were separated into two groups, expressing low (PIS 0–3, N=23) or high (PIS 4–12, N=25) levels of ISCU protein. MicroRNA-210 was expressed 2.7-fold higher in the low ISCU-expressing group. ***P<0.001, Mann–Whitney test. (D) The CCRCCs expressed half the ISCU protein of the papillary tumours. *P<0.05, unpaired t-test.
MicroRNA-210 expression correlates with favourable clinico-pathological factors
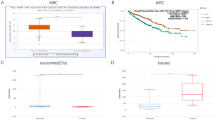
High miR-210 expression in CCRCCs was associated with lower stage and grade (Figure 7A and B). Higher grade (Fuhrman 3–4, N=49) tumours expressed 45% of the miR-210 compared with lower grade (Fuhrman 1–2, N=24) tumours (P<0.01, Mann–Whitney test) (Figure 7C). Similarly, higher-stage tumours (T3+, N=49) expressed 74% of the miR-210 compared with lower-stage (T1–2, N=24) tumours (P<0.05, Mann–Whitney test) (Figure 7D).

MicroRNA-210 correlation with pathological and outcome variables. MicroRNA-210 is associated with lower tumour grade (A) and stage (B). (C) Patients grouped by CCRCC tumours of high grade (grade 1–2, N=24) or low grade (grade 3–4, N=49). MicroRNA-210 expression in high-grade tumours was 55% of that in the low-grade tumours. **P<0.01, Mann–Whitney test. (D) MicroRNA-210 expression in high-stage (stage 3–4, N=49) tumours was 74% of that in low-stage (stage 1–2, N=24) tumours. *P<0.05. (E) Patients were separated into three (N=23 for each group) groups based on miR-210 expression in their CCRCC tumours. High miR-210 associated with better survival. P=0.05, Gehan–Breslow–Wilcoxon test. (F) Tumours were separated into two groups based on high (N=20) and low (N=18) Ki-67 expression. MicroRNA-210 expression was 1.7-fold lower in the Ki-76-low group (P<0.05, Mann–Whitney test).
Patients were divided into three equal-sized groups based on miR-210 expression levels (N=23 in each group). As shown in Figure 7E, high miR-210 expression was associated with improved survival post nephrectomy, compared with medium and low levels of miR-210 (P=0.05, log-rank test for trend; low miR-210 group: 12 deaths, 11 censored; medium miR-210 group: 8 deaths, 15 censored; high miR-210 group: 4 deaths, 19 censored). The analysis had also been performed based on two groups, but a significant survival difference was seen only in un-normalised miR-210 data (Figure 8). The three-group analysis demonstrated a larger difference in the miR-210-high group.

snoRNA controls and survival. (A–C) Survival of patients expressing snoRNA RNU44 (A), RNU48 (B) and RNU6B (C) genes >median or <median was plotted. No significant difference in survival was seen. (D) Patients expressing un-normalised miR-210 >median had improved survival post nephrectomy. P=0.005, log-rank test. Median survival miR-210 low 943 days, high 1959 days, HR 3.01, 95% CI 1.39–6.51.
In view of the above survival data, it was decided to examine tumour proliferation by analysing the expression of Ki-67, an established marker of proliferation. The TMAs were stained for Ki-67, and the tumours were separated into two groups based on high (N=19) or low (N=20) Ki-67 expression. MicroRNA-210 expression in the Ki-67-low tumours was 1.7-fold higher than in the Ki-67-high group (P<0.05, Mann–Whitney test) (Figure 7F).
Validation of control snoRNAs and mRNAs
Variation of RNU44, RNU48 and RNU6B with grade, stage and between normal tissue and tumour was plotted (Figure 9). No significant variation in average expression was seen between the two tissue types (normals CT=26.0, tumours CT=25.7). Average expression (CT value) of these controls did not vary greatly between high and low stage (CT=25.77 vs 25.71) or grade (CT=25.61 vs 25.99). The mRNA expression of the commonly used control beta actin (Seliger et al, 2007; Neal et al, 2010) did, however, vary more between normal (average CT=17.8) and tumour tissue (average CT=17.0) (Figure 10). Reassuringly, another control gene GUSB (which was not used for normalisation of VHL/CA9 in this study) demonstrates variation in the same direction with reduced expression in the normal tissues (average CT=23.3) compared with tumour tissues (average CT=22.2).

Expression of snoRNAs related to clinical features. Whiskers=minimum to maximum, box 25th–75th percentile. (A) Controls in low- or high-grade tumours. Average CT in low grade=25.61 and high grade=25.99. (B) Control genes in low- or high-stage tumours. Average CT across all three controls in low stage=25.71 and high stage=25.77. (C) Controls in normal or tumour tissue. Average CT in normals=26.0 and tumours=25.7.

Expression of control genes in normal and CCRCC tissue. Whiskers=minimum to maximum, box 25th–75th percentile. Beta-actin CT in normal vs tumour=17.80 vs 17.02 (mean) and 17.73 vs 16.72 (median). GUSB CT in normal vs tumour=23.3 vs 21.15 (mean) and 23.12 vs 20.87 (median).
Discussion
Hypoxia-inducible factor-1 and -2 are known to regulate distinct sets of genes (Raval et al, 2005; Gordan et al, 2007). Nevertheless, there is considerable overlap of the data sets, and the targets can vary among different tissue or cell types (Raval et al, 2005). Our group and others have previously shown miR-210 to be induced by HIF-1 in cell lines including RCC4, MCF7 and HUVEC (Camps et al, 2008; Pulkkinen et al, 2008). In this study, RCC4 VHL− cells upregulated miR-210 in the expected fashion, with the RCC4 VHL+ cells overexpressing miR-210-only in hypoxia. 786-O cells also upregulated miR-210, although to a lesser extent than the RCC4 cells expressing HIF-1. Knockdown of HIF-2 with siRNA blocked the hypoxic upregulation of miR-210 in VHL+ cells, and in the VHL− cells in normoxia. These findings are in contrast to Nakada et al (2011), who found that miR-210 was not upregulated in hypoxia, and concluded that HIF-1α was necessary for miR-210 induction. This may be explained by their use of 1% O2 compared with 0.1% O2 used in our study (Nakada et al, 2011). CHIP-seq data confirmed the presence of HIF-2 binding near the gene locus of miR-210, providing strong additional evidence of HIF-2-mediated regulation. However, hypoxia further increased miR-210 expression over the normoxic baseline in VHL− 786-O cells, and si-HIF-2 failed to prevent hypoxic miR-210 upregulation in the VHL− cells, suggesting that a HIF-independent mechanism is also promoting transcription of this miRNA. The fact that RCC4 cells upregulate miR-210 to a greater extent than 786-O cells suggests, although does not prove, that HIF-1 is the preferential regulator of miR-210. In support of this is the finding in MCF7 cells, which express both HIF isoforms, that only HIF-1 knockdown prevents miR-210 induction in hypoxia (Camps et al, 2008). Our CHIP-seq data in MCF7 cells confirm that both HIF-1 and HIF-2 bind close to the miR-210-coding region. Apparent dominance of HIF-1 in miR-210 regulation would be consistent with the findings of Elvidge et al (2006), who found that HIF-1 knockdown reduced general hypoxic upregulation of genes to a greater extent than HIF-2.
MicroRNA-210 has previously been reported to be upregulated in renal cancer (Juan et al, 2010; Weng et al, 2010; White et al, 2011), and has been described as part of a miRNA classification system for this disease (Fridman et al, 2010). We have confirmed miR-210 overexpression in both CCRCC and papillary renal cancers to a lesser extent, in agreement with the findings of Valera et al (2011). The CCRCCs induced higher levels of miR-210, presumably due to VHL dysfunction. We did not see a significant difference in expression of miR-210 between CCRCCs with VHL gene mutations and those without. This is most likely to be because of the presence of alternative mechanisms of VHL inactivation by methylation or loss of heterozygosity. Promotor hypermethylation of the VHL gene, even in the absence of VHL mutation, has been described, and could account for increased miR-210 in patients with tumours harbouring a normal VHL gene. In one study, hypermethylation of VHL was found in 5 out of 26 CCRCCs, 4 (15%) of which had no detectable VHL mutation (Herman et al, 1994). Thirty of our tumour samples (Leeds tumour data set) were analysed for all three mechanisms of VHL mutation, and 29 out of 30 tumours were found to have VHL inactivation by one of these means (Young et al, 2009).
There was a great range of miR-210 expression within the tumour samples, with much less variation in normal kidney tissue. The correlation of miR-210 with CA9 suggests that its expression could be due to HIF-1 transcriptional activity. CA9 is predominantly a HIF-1 target, and is not overexpressed in 786-O cells. Gordan et al (2008) categorised CCRCCs by their expression of HIF-α subtypes, into those expressing no HIF (VHL WT), HIF-1 and HIF-2 (H1H2), or H2-only (H2). Hypoxia-inducible factor-1 represses Myc by displacing it from its transcriptional binding sites, leading to pro-apoptotic p21 and p27 stabilisation. Conversely, HIF-2 enhances Myc activity, leading to enhanced CyclinD2 and E2F3 activity, thus conferring a more proliferative phenotype in the ‘H2’ tumours (Gordan et al, 2007). Hypoxia-inducible factor-2, but not HIF-1, has been shown to be necessary to overcome the tumour-suppressor effect of VHL in xenograft models (Maranchie et al, 2002; Covello et al, 2005; Raval et al, 2005). We hypothesise that miR-210 levels are dictated by the balance of HIF-1 vs HIF-2 activity. Thus, when both are present, HIF-1 predominates, but HIF-2 alone can function with a lower level of effect.
Interestingly, miR-210 expression inversely correlated with VHL mRNA expression. The primers to VHL were designed to target the 3′ UTR, and thus the expression measured by qRT–PCR should be of transcripts that have not been halted by a truncating mutation. The position or type of VHL mutation may lead to different copy numbers of the VHL transcript, and consequently different levels of functionality of the resulting VHL protein. However, it is recognised that missense mutations can also lead to loss of VHL function without changes in mRNA copy number.
We have previously shown that ISCU is a target of miR-210. Although this work was in completion, Neal et al (2010) showed that ISCU displayed an inverse relationship to miR-210 at mRNA level. We have confirmed this at both the mRNA and protein level, providing additional evidence of miR-210 activity in vivo. In contrast to their findings, however, we found that high miR-210 expression in CCRCC is associated with better prognosis and lower grade/stage of tumours. This was unexpected, with both our group and others having shown that miR-210 is correlated with poorer prognosis in other cancer types. However, CA9 expression has previously been shown to be associated with good prognosis in CCRCC (Bui et al, 2003, 2004).
The association of miR-210 with good clinico-pathological parameters in CCRCC is surprising. This is unexpected partly because of the presumed increased activity of the hypoxia-HIF axis relieved of its suppression by VHL. In addition, the loss of HIF-independent VHL-mediated suppression of targets such as cyclin D1 (Zatyka et al, 2002) or SP1 (Yuen et al, 2007) would be predicted to confer a more aggressive phenotype. However, although VHL inactivation in CCRCCs should lead to constitutive HIF activation and miR-210 upregulation, further loss of cell differentiation coupled with ongoing mutations may manifest with reduction in expression of genes such as miR-210. Perhaps a more likely explanation is that reduced miR-210 (and CA9) expression reflects a shift from HIF-1 to HIF-2 predominance. In support of this, we showed that miR-210 has an inverse relationship to Ki-67 expression in tumours. Though this is not necessarily a direct mechanistic association with miR-210, it has been shown that renal tumours expressing only HIF-2 exhibit increased growth rates and higher Ki-67 expression. Interestingly, Nakada et al (2011) showed that miR-210 overexpression resulted in growth suppression in renal cancer cell lines, with accumulation at G2/M phase. Although this would seem to support a protective effect of miR-210 in renal cancer, they also report miR-210 overexpression causing centrosome amplification and increased aneuploidy.
An explanation for the association of HIF-2-only tumours with higher proliferation is suggested in a model of wound re-epithilialisation in hypoxia. Keratinocyte proliferation, as measured by Ki-67 expression, was reduced in hypoxia due to HIF-1-mediated miR-210 overexpression, leading to repression of the cell-cycle regulatory protein, E2F3 (Biswas et al, 2010). A switch from HIF-1 to HIF-2 might, therefore, be predicted to increase proliferation through de-repression of E2F3. Low miR-210 in oesophageal squamous cell carcinoma has been associated with poorly differentiated tumours, with miR-210 acting as a tumour suppressor by downregulating fibroblast growth factor receptor-like 1, leading to cell-cycle arrest in G1G0 (Tsuchiya et al, 2011).
In conclusion, we provide further evidence of miR-210 upregulation in renal cancer. We show that its regulation is predominantly HIF-1-mediated, but that HIF-2 can regulate it in the absence of HIF-1, albeit to a lesser extent. In CCRCC, we have demonstrated that it correlates inversely with ISCU expression, both at the mRNA and protein level. Increased miR-210 is associated with lower tumour stage and grade, better survival and reduced proliferation. Finally, we show that VHL mRNA expression correlates inversely with miR-210 expression.
Change history
19 March 2013
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Biswas S, Roy S, Banerjee J, Hussain SR, Khanna S, Meenakshisundaram G, Kuppusamy P, Friedman A, Sen CK (2010) Hypoxia inducible microRNA 210 attenuates keratinocyte proliferation and impairs closure in a murine model of ischemic wounds. Proc Natl Acad Sci USA 107: 6976–6981
Bui MH, Seligson D, Han KR, Pantuck AJ, Dorey FJ, Huang Y, Horvath S, Leibovich BC, Chopra S, Liao SY, Stanbridge E, Lerman MI, Palotie A, Figlin RA, Belldegrun AS (2003) Carbonic anhydrase IX is an independent predictor of survival in advanced renal clear cell carcinoma: implications for prognosis and therapy. Clin Cancer Res 9: 802–811
Bui MH, Visapaa H, Seligson D, Kim H, Han KR, Huang Y, Horvath S, Stanbridge EJ, Palotie A, Figlin RA, Belldegrun AS (2004) Prognostic value of carbonic anhydrase IX and KI67 as predictors of survival for renal clear cell carcinoma. J Urol 171: 2461–2466
Camps C, Buffa FM, Colella S, Moore J, Sotiriou C, Sheldon H, Harris AL, Gleadle JM, Ragoussis J (2008) hsa-miR-210 Is induced by hypoxia and is an independent prognostic factor in breast cancer. Clin Cancer Res 14: 1340–1348
Chan SY, Zhang YY, Hemann C, Mahoney CE, Zweier JL, Loscalzo J (2009) MicroRNA-210 controls mitochondrial metabolism during hypoxia by repressing the iron-sulfur cluster assembly proteins ISCU1/2. Cell Metab 10: 273–284
Chen Z, Li Y, Zhang H, Huang P, Luthra R (2010) Hypoxia-regulated microRNA-210 modulates mitochondrial function and decreases ISCU and COX10 expression. Oncogene 29: 4362–4368
Chia SK, Wykoff CC, Watson PH, Han C, Leek RD, Pastorek J, Gatter KC, Ratcliffe P, Harris AL (2001) Prognostic significance of a novel hypoxia-regulated marker, carbonic anhydrase IX, in invasive breast carcinoma. J Clin Oncol 19: 3660–3668
Covello KL, Simon MC, Keith B (2005) Targeted replacement of hypoxia-inducible factor-1alpha by a hypoxia-inducible factor-2alpha knock-in allele promotes tumor growth. Cancer Res 65: 2277–2286
Elvidge GP, Glenny L, Appelhoff RJ, Ratcliffe PJ, Ragoussis J, Gleadle JM (2006) Concordant regulation of gene expression by hypoxia and 2-oxoglutarate-dependent dioxygenase inhibition: the role of HIF-1alpha, HIF-2alpha, and other pathways. J Biol Chem 281: 15215–15226
Favaro E, Ramachandran A, McCormick R, Gee H, Blancher C, Crosby M, Devlin C, Blick C, Buffa F, Li JL, Vojnovic B, Pires das Neves R, Glazer P, Iborra F, Ivan M, Ragoussis J, Harris AL (2010) MicroRNA-210 regulates mitochondrial free radical response to hypoxia and krebs cycle in cancer cells by targeting iron sulfur cluster protein ISCU. PLoS One 5: e10345
Fridman E, Dotan Z, Barshack I, David MB, Dov A, Tabak S, Zion O, Benjamin S, Benjamin H, Kuker H, Avivi C, Rosenblatt K, Polak-Charcon S, Ramon J, Rosenfeld N, Spector Y (2010) Accurate molecular classification of renal tumors using microRNA expression. J Mol Diagn 12: 687–696
Gee HE, Camps C, Buffa FM, Patiar S, Winter SC, Betts G, Homer J, Corbridge R, Cox G, West CM, Ragoussis J, Harris AL (2010) hsa-mir-210 is a marker of tumor hypoxia and a prognostic factor in head and neck cancer. Cancer 116: 2148–2158
Gordan JD, Bertout JA, Hu CJ, Diehl JA, Simon MC (2007) HIF-2alpha promotes hypoxic cell proliferation by enhancing c-myc transcriptional activity. Cancer Cell 11: 335–347
Gordan JD, Lal P, Dondeti VR, Letrero R, Parekh KN, Oquendo CE, Greenberg RA, Flaherty KT, Rathmell WK, Keith B, Simon MC, Nathanson KL (2008) HIF-alpha effects on c-Myc distinguish two subtypes of sporadic VHL-deficient clear cell renal carcinoma. Cancer Cell 14: 435–446
Harris AL (2002) Hypoxia—a key regulatory factor in tumour growth. Nat Rev Cancer 2: 38–47
Herman JG, Latif F, Weng Y, Lerman MI, Zbar B, Liu S, Samid D, Duan DS, Gnarra JR, Linehan WM (1994) Silencing of the VHL tumor-suppressor gene by DNA methylation in renal carcinoma. Proc Natl Acad Sci USA 91: 9700–9704
Ho AS, Huang X, Cao H, Christman-Skieller C, Bennewith K, Le QT, Koong AC (2010) Circulating miR-210 as a novel hypoxia marker in pancreatic cancer. Transl Oncol 3: 109–113
Huang WC, Swietach P, Vaughan-Jones RD, Glitsch MD (2009) Differentiation impairs low pH-induced Ca2+ signaling and ERK phosphorylation in granule precursor tumour cells. Cell Calcium 45: 391–399
Iliopoulos O, Kibel A, Gray S, Kaelin WG (1995) Tumour suppression by the human von Hippel-Lindau gene product. Nat Med 1: 822–826
Juan D, Alexe G, Antes T, Liu H, Madabhushi A, Delisi C, Ganesan S, Bhanot G, Liou LS (2010) Identification of a microRNA panel for clear-cell kidney cancer. Urology 75: 835–841
Kulshreshtha R, Ferracin M, Negrini M, Calin GA, Davuluri RV, Ivan M (2007) Regulation of microRNA expression: the hypoxic component. Cell Cycle 6: 1426–1431
Maranchie JK, Vasselli JR, Riss J, Bonifacino JS, Linehan WM, Klausner RD (2002) The contribution of VHL substrate binding and HIF1-alpha to the phenotype of VHL loss in renal cell carcinoma. Cancer Cell 1: 247–255
McCormick R, Buffa FM, Ragoussis J, Harris AL (2010) The role of hypoxia regulated microRNAs in cancer. Curr Top Microbiol Immunol 345: 47–70
Nakada C, Tsukamoto Y, Matsuura K, Nguyen TL, Hijiya N, Uchida T, Sato F, Mimata H, Seto M, Moriyama M (2011) Overexpression of miR-210, a downstream target of HIF1alpha, causes centrosome amplification in renal carcinoma cells. J Pathol 224: 280–288
Neal CS, Michael MZ, Rawlings LH, Van der Hoek MB, Gleadle JM (2010) The VHL-dependent regulation of microRNAs in renal cancer. BMC Med 8: 64
Pillai RS (2005) MicroRNA function: multiple mechanisms for a tiny RNA? RNA 11: 1753–1761
Pulkkinen K, Malm T, Turunen M, Koistinaho J, Yla-Herttuala S (2008) Hypoxia induces microRNA miR-210 in vitro and in vivo ephrin-A3 and neuronal pentraxin 1 are potentially regulated by miR-210. FEBS Lett 582: 2397–2401
Raval RR, Lau KW, Tran MG, Sowter HM, Mandriota SJ, Li JL, Pugh CW, Maxwell PH, Harris AL, Ratcliffe PJ (2005) Contrasting properties of hypoxia-inducible factor 1 (HIF-1) and HIF-2 in von Hippel-Lindau-associated renal cell carcinoma. Mol Cell Biol 25: 5675–5686
Rouault TA, Tong WH (2008) Iron-sulfur cluster biogenesis and human disease. Trends Genet 24: 398–407
Saarnio J, Parkkila S, Parkkila AK, Waheed A, Casey MC, Zhou XY, Pastorekova S, Pastorek J, Karttunen T, Haukipuro K, Kairaluoma MI, Sly WS (1998) Immunohistochemistry of carbonic anhydrase isozyme IX (MN/CA IX) in human gut reveals polarized expression in the epithelial cells with the highest proliferative capacity. J Histochem Cytochem 46: 497–504
Seliger B, Fedorushchenko A, Brenner W, Ackermann A, Atkins D, Hanash S, Lichtenfels R (2007) Ubiquitin COOH-terminal hydrolase 1: a biomarker of renal cell carcinoma associated with enhanced tumor cell proliferation and migration. Clin Cancer Res 13: 27–37
Tsuchiya S, Fujiwara T, Sato F, Shimada Y, Tanaka E, Sakai Y, Shimizu K, Tsujimoto G (2011) MicroRNA-210 regulates cancer cell proliferation through targeting fibroblast growth factor receptor-like 1 (FGFRL1). J Biol Chem 286: 420–428
Valera VA, Walter BA, Linehan WM, Merino MJ (2011) Regulatory effects of microRNA-92 (miR-92) on VHL gene expression and the hypoxic activation of miR-210 in clear cell renal cell carcinoma. J Cancer 2: 515–526
Weng L, Wu X, Gao H, Mu B, Li X, Wang JH, Guo C, Jin JM, Chen Z, Covarrubias M, Yuan YC, Weiss LM, Wu H (2010) MicroRNA profiling of clear cell renal cell carcinoma by whole-genome small RNA deep sequencing of paired frozen and formalin-fixed, paraffin-embedded tissue specimens. J Pathol 222: 41–51
White NM, Bao TT, Grigull J, Youssef YM, Girgis A, Diamandis M, Fatoohi E, Metias M, Honey RJ, Stewart R, Pace KT, Bjarnason GA, Yousef GM (2011) miRNA profiling for clear cell renal cell carcinoma: biomarker discovery and identification of potential controls and consequences of miRNA dysregulation. J Urol 186: 1077–1083
Young AC, Craven RA, Cohen D, Taylor C, Booth C, Harnden P, Cairns DA, Astuti D, Gregory W, Maher ER, Knowles MA, Joyce A, Selby PJ, Banks RE (2009) Analysis of VHL gene alterations and their relationship to clinical parameters in sporadic conventional renal cell carcinoma. Clin Cancer Res 15: 7582–7592
Yuen JS, Cockman ME, Sullivan M, Protheroe A, Turner GD, Roberts IS, Pugh CW, Werner H, Macaulay VM (2007) The VHL tumor suppressor inhibits expression of the IGF1R and its loss induces IGF1R upregulation in human clear cell renal carcinoma. Oncogene 26: 6499–6508
Zatyka M, da Silva NF, Clifford SC, Morris MR, Wiesener MS, Eckardt KU, Houlston RS, Richards FM, Latif F, Maher ER (2002) Identification of cyclin D1 and other novel targets for the von Hippel-Lindau tumor suppressor gene by expression array analysis and investigation of cyclin D1 genotype as a modifier in von Hippel-Lindau disease. Cancer Res 62: 3803–3811
Acknowledgements
We thank Dr Kaelin for supplying cell lines, Helen Turley and her colleagues for TMA processing, the ORB and our funders: Cancer Research UK, UCARE, The NIHR Oxford Biomedical Research Centre. This study was supported by the Cancer Research UK (ALH, REB and PJS); Wellcome Trust (JR); Royal College of Surgeons (RIM and CB); Oxford Health Services Research Committee (RIM); Urological Foundation (RIM and CB); Urology Cancer Research and Education (RIM and CB); Higher Education Funding Council for England (DRM); Wellcome Trust (JS); and NIHR Oxford Comprehensive Biomedical Research Centre (ALH).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
McCormick, R., Blick, C., Ragoussis, J. et al. miR-210 is a target of hypoxia-inducible factors 1 and 2 in renal cancer, regulates ISCU and correlates with good prognosis. Br J Cancer 108, 1133–1142 (2013). https://doi.org/10.1038/bjc.2013.56
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2013.56
Keywords
This article is cited by
-
Hypoxia-induced autophagy in triple negative breast cancer: association with prognostic variables, patients’ survival and response to neoadjuvant chemotherapy
Virchows Archiv (2023)
-
Diagnostic applications and therapeutic option of Cascade CRISPR/Cas in the modulation of miRNA in diverse cancers: promises and obstacles
Journal of Cancer Research and Clinical Oncology (2023)
-
Iron-sulphur cluster biogenesis factor LYRM4 is a novel prognostic biomarker associated with immune infiltrates in hepatocellular carcinoma
Cancer Cell International (2021)
-
Nickel nanoparticle-induced cell transformation: involvement of DNA damage and DNA repair defect through HIF-1α/miR-210/Rad52 pathway
Journal of Nanobiotechnology (2021)
-
The interplay between HIF-1α and noncoding RNAs in cancer
Journal of Experimental & Clinical Cancer Research (2020)
