
Abstract
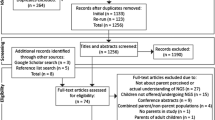
Parents' preferences for unsolicited findings (UFs) from diagnostic whole-exome sequencing (WES) for their children remain largely unexplored. Our aim was to gain insight into parental considerations favoring acceptance/decline of UFs pertaining to their child. We conducted 20 qualitative, semistructured interviews with parents (n=34) of children with a developmental delay, aged <1 to 17 years, after consenting to WES, but before feedback of results. Key findings from our study were that all parents favored acceptance of UFs for medically actionable conditions in childhood, but that preferences and considerations diverged for UFs with no medical actionability, or only in adulthood, and regarding carrier-status. Sometimes non-medical utility considerations (considerations of usefulness of knowing UFs, not rooted in (preventive) medical treatment or controls) were given in favor of disclosure of UFs. Sometimes the child's future autonomy formed a reason to withhold UFs at present, despite an unfavorable prognosis concerning the child's cognitive capabilities. Some parents only preferred receiving UFs if these findings were directly related to their reasons for seeking a diagnosis. These findings are essential for developing morally responsible policy and for counseling. Further research should focus on whether considerations of non-medical utility alone can justify disclosure of UFs and whether reasons for seeking a diagnosis place further constraints on what UFs may be returned/withheld. How parents can be aided in contemplating different scenarios regarding their child's future development also deserves further inquiry.
Similar content being viewed by others

Introduction
Next-generation sequencing technologies, such as whole-exome sequencing (WES) and whole-genome sequencing, map much vaster parts of persons’ DNA than traditional methods, and are therefore useful for reaching a diagnosis in cases of suspected, yet unclarified, genetic disorders. However, compared with previous genetic assays, these techniques also increase the chance of unsolicited findings (UFs).1, 2 This feature of next-generation sequencing technology raises the question what UFs may be disclosed/withheld and under what conditions and how UFs should be presented during counseling so that informed consent is safeguarded.3, 4, 5 These questions become all the more pressing in child cases, for which parents must give their proxy consent. Given that next-generation sequencing may reveal UFs concerning predispositions for conditions not only clinically relevant and actionable in childhood but also conditions with adult onset that may or may not be actionable, or only at a later stage in the child’s adult life, specific moral questions arise regarding the conditions for disclosure. Should choices about disclosure of UFs regarding the child belong to the freedom of parents? Or should certain UFs always be disclosed in childhood, for example, due to their medical actionability, while others should never be disclosed in childhood, for example, to safeguard the child’s future autonomy?6, 7
International policy statements, both in the past and present, have taken different moral standpoints on these questions. As Bredenoord et al has noticed, a gradual shift appears to be taking place in international policy contexts: some current policies stress protecting the child’s future autonomous decision-making (or a ‘right to an open future’8, 9), which echoes various policy recommendations regarding genetic testing in the past and directs certain choices for UFs to be deferred until adulthood;10, 11, 12 yet, some policies have taken a family-based approach,13 thus entrusting more discretion over UFs to parents.14
The direction that policy should take depends on ethical justification and on insights from empirical studies: we need to know why persons (do not) want to know certain UFs; what their experiences are during decision-making; and what problems they encounter in making choices. Such insights serve as input for ethical reflection and can help further specify what parents’ and genetic professionals’ moral responsibilities are toward children in the different situations in clinical practice, which is needed for responsible policy development.
The aim of this research was to gain insight into parents’ preferences and considerations concerning return of UFs for their child undergoing diagnostic WES in trio-analyses. Although we also inquired about parents’ preferences regarding UFs pertaining to themselves, the focus of this paper is limited to considerations regarding the child because of the specific ethical issues that arise about (non)disclosure of UFs in child cases. The policy that parents consented to allowed for some freedom of choice over UFs (Table 1). To date, few empirical qualitative studies have investigated the preferences and considerations of parents actually confronted with the choice about (non)disclosure of UFs from clinical WES for their child.15, 16, 17 Our study, which was conducted in the Netherlands where WES is part of standard clinical genetics care18 and health insurers reimburse the costs for its use in diagnostics, is one of the first studies to research non-hypothetical parental considerations for favoring acceptance or decline of UFs in a clinical setting.
Materials and methods
Recruitment occurred through clinical geneticists at the University Medical Center Utrecht, who offered preliminary information about the research to parents and asked if the research team could contact them. CC contacted parents about participation and obtained informed consent before interviews (for further information see Supplementary Materials and Methods).
At the time of this study, University Medical Center Utrecht had just started using WES for diagnostic purposes, initially limiting its use to cases of intellectual disability with/without multiple congenital abnormalities. None of the children met the legal criteria for competence owing to developmental delay and age. We, therefore, only investigated the views of parents. Inclusion criteria were that parents: had undergone pretest counseling for WES; gave consent for WES for their child before the interview; and had not yet received results.
Twenty interviews were conducted with parents (n=34) of children aged <1 to 17 at parents’ residences (see Table 2 for participant characteristics). Six of the interviews were conducted with one parent (1 with a father and 5 with mothers); all other interviews were conducted with both parents or partially with both parents. Parents were married or living together at the time of the interviews.
Our multidisciplinary research team, including a psychologist, a pediatrician, clinical geneticists and ethicists, devised a semistructured topic list for the interviews. Interview questions (see Supplementary Materials and Methods) focused on parents’ preferences for predefined categories of UFs that had been explained to them during pretest counseling; considerations favoring acceptance/decline of those categories; and views regarding the center’s policy standpoints (ie, always/never return or opt-out) for the various categories. Interviews were audio-recorded and then transcribed by a commissioned typist. Each interview transcript was open coded by two authors separately (CC analyzed all transcripts with either MvS or IB), then consensus was reached on the coding. Open codes were then grouped into themes using the NVivo 10 Software (QSR International Ply Ltd., Doncaster, VIC, Australia) for qualitative data management.
Results
All of the respondents wished to receive UFs for severe, medically actionable results in childhood. Preferences did, however, diverge for the other three categories. Different groups of considerations emerged from the data. Table 3 summarizes considerations according to whether they favored acceptance/decline of the various categories of UFs and offers illustrative quotes. Below considerations favoring disclosure are first discussed and then considerations favoring nondisclosure.
Groups of considerations favoring disclosure of UFs
Availability of medical treatment and prevention
All parents wished to receive UFs for severe medically actionable conditions in childhood because of the availability of medical treatment or prevention (controls), stressing that this was in their child’s best interest. Some also wished to receive any UFs for medically actionable conditions in childhood – not just severe ones as stated in the center’s policy. Designing a sound treatment plan for all of the child’s health problems was also viewed as an important aim, including limiting drug interactions and not choosing drugs with certain side effects for one condition that could worsen another condition.
This theme also emerged among some parents’ reasoning for receiving UFs related to severe conditions only medically actionable in adulthood. Some parents viewed timing of onset to be irrelevant. This was because they felt they would always remain responsible for making (medical) decisions for their child as a result of the child’s intellectual disability or because they had uncertainty about whether they would always have this responsibility for their child. Some regarded the availability of (preventive) medical treatment as trumping other types of considerations, for example, concerning the child’s future autonomy – even if it eventually became clearer that the child could possibly develop decisional competence.
Possible future availability of medical treatment and prevention
For UFs for medically inactionable conditions, parents often cited the possible future availability of (preventive) medical treatment as warranting disclosure at present. A few parents of young children also mentioned this as a reason for disclosure of UFs for conditions only medically actionable in adulthood, as (preventive) treatment for such conditions might become available at an earlier stage, that is, during childhood. Some of these parents also stressed that the reason they wished to receive these findings at present, rather than later in the child’s life, was because they had concerns or unclarity about recontact procedures or because of the unlikelihood that they would recontact the center to ask these types of questions, especially if they received a diagnosis through WES. Sometimes definitions concerning medical ‘actionability’/‘inactionability’ were not clear to parents and they wanted concrete examples.
Utility: beyond medical intervention
The potential non-medical utility (ie, usefulness not rooted in (preventive) medical treatment/controls) of knowledge of UFs was often emphasized. Examples included being able to gain more specific instructions on caring for one’s child; alertness to the development of symptoms associated with a condition, including conveying the risks of developing the condition to those involved in the child’s (daily) surroundings, for example, school, daycare; and avoiding another diagnostic odyssey.
Another relevant consideration in favor of acceptance was to avoid feelings of regret or guilt that might arise if medically actionable findings with child/adult onset were not disclosed and it turned out to be too late to optimally attend to the child’s problem(s). Parents also stated that knowledge of such UFs was for their own peace of mind.
Some parents who had reservations about receiving (some types of) UFs actually preferred to receive certain findings at present, to avoid anticipated anxiety that could be caused because of uncertainty about whether UFs for severe conditions were found, but never disclosed to them. This could occur if parents preferred not to hear a finding (as could be the case with severe conditions only medically actionable in adulthood – the center’s policy allows parents to choose whether or not to receive these findings) or because current policy did not allow for disclosure (as could be the case for severe medically inactionable conditions). In contrast, other parents did not have reservations about receiving UFs, but did mention wanting to avoid projected anxiety as an ancillary consideration to their other reasons favoring acceptance, such as the availability of medical treatment/prevention and wanting to avoid feelings of regret or guilt.
Parents sometimes also expressed a strong need to be in control of their child’s situation now and in the future and to avoid feelings of powerlessness, especially given the child’s present medical situation. These parents thought that receiving UFs could help them visualize what their child’s future could look like and help them gain a sense of security. This type of reasoning was seen for both medically actionable and inactionable UFs. Concerning inactionable UFs, some parents saw this potential utility to outweigh any negative effects of knowing such results for themselves/the child. Incidentally, some parents thought it was a viable option never to share these UFs with their child, even if it did become clearer that the child could become autonomous, for example, if WES revealed a mutation for a condition that predicted the child could become autonomous.
For severe, inactionable medical conditions, life planning was also important. Concrete examples included saving for a family vacation; stopping working (earlier); saving vacation days; advising the child in study and career choices, for example, whether to choose a lengthy university study or do something else with their life. Life planning was sometimes also mentioned as a relevant consideration for favoring acceptance of UFs for medically actionable conditions, as some conditions could turn out to be fatal or permanently impede normal functioning despite treatment. Some parents who underlined this reasoned according to the worst possible scenario, which was sometimes influenced by prior life events, such as the death of one of their children.
Emotional preparation of the child, other children in the family, the parents themselves and other relatives was also important for some parents. Parents sometimes emphasized that because their child had a cognitive impairment/psychological condition, emotionally preparing them for developing another condition and/or for treatment was especially important. Concerning medically inactionable conditions, some parents said that they wished to receive these findings at present, so that they could start their grieving process now as opposed to later, which would allow them to be able to optimally care for their child once the child’s condition started deteriorating.
Being able to explain the child’s condition, or risk of developing it, to others (eg, insurance companies, care agencies, daycare, teachers, friends, acquaintances and relatives) to gain financial/social support was also expressed. Oftentimes parents said that the outside world did not always understand/empathize with their current situation.
Specifically with respect to UFs for carrier-status, parents sometimes stated that they wished to receive this information to be able to offer more pinpointed sexual and reproductive education and guidance/advice, as teenage pregnancy is possible.
Carrier-status of child and right to know of parent
One mother felt that if the child’s carrier-status was something inherited from the parents, it was information about themselves, which she and her partner had a right to know. This mother attributed causal responsibility to herself for the child’s carrier-status, and then took this causal responsibility to have the morally laden implication that information about the child’s carrier-status is information that belongs to her and her partner.
Relation to reasons for seeking a diagnosis
A portion of the parents pointed out that reasons for accepting various UFs should bear a relation to their reasons for seeking a diagnosis. For instance, parents explained that one reason for seeking a diagnosis via WES was to be able to visualize what the child’s future health might look like and that as UFs in various categories could also help them achieve this aim, those results should also be returned. For these parents, their reasons for seeking a diagnosis are what justified returning UFs in the various categories.
Groups of considerations favoring nondisclosure of UFs
Future autonomy
Some parents saw the future autonomy (ie, coming to possess the relevant capacities for making autonomous choices) of the child as a relevant consideration, which favored decline of UFs for all categories, except medically actionable conditions in childhood (and in some cases child-onset medically inactionable conditions, but not adult-onset medically inactionable conditions). Parents felt that decisions concerning these findings ought to be deferred to adulthood, if and when the child is able to decide for themselves. Parents added that this standpoint was only justified if obtaining results about UFs was possible later on.
Parents who put forth considerations of future autonomy, especially those of young children, were, however, sometimes uncertain about whether their child could develop into an autonomous adult, because of their age and/or current developmental delay, and this complicated determining what their preference was. Other parents of young children made no mention of this uncertainty and seemed to assume that their child could become autonomous, despite the fact that the indication for WES was developmental delay.
In contrast, some parents, especially those of older children with intellectual disability, were sure that their child would never become autonomous, even if they generally did take future autonomy to be a morally relevant consideration. That these parents saw future autonomy as a morally relevant consideration was evident in their reflection about the implications of WES results for their other children without intellectual disability, for example, whether return of UFs pertaining to the parents themselves could or would inhibit the possibilities for their other children of leading a life of their own choosing.
Negative emotional impact
The possible negative emotional aspects of knowledge of UFs for parents, their child(ren) and their other relatives were also mentioned as reasons favoring decline, except for UFs regarding conditions medically actionable in childhood. Concrete examples included worrying or fearfully waiting until the condition manifests itself. Parents referred to character traits, such as insecurity or being a ‘thinker’ and taking numerous scenarios into account, sometimes experienced as a kind of informational overload, as making decisions about UFs particularly difficult for them. Parents often preferred not to receive UFs for medically inactionable conditions, because of the negative emotional impact this could have on the entire family. Some also felt that knowledge of such UFs may lead them to spoil their child because of a limited life expectancy.
Some parents felt that disclosure of UFs for carrier-status and medically inactionable conditions at present could cause highly charged emotional problems later on that they wanted to avoid, such as whether to share such information with the child (pending their level of cognitive development) and the effects that may have on the child’s reproductive choices.
Lack of immediate (medical) action
For UFs regarding conditions only medically actionable in adulthood and carrier-status, some parents stated that because the information was not immediately (medically) actionable, and could be disclosed at a later point in time, it was not relevant to know now.
Insurance ineligibility
Insurance and mortgage ineligibility were reasons favoring nondisclosure of UFs for medically inactionable conditions and conditions only medically actionable in adulthood at present.
Doubtful of/deny non-medical utility
Non-medical utility claims, for example, life planning and preparation, were sometimes explicitly denied/doubted by parents, leading them to favor decline of UFs for carrier-status and medically inactionable conditions. These parents questioned whether they would actually change the way they lead their lives or make certain preparations.
No relation to reasons for seeking a diagnosis
As mentioned previously, some parents thought that reasons for accepting UFs should overlap with the kinds of reasons they had for seeking a diagnosis via WES. If this relation was not present, parents thought that UFs should not be disclosed. Some parents argued that results for carrier-status did not have any relation to their reasons for seeking a diagnosis, as reproductive matters were irrelevant to the child’s future health.
Discussion
Parents preferred to receive UFs concerning medically actionable conditions in childhood, but preferences and considerations diverged for UFs with no medical actionability, or medical actionability only in adulthood, and for carrier-status. Some parents preferred not to receive certain findings in the latter categories at present because of considerations of the child’s future autonomy – consistent with findings elsewhere.19 Other considerations for foregoing UFs, which have also been touched on in previous research included negative emotional impact; insurance ineligibility; lack of immediate (medical) action; and doubts/denial of non-medical utility claims.16, 20, 21, 22, 23, 24, 25
In contrast, other parents did not view the child’s autonomy as supporting decline of certain UFs at present, even if they thought their child would become autonomous. Instead, they favored disclosure of UFs due to considerations of non-medical utility (or for (possible) future medically actionability). Previous studies have also identified this type of reasoning.16, 19, 20, 21, 22, 23, 24, 25
Our findings provide important information about what parents regard as ethically justified reasons for disclosing/withholding UFs. Below we discuss how various key findings from our study are essential for morally responsible policy development and counseling.
First, some parents did not view future autonomy as a relevant consideration in their reasoning for UFs for carrier-status, conditions only medically actionable in adulthood and adult-onset medically inactionable conditions, even if it eventually would turn out that their child could develop the capacities for autonomous decision-making. Instead, they offered considerations of non-medical utility. This conflicts with some present and past policy recommendations,9, 11, 12 as well as some ethical views.7, 14 Parents in our study mentioned that considerations of non-medical utility can be focused on the child, other children in the family, the parents, other relatives or a combination of these persons. This suggests, as Christenhusz et al23 have identified in their qualitative study, that parents sometimes adopt what they call a ‘family-wide view’ of (non)disclosure, in which non-medical (and medical) benefits to relatives are seen as warranting return of UFs in some cases, while in others the negative impact on relatives is sometimes seen as warranting nondisclosure.23 The contention is, at least in some of these cases, that the non-medical benefits or harms go in both directions: if the family can be harmed or benefited by returning/withholding a UF, then this benefit/harm will accrue (even if only indirectly) to the child; and, conversely, what is beneficial or harmful for the child will also be beneficial or harmful to the family. However, cases are fathomable in which it is unlikely or doubtful that the child will benefit in the end, even if the parents do experience benefits from knowledge of the UF. For example, parents may want to know UFs for medically inactionable conditions to make the most of their time left with the child, but in the end this may only lead to spoiling the child. Such claims should thus be subject to further scrutiny.
Furthermore, even apart from questions of whether the child could benefit from what the parents see as beneficial, parents who offered considerations of non-medical utility sometimes also immediately questioned these claims and were sometimes skeptical about whether they would actually make certain changes to the way they lead their lives. Considerations of non-medical utility need to be the focus of both further empirical and ethical research, to determine whether they are justifiable reasons for disclosure or not. Further ethical research should focus on what the freedoms are of parents and professionals and what UFs need to be returned or withheld in order for parents and professionals to fulfill their responsibilities toward children under their care.
A second key finding was that some parents who viewed considerations of the child’s future autonomy as a reason to decline UFs (except those with medical actionability in childhood) based their reasoning on the presumption that their child would become autonomous, even though this was questionable because of their current developmental delay. It is possible, although this is a speculation and requires further research, that parents wish to maintain hope of a better future for their child.26, 27 This finding is relevant for counseling and policy development on return of results and recontact procedures, as it is conceivable that parents may have made different disclosure decisions, for example, to accept return of UFs for conditions only medically actionable in adulthood, if they were aware of the possibility that their child may remain incompetent. Further empirical research should focus on how parents can be aided in contemplating different types of scenarios regarding their child’s level of future development. This should form part of the informed consent process, and is especially important at centers in which policy allows parents to decide what UFs to accept or decline.
Third, another key finding was that a portion of parents only wished to receive UFs if reasons for having them returned bore a direct relation to the reasons underlying their search for a diagnosis via WES. Thus, some parents saw this relation as a further condition/constraint on what UFs may be returned or withheld, particularly where considerations of non-medical utility were concerned. This finding points to the pivotal role of genetic counseling for ensuring that one’s expectations and hopes for WES results are in line with possible WES outcomes, including cases in which no diagnosis is reached, with or without UFs. Further ethical research should focus on whether this type of reasoning could justify (non)disclosure of certain UFs.
Limitations
Our study has several limitations. First, parents were not interviewed who for whatever reason eventually decided to forego WES for their child. Yet, interviewing these parents may reveal considerations against the use of WES or against receiving certain UFs that are relevant for developing informed decision-making procedures. Second, our study did not include respondents from important minority groups in the Netherlands, for example, persons from Moroccan/Turkish descent, as they are underrepresented in genetic clinics. Third, our research focused on considerations of parents of incompetent children who had a developmental delay. Research on persons’ reasoning from other ethnic backgrounds and in cases of children capable of participating in decision-making may reveal new reasoning.
Conclusions
The findings of this study form some of the first insights on what kinds of considerations favor acceptance or decline of UFs for one’s child as well as difficulties encountered in decision-making for parents faced with choices regarding UFs from WES. Considerations of non-medical utility should be the focus of further ethical research, to determine whether they are justifiable reasons for disclosure or not. Moreover, for young children and/or those with a developmental delay, the possibility that the child may not develop competence deserves attention in policy and counseling; further research should focus on how parents can be aided in considering different scenarios regarding their child’s development and the various implications for disclosure choices. Subsequent ethical inquiry should also analyze whether a relation is required between one’s reasons for seeking a diagnosis via WES and considerations for acceptance of (certain) UFs.
References
Bamshad MJ, Ng SB, Bigham AW et al: Exome sequencing as a tool for Mendelian disease gene discovery. Nat Rev Genet 2011; 12: 745–755.
Johnston JJ, Rubinstein WS, Facio FM et al: Secondary variants in individuals undergoing exome sequencing: Screening of 572 individuals identifies high-penetrance mutations in cancer-susceptibility genes. Am J Hum Genet 2012; 91: 97–108.
Bredenoord AL, Onland‐Moret NC, Van Delden JJ : Feedback of individual genetic results to research participants: in favor of a qualified disclosure policy. Hum Mutat 2011; 32: 861–867.
Berg JS, Khoury MJ, Evans JP : Deploying whole genome sequencing in clinical practice and public health: meeting the challenge one bin at a time. Genet in Med 2011; 13: 499–504.
Dondorp W, Sikkema‐Raddatz B, de Die‐Smulders C, de Wert G : Arrays in postnatal and prenatal diagnosis: an exploration of the ethics of consent. Hum Mutat 2012; 33: 916–922.
Abdul-Karim R, Berkman BE, Wendler D et al: Disclosure of incidental findings from next-generation sequencing in pediatric genomic research. Pediatrics 2013; 131: 564–571.
Bredenoord AL, de Vries MC, van Delden JJ : Next-generation sequencing: does the next generation still have a right to an open future? Nat Rev Genet 2013; 14: 306–306.
Feinberg J. The child's right to an open future; in Aiken W, LaFollette W (eds): Whose Child? Children's Rights, Parental Authority, and State Power. Totowa, NJ, USA: Littlefield, Adams & Co.,, 1980, pp 124–153.
Sénécal K, Rahimzadeh V, Knoppers BM, Fernandez CV, Avard D, Sinnett D : Statement of principles on the return of research results and incidental findings in paediatric research: a multi-site consultative process 1. Genome 2015; 58: 541–548.
Borry P, Evers-Kiebooms G, Cornel MC, Clarke A, Dierickx K : Genetic testing in asymptomatic minors: background considerations towards ESHG Recommendations. Eur J Hum Genet 2009; 17: 711–719.
European Society of Human Genetics: Genetic testing in asymptomatic minors: recommendations of the European Society of Human Genetics. Eur J Hum Genet 2009; 17: 720.
American Association of Pediatrics: Ethical issues with genetic testing in pediatrics. Committee on Bioethics. Pediatrics 2001; 107: 1451–1455.
Green RC, Berg JS, Grody WW et al: ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet Med 2013; 15: 565–574.
Bredenoord AL, De Vries MC, van Delden H : The right to an open future concerning genetic information. Am J Bioethics 2014; 14: 21–23.
Rigter T, Van Aart C, Elting M, Waisfisz Q, Cornel M, Henneman L : Informed consent for exome sequencing in diagnostics: exploring first experiences and views of professionals and patients. Clin Genet 2014; 85: 417–422.
Clift KE, Halverson CM, Fiksdal AS, Kumbamu A, Sharp RR, McCormick JB : Patients' views on incidental findings from clinical exome sequencing. Appl Transl Genomics 2015; 4: 38–43.
Shahmirzadi L, Chao EC, Palmaer E, Parra MC, Tang S, Gonzalez KDF : Patient decisions for disclosure of secondary findings among the first 200 individuals undergoing clinical diagnostic exome sequencing. Genet Med 2013; 16: 395–399.
Vrijenhoek T, Kraaijeveld K, Elferink M et al: Next-generation sequencing-based genome diagnostics across clinical genetics centers: implementation choices and their effects. Eur J Hum Genet 2015; 23: 1142–1150.
Sapp JC, Dong D, Stark C et al: Parental attitudes, values, and beliefs toward the return of results from exome sequencing in children. Clin Genet 2014; 85: 120–126.
Townsend A, Adam S, Birch PH, Lohn Z, Rousseau F, Friedman JM : ‘I want to know what's in Pandora's box’: comparing stakeholder perspectives on incidental findings in clinical whole genomic sequencing. Am J Med Genet A 2012; 158: 2519–2525.
Levenseller BL, Soucier DJ, Miller VA, Harris D, Conway L, Bernhardt BA : Stakeholders’ opinions on the implementation of pediatric whole exome sequencing: implications for informed consent. J Genet Couns 2014; 23: 552–565.
Christenhusz GM, Devriendt K, Peeters H, Van Esch H, Dierickx K : The communication of secondary variants: interviews with parents whose children have undergone array‐CGH testing. Clin Genet 2014; 86: 207–216.
Christenhusz GM, Devriendt K, Van Esch H, Dierickx K : Focus group discussions on secondary variants and next-generation sequencing technologies. Eur J Med Genet 2015; 58: 249–257.
Kleiderman E, Knoppers BM, Fernandez CV et al: Returning incidental findings from genetic research to children: views of parents of children affected by rare diseases. J Med Genet 2014; 40: 691–696.
Driessnack M, Daack-Hirsch S, Downing N et al: The disclosure of incidental genomic findings: an 'ethically important moment' in pediatric research and practice. J Community Genet 2013; 4: 435–444.
Truitt M, Biesecker B, Capone G, Bailey T, Erby L : The role of hope in adaptation to uncertainty: the experience of caregivers of children with Down syndrome. Patient Educ Couns 2012; 87: 233–238.
Landsman G : Emplotting children's lives: Developmental delay vs. disability. Soc Sci Med 2003; 56: 1947–1960.
Acknowledgements
This research was funded by ZonMw – the Netherlands Organization for Health Research and Development (Grant No. 70-73000-98-047).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on European Journal of Human Genetics website
Supplementary information
Rights and permissions
About this article

Cite this article
Cornelis, C., Tibben, A., Dondorp, W. et al. Whole-exome sequencing in pediatrics: parents’ considerations toward return of unsolicited findings for their child. Eur J Hum Genet 24, 1681–1687 (2016). https://doi.org/10.1038/ejhg.2016.100
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejhg.2016.100
This article is cited by
-
Uncertain futures and unsolicited findings in pediatric genomic sequencing: guidelines for return of results in cases of developmental delay
BMC Medical Ethics (2023)
-
Should we respect parents’ views about which results to return from genomic sequencing?
Human Genetics (2022)
-
Parents, their children, whole exome sequencing and unsolicited findings: growing towards the child’s future autonomy
European Journal of Human Genetics (2021)
-
‘We Should View Him as an Individual’: The Role of the Child’s Future Autonomy in Shared Decision-Making About Unsolicited Findings in Pediatric Exome Sequencing
Health Care Analysis (2021)
-
The psychosocial and service delivery impact of genomic testing for inherited retinal dystrophies
Journal of Community Genetics (2019)
