
Abstract
Until recently, only retrospective studies had been published on salvage high-dose melphalan (HDM) with autologous stem cell ‘transplantation’ (ASCT). In a prospective, nonrandomized phase-2 study, we treated 53 bortezomib-naïve patients with bortezomib–dexamethasone as induction and bortezomib included in the conditioning regimen along with the HDM. Median progression-free survival (PFS), time to next treatment (TNT) and overall survival (OS) after start of reinduction therapy were 21.6, 22.8 and 46.6 months, respectively. For 49 patients who completed salvage bortezomib–HDM(II) with ASCT, there was no significant difference of PFS and TNT after HDM (II) compared with after the initial HDM(I), and thus patients were their own controls (PFS (I: 20.1 vs II: 19.3 months (P=0.8)) or TNT (I: 24.4 vs II: 20.7 months (P=0.8)). No significant differences in the response rates after salvage ASCT compared with the initial ASCT. Bortezomib–HDM conditioning combo was feasible, and toxicity was as expected for patients treated with bortezomib and ASCT. In conclusion, in bortezomib-naïve patients treated at first relapse with salvage ASCT including bortezomib, PSF and TNT did not differ significantly from initial ASCT and median OS was almost 5.5 years with acceptable toxicity. A recent prospective randomized study confirms salvage ASCT to be an effective treatment.
Similar content being viewed by others

Introduction
With the introduction of high-dose melphalan (HDM) followed by autologous stem cell ‘transplantation’ (ASCT) and the use of new agents, the outcomes of patients with multiple myeloma have steadily improved. However, multiple myeloma is still an incurable disease, and patients will eventually relapse after front-line therapy. Because of the fact that ASCT is a highly efficient therapy in a majority of patients, it is a widespread routine to harvest a sufficient number of stem cells for at least two transplantations. A second ASCT can then be offered to relapsing patients who are still considered young and fit enough for this treatment. However, only few reports of the results of a second ASCT in the relapse setting had been published and all studies were retrospective,1, 2, 3, 4, 5, 6, 7 as recently reviewed.8 Recently, the first prospective phase-3 study was published from the UK.9 The duration of disease control after salvage ASCT has usually been observed to be shorter than after the initial ASCT.
It is a general observation that the time from first ASCT to relapse has a great impact on the prognosis for both progression-free survival (PFS) after second-line treatment and for overall survival (OS).10, 11, 12, 13, 14 New drugs such as bortezomib and IMIDs, thalidomide and lenalidomide have improved response rate and response duration and are more efficient as second-line treatment than conventional chemotherapy.15, 16 Furthermore, there are indications that treatment with bortezomib may overcome the adverse prognostic importance of some of the high-risk cytogenetic aberrations in multiple myeloma like t(4;14).17
We conducted a prospective study to explore the efficacy of salvage high-dose therapy with ASCT at first symptomatic relapse preceded by induction therapy with bortezomib and dexamethasone and inclusion of bortezomib in the conditioning regimen of ASCT, which has also been addressed by the French group,18 the Italian group19 and most recently a Japanese group20 and was shown to be feasible in a phase-1/2 study.21
Materials and methods
Inclusion criteria
Patients with multiple myeloma at first symptomatic relapse, who had been treated with HDM followed by ASCT as first-line treatment, were eligible for inclusion, if they had preserved at least 2.0 × 106 CD34+ frozen stem cells/kg body weight.
Exclusion criteria
Patients were excluded if they had received former treatment with bortezomib, had neuropathy grade ⩾3 or had WHO performance status >3.
Study design
The trial was a prospective nonrandomized phase-2 study.
Study treatment
Three courses of intravenous bortezomib (Velcade) at a dose of 1.3 mg/m2 on days 1, 4, 8 and 11 and oral dexamethasone at a dose of 20 mg on days 1, 2, 4, 5, 8, 9, 11 and 12 were followed by HDM (200 mg/m2) on day −2 and intravenous bortezomib at a dose of 1.3 mg/m2 on days −5 and −2, and subsequent infusion of at least 2.0 × 106 CD34+ stem cells on day 0. Prophylactic antiviral, antibacterial, and antifungal treatment and G-CSF were given according to local routine. Bortezomib dose was reduced to 1.0 mg/m2 and subsequently to 0.7 mg/m2 in the case of neurotoxicity according to the manufacturer’s instructions. The primary end point was a comparison of the PFS after salvage HDM with stem cell support (ASCT) with PFS after first ASCT. Secondary end points were (1) to determine the tolerability of including bortezomib in the conditioning regimen with HDM; (2) to determine the response rates of the salvage ASCT according to IMWG criteria;22 and (3) to determine the time schedule for marrow regeneration (neutrophil and platelet recovery) after the second ASCT. Furthermore, the efficacy in patients with early relapse (within first year) after first ASCT vs later relapse was explored.
All patients signed a written informed consent before inclusion. The study was approved by the ethics committees and health authorities in all participating countries and conducted in accordance with the Helsinki declaration of 1975 and the Guidelines for Good Clinical Practice. This study was registered at www.clinicaltrials.gov as no. NCT00508209.
Statistical analysis
OS, PFS (event: progression or death of any cause) and time to next treatment (TNT) after salvage ASCT all had censored observation and were analyzed using the Kaplan–Meier method and Cox proportional hazard models.
Unless otherwise mentioned, OS, TNT and PFS were calculated from the start of bortezomib treatment. To compare TNT and PFS after initial ASCT and salvage ASCT, we calculated the ratio between TNT after salvage and initial ASCT and PFS after salvage and initial ASCT. These ratios were analyzed using the Kaplan–Meier method.
The McNemar test using exact P-values was used for comparisons of paired ordinal variables.
All P-values were two-sided, and P-values below 0.05 were considered significant. R version 3.0.0 was used for all calculations (R foundation for statistical computing, Vienna, Austria).
Results
Between 17 July 2007 and 8 June 2009, 53 patients with their first relapse after upfront HDM with ASCT were included, and the characteristics at inclusion are presented in Table 1. Consecutive patients fulfilling the inclusion criteria were included at each center. The initial induction therapy had been standard vincristine, doxorubicin, dexamethasone (VAD) or cyclophosphamide and dexamethasone (CTX/Dex), as previously described.23 No patient had received consolidation therapy, whereas seven patients had received Interferon-α 2b maintenance after the initial ASCT. Cytogenetics or fluorescence in situ hybridization (FISH) were not a part of the trial, and retospectively 36 patients had neither karyotype nor FISH results and therefore these results are not presented here. All patients received standard dose reinduction treatment with bortezomib and dexamethasone, but four patients never came to salvage HDM: one patient died from multiorgan failure after only one bortezomib injection, one patient developed respiratory distress syndrome and two patients developed progressive disease (see Figure 1). The median number of CD34+ stem cells given was 3.63 (range: 2.0–12.1) × 106/kg body weight.

Phase 2 study of bortezomib–dexamethasone reinduction followed by bortezomib–high-dose melphalan (HDM-Btz) with autologous stem cell support (ASCT) at first relapse after initial ASCT. Survey of included patients.
Marrow regeneration
Time to neutrophils above 0.5–1.0 × 109/L were 11 days (range 10–14) and 12 days (range 7–41), respectively. Time to platelets above 20–100 × 109/L were 11 days (range 0–20) and 21 days (range 11–48), respectively. The overall median follow-up time was 30.4 months.
Survival and response rates
The median follow-up times were 19.3, 19.4 and 30.9 months for median PFS, TNT and OS, respectively. The PFS, TNT and OS after the start of reinduction therapy were 21.6, 22.8 and 46.6 months, respectively (Figure 2). For the 49 patients who completed the salvage bortezomib–HDM with ASCT, the EFS, TNT and OS after ASCT were 19.3, 20.7 and 44.3 months, respectively. An updated survival from February 2015 with an overall follow-up time for OS of 51.1 months showed a median OS of 65.7 months (95% CI: 44.6;79.9).

Kaplan–Meier plot of overall survival (OS), progression-free survival (PFS) and time to next treatment (TNT) from start of reinduction therapy of all included patients. The Y axis indicates the event-free survival (event=death or PD (PFS) or next treatment (TNT)).
The overall response rates were complete response/near complete response (CR/nCR) 32.1%, very good partial response (VGPR) 28.3%, partial response (PR) 26.4%, minor response (MR) 1.9%, progressive disease (PD) 3.8% and non-evaluable (NE) 3.8% for the 53 included patients. The response rates for the 49 patients who completed ASCT appear from Table 2 showing response rates before and after ASCT. Altogether, 35% of the patients achieved CR/nCR after salvage ASCT, whereas 22% of the patients achieved CR/nCR after initial ASCT. Nine patients (18%) had better response after salvage ASCT, and three patients (6%) had the best response after primary ASCT, although this difference was not significant (P=0.14, McNemar test).
Response after initial induction therapy compared with response after reinduction
Eighteen patients improved the depth of response from the initial induction to the velcade–dex induction (9 to CR/nCR (4 from PR, 4 from SD and 1 from NE), 6 to VGPR (5 from PR and 1 from SD), 2 from SD to PR and 1 from PD to SD), whereas 10 patients had less deep responses (one from CR/nCR to PR, 8 from PR (6 to SD and 2 to PD) and 1 from SD to PD). Eleven patients had the same response as that after the initial induction, whereas response evaluation was not possible in four patients. There was a significant relationship between the CR/nCR and PFS (P=0.047), but not between overall response rate (PR or better) and PFS (P>0.13).
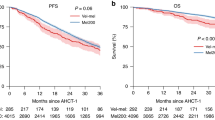
Comparison between the salvage ASCT and the initial ASCT shows no significant difference of PFS (I: 20.1 vs II: 19.3 months (P=0.8)) or TNT (I: 24.4 vs II: 20.7 months (P=0.8)) (Figure 3). There was a significant correlation between PFS after the initial ASCT and the salvage ASCT (P=0.0005, Cox regression). Eleven patients, who had relapsed within the first year after initial ASCT, had median 10.0 months PFS compared with 24.4 months in patients with later relapse (P=0.009). Twenty-one patients, who had relapsed within the first 2 years after initial ASCT, had median 11.5 months PFS compared with 28.6 months in patients with later relapse (P=0.002). The median ratio between TNT after salvage and initial ASCT was 0.71 (CI: 0.60–0.92), and the median ratio between PFS after salvage and initial ASCT was 0.8 (CI: 0.64–1.108).

Kaplan–Meier Plot of PFS II after salvage autologous stem cell transplantation (ASCT) compared with PFS I after initial ASCT (a) and TNT II after salvage ASCT compared with TNT I after initial ASCT (b). The Y axis indicates the event-free survival (event=death or PD (PFS) (a) or next treatment (TNT) (b)).
Toxicity
Neurotoxicity data are presented in Table 3. About half of the patients had some degree of neurotoxicity after the induction therapy. In three patients, the neuropathy progressed after the combination of bortezomib and HDM. The neurological symptoms resolved in most of the patients after high-dose therapy. However, four patients had unresolved neuropathy (one patient with grade 3 neuropathic pain, one patient with grade 3 sensory neuropathy and two patients with combined neuropathic pain and sensory neuropathy). Although the symptoms disappeared in three of these patients within 6–12 months, one patient still had unchanged symptoms >1 year after ASCT. Non-neurological toxicity is presented in Table 4 and it did not differ from what is seen in other patients treated with HDM and ASCT.
Discussion
In this prospective study, we demonstrate that reinduction with bortezomib and dexamethasone and addition of bortezomib to conditioning HDM is a feasible treatment with longer PFS than expected. By intention-to-treat analysis, the study population had a median PFS of about 20 months and an overall survival of almost 5.5 years after a second ASCT.
Richardson et al.24 showed in the APEX study that bortezomib single-drug treatment gave a PFS of 8.1 months in a bortezomib-naive population receiving second-line treatment, including two-thirds initially treated with stem cell transplantation or other high-dose regimens. Hjorth et al.25 found similar PFS for patients treated with bortezomib–dexamethasone (7.2 months) and thalidomide-dexamethasone (9 months) as second-line therapy in patients who had not received prior thalidomide or bortezomib treatment. In a phase-2 study, Palumbo et al.26 found a somewhat longer PFS (17 months) in 62 patients receiving thalidomide–dexamethasone as second-line treatment, and most of the patients (97%) had initially received ASCT. Stadtmauer et al.16 analyzed two large phase-3 studies of lenalinomide–dexamethasone in relapsed or refractory myeloma (MM-009 and MM-010) with respect to second-line treatment and found PFS of 14.1 months and OS of 42.0 months, and here 67% of these patients had received initial ASCT. Thus, our results are better than the findings in most published studies on second-line treatment in relapsed myeloma patients. However, one must be cautious when comparing different studies, as the selection of patients has a great impact on the prognosis, as indicated by the significance of the first PFS after initial treatment as documented in the present study.
In this study, we did not find any significant difference in PFS or TNT after the salvage ASCT compared with the first ASCT, which was better than expected. This comparison may be problematic as death is included as an event, but obviously it could only be an issue after salvage ASCT. However, this would introduce a bias for better median PSF and TNT than average after an initial ASCT. On the other hand, the 49 patients who completed salvage ASCT were selected, but still they were their own controls. Therefore, the results are interesting and important.
In a recent retrospective analysis of salvage second ASCT, Michaelis et al.1 reported registry data from 187 patients reported to the Center for International Blood and Bone Marrow Transplant Research (CIBMTR).
The authors also reviewed five other retrospective studies on salvage ASCT in multiple myeloma. The results showed a medium PFS of 8.5–16.4 months and OS of 19–53 months where the time to relapse after the initial ASCT had a major impact on the PFS after the salvage ASCT. The conclusion was that salvage ASCT should be considered only in patients who relapse/progress later than 1.5 years after the initial ASCT. This is in accordance with the review by Atanackovic and Schilling.8 Our results show a little longer PFS and OS after salvage ASCT with bortezomib in bortezomib-naïve patients and a median OS of about 10 months for patients with PFS <1.5 years after the initial ASCT, and this is longer than 6 months OS reported by Alvares et al.6 The improved depth of response induced by reinduction with bortezomib–dexamethasone may partly be responsible for the effect by salvage ASCT in the present study of bortezomib-naïve patients. However, as the treatment of younger newly diagnosed myeloma patients still improves with inclusion of new drugs in the induction therapy and by inclusion of consolidation and/or maintenance therapy, the future use of salvage ASCT should still be subject for prospective randomized clinical studies where the treatment is adjusted to the former treatment of the patients.
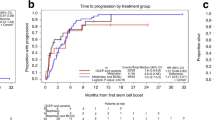
In the only prospective randomized study published most recently, Cook et al.9 compared salvage HDM with ASCT to weekly oral cyclophosphamide in patients who had not progressed during reinduction with PAD (bortezomib–doxorubicin–dexamethasone). They showed improved PFS of 19 months compared with 11 months in the cyclophosphamide group and comparable to the findings in the present study of 19.3 months.
In our study, the quality of the response shows a trend to improve by increasing the percentage of VGPR or CR/nCR from 54 to 66.5, and in one-third of the patients VGPR was achieved before HDM–bortezomib. In the retrospective study of Center for International Blood and Bone Marrow Transplant Research (CIBMTR), the chemosensitivity and disease status had no effect on outcomes after the salvage ASCT.1 In addition, the response rates were comparable to the phase-3 study showing 59% VGPR or better.9
The combination of bortezomib and HDM was generally well tolerated. The expected side effects were mainly of low grade. Some patients experienced a flare-up of the neurological side effects following salvage HDM–bortezomib with stem cell support, and in one patient the symptoms seem to have become chronic. In all other cases the neurological symptoms had disappeared after 6−12 months. In the phase-1/2 trial of the combination of bortezomib and ASCT, Lonial et al.21 did not report any neurological adverse event, possibly because only 60% of their patients had received bortezomib before and they only used a single dose in connection with ASCT. The neurotoxicity might be further reduced by administering bortezomib subcutaneously;27 however, this was not approved at the time of the present study. Four of the 53 patients never went on with ASCT, one because of early death, one because of toxicity and two because of progressive disease. The retrospective studies gave no information of how many patients were excluded before planned salvage ASCT.
In conclusion, the findings in our study support the use of salvage HDM–bortezomib after reinduction with bortezomib and dexamethasone induction at least in bortezomib-naive patients. Our study shows an efficacy comparable to the recent prospective randomized study that documented the efficacy of salvage HDM compared with cyclophosphamide after induction with the bortezomib-containing regimen PAD. More prospective randomized studies are needed to find the optimal place and regimen for salvage HDM eventually stratified for the initial induction therapies.
References
Michaelis LC, Saad A, Zhong X, Le-Rademacher J, Freytes CO, Marks DI et al. Salvage second hematopoietic cell transplantation in myeloma. Biol Blood Marrow Transplant 2013; 19: 760–766.
Hong JY, Choi MK, Kim DH, Kim SJ, Kim K, Kim CW et al. Feasibility of second hematopoietic stem cell transplantation using reduced-intensity conditioning with fludarabine and melphalan after failed autologous stem cell transplantation. Transplant Proc 2010; 42: 3723–3728.
Krivanova A, Hajek R, Krejci M, Scudla V, Indrak K, Bacovsky J et al. Second autologous transplantation for multiple myeloma patients relapsing after the first autograft—a pilot study for the evaluation of experimental maintenance therapies. Report of the prospective non-randomized pilot study of the Czech Myeloma Group. Onkologie 2004; 27: 275–279.
Olin RL, Vogl DT, Porter DL, Luger SM, Schuster SJ, Tsai DE et al. Second auto-SCT is safe and effective salvage therapy for relapsed multiple myeloma. Bone Marrow Transplant. 2009; 43: 417–422.
Shah N, Ahmed F, Bashir Q, Qureshi S, Dinh Y, Rondon G et al. Durable remission with salvage second autotransplants in patients with multiple myeloma. Cancer 2012; 118: 3549–3555.
Alvares CL, Davies FE, Horton C, Patel G, Powles R, Morgan GJ . The role of second autografts in the management of myeloma at first relapse. Haematologica 2006; 91: 141–142.
Sellner L, Heiss C, Benner A, Raab MS, Hillengass J, Hose D et al. Autologous retransplantation for patients with recurrent multiple myeloma: a single-center experience with 200 patients. Cancer 2013; 119: 2438–2446.
Atanackovic D, Schilling G . Second autologous transplant as salvage therapy in multiple myeloma. Br J Haematol 2013; 163: 565–572.
Cook G, Williams C, Brown JM, Cairns DA, Cavenagh J, Snowden JA et al. High-dose chemotherapy plus autologous stem-cell transplantation as consolidation therapy in patients with relapsed multiple myeloma after previous autologous stem-cell transplantation (NCRI Myeloma X Relapse [Intensive trial]): a randomised, open-label, phase 3 trial. Lancet Oncol 2014; 15: 874–885.
Alegre A, Granda A, Martinez-Chamorro C, Diaz-Mediavilla J, Martinez R, Garcia-Larana J et al. Different patterns of relapse after autologous peripheral blood stem cell transplantation in multiple myeloma: clinical results of 280 cases from the Spanish Registry. Haematologica 2002; 87: 609–614.
Alvares CL, Davies FE, Horton C, Patel G, Powles R, Sirohi B et al. Long-term outcomes of previously untreated myeloma patients: responses to induction chemotherapy and high-dose melphalan incorporated within a risk stratification model can help to direct the use of novel treatments. Br J Haematol 2005; 129: 607–614.
Lenhoff S, Hjorth M, Turesson I, Westin J, Gimsing P, Wisloff F et al. Intensive therapy for multiple myeloma in patients younger than 60 years. Long-term results focusing on the effect of the degree of response on survival and relapse pattern after transplantation. Haematologica 2006; 91: 1228–1233.
Cook G, Liakopoulou E, Pearce R, Cavet J, Morgan GJ, Kirkland K et al. Factors influencing the outcome of a second autologous stem cell transplant (ASCT) in relapsed multiple myeloma: a study from the British Society of Blood and Marrow Transplantation Registry. Biol Blood Marrow Transplant. 2011; 17: 1638–1645.
Hermansen NE, Gimsing P . Patient heterogeneity in phase II studies of refractory disease in multiple myeloma—the ‘spell’ of the time to first relapse. Br J Haematol 2008; 140: 115–116.
Musto P, Falcone A, Sanpaolo G, Guglielmelli T, Zambello R, Balleari E et al. Bortezomib (Velcade) for progressive myeloma after autologous stem cell transplantation and thalidomide. Leuk Res 2006; 30: 283–285.
Stadtmauer EA, Weber DM, Niesvizky R, Belch A, Prince MH, San Miguel JF et al. Lenalidomide in combination with dexamethasone at first relapse in comparison with its use as later salvage therapy in relapsed or refractory multiple myeloma. Eur J Haematol 2009; 82: 426–432.
Avet-Loiseau H, Leleu X, Roussel M, Moreau P, Guerin-Charbonnel C, Caillot D et al. Bortezomib plus dexamethasone induction improves outcome of patients with t(4;14) myeloma but not outcome of patients with del(17p). J Clin Oncol 2010; 28: 4630–4634.
Roussel M, Moreau P, Huynh A, Mary JY, Danho C, Caillot D et al. Bortezomib and high-dose melphalan as conditioning regimen before autologous stem cell transplantation in patients with de novo multiple myeloma: a phase 2 study of the Intergroupe Francophone du Myelome (IFM). Blood 2010; 115: 32–37.
Palumbo A, Avonto I, Bruno B, Falcone A, Scalzulli PR, Ambrosini MT et al. Intermediate-dose melphalan (100 mg/m2/bortezomib/thalidomide/dexamethasone and stem cell support in patients with refractory or relapsed myeloma. Clin Lymphoma Myeloma 2006; 6: 475–477.
Miyamoto T, Yoshimoto G, Kamimura T, Muta T, Takashima S, Ito Y et al. Combination of high-dose melphalan and bortezomib as conditioning regimen for autologous peripheral blood stem cell transplantation in multiple myeloma. Int J Hematol 2013; 98: 337–345.
Lonial S, Kaufman J, Tighiouart M, Nooka A, Langston AA, Heffner LT et al. A phase I/II trial combining high-dose melphalan and autologous transplant with bortezomib for multiple myeloma: a dose- and schedule-finding study. Clin Cancer Res 2010; 16: 5079–5086.
Durie BG . Use of bisphosphonates in multiple myeloma: IMWG response to Mayo Clinic consensus statement. Mayo Clin Proc 2007; 82: 516–517.
Mellqvist UH, Lenhoff S, Johnsen HE, Hjorth M, Holmberg E, Juliusson G et al. Cyclophosphamide plus dexamethasone is an efficient initial treatment before high-dose melphalan and autologous stem cell transplantation in patients with newly diagnosed multiple myeloma: results of a randomized comparison with vincristine, doxorubicin, and dexamethasone. Cancer 2008; 112: 129–135.
Richardson PG, Sonneveld P, Schuster MW, Irwin D, Stadtmauer EA, Facon T et al. Bortezomib or high-dose dexamethasone for relapsed multiple myeloma. N Engl J Med 2005; 352: 2487–2498.
Hjorth M, Hjertner O, Knudsen LM, Gulbrandsen N, Holmberg E, Pedersen PT et al. Thalidomide and dexamethasone vs bortezomib and dexamethasone for melphalan refractory myeloma: a randomized study. Eur J Haematol 2012; 88: 485–496.
Palumbo A, Falco P, Ambrosini MT, Petrucci MT, Musto P, Caravita T et al. Thalidomide plus dexamethasone is an effective salvage regimen for myeloma patients relapsing after autologous transplant. Eur J Haematol 2005; 75: 391–395.
Moreau P, Coiteux V, Hulin C, Leleu X, van d V, Acharya M et al. Prospective comparison of subcutaneous versus intravenous administration of bortezomib in patients with multiple myeloma. Haematologica 2008; 93: 1908–1911.
Acknowledgements
We thank all of the patients who participated in this study and the study nurses from all of the study sites. Drs Peter Gimsing, Øyvind Hjertner, Niels Abildgaard, Niels Frost Andersen, Tobias Gedde Dahl, Henrik Gregersen,, Ulf-Henrik Mellqvist, Olle Linder, Roald Lindås, Nielsaage Tøffner Clausen and Stig Lenhoff performed the research and contributed data from the included patients. Drs Peter Gimsing, Øyvind Hjertner and Stig Lenhoff designed the research study. Drs Peter Gimsing and Tobias W. Klausen analyzed the data. Drs Peter Gimsing, Øyvind Hjertner and Stig Lenhoff wrote the paper. All authors critically reviewed and approved the final manuscript.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
Janssen-Cilag supplied the study with free bortezomib and supported the expenses for conducting the study with a grant. Janssen-Cilag, together with Celgen and Mundipharma, are sponsors of The Nordic Myeloma Study Group. During the trial, the Nordic Myeloma Study Group has also received funding from the Nordic Cancer Union. P. Gimsing has received lecture honaria from Amgen. N. Abildgaard has received research grants Celgene and Janssen-Cilag. UH Mellqvist has received lecture honoraria from Celgene, Jansen, Mundipharma and Amgen. All remaining authors have declared no conflicts of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Gimsing, P., Hjertner, Ø., Abildgaard, N. et al. Salvage bortezomib–dexamethasone and high-dose melphalan (HDM) and autologous stem cell support (ASCT) in myeloma patients at first relapse after HDM with ASCT. A phase-2 trial. Bone Marrow Transplant 50, 1306–1311 (2015). https://doi.org/10.1038/bmt.2015.125
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2015.125
This article is cited by
-
Novel agent-based salvage autologous stem cell transplantation for relapsed multiple myeloma
Annals of Hematology (2017)
-
Re-invigorating rather than re-inventing the wheel: augmenting the impact of salvage autologous stem cell transplantation for multiple myeloma in the era of novel agents
Bone Marrow Transplantation (2015)
