
Abstract
It remains unclear whether lowering the blood pressure effectively prevents cognitive impairment. The aim of the current study was to explore the association between the prevalence, treatment and control of hypertension and the risk of mild cognitive impairment (MCI) among elderly Chinese people. This is a cross-sectional study conducted in Beijing, China. A two-stage stratified clustering sampling method was used, and 2065 participants, aged ⩾60 years, were included in the analysis. The Mini-Mental State Examination was used to assess participants’ cognitive function. The prevalence of MCI was higher in hypertensive (16.5%) than in normotensive individuals (13.1%; P=0.043). Furthermore, in those hypertensive patients, the prevalence of MCI was lower in those treated (14.9%) than in those not treated (19.9%; P=0.019) and lower in those controlled (13.4%) than in those uncontrolled (17.9%; P=0.042). The adjusted odds ratio (OR; 95% confidence interval (CI)) of having MCI was 1.59 (1.07–2.35) in those with hypertension compared with those normotensive individuals. The assessment of the hypertensive patients revealed the adjusted OR (95% CI) of having MCI in those with treated hypertension was 0.60 (0.42–0.86) compared with those untreated hypertension, and in those with controlled hypertension was 0.64 (0.43–0.93) compared with those non-controlled hypertension (regardless of treatment). However, among the treated hypertensive patients, there was no difference in the prevalence of MCI between the patients who reached and those who did not reach their treatment goal. We suggest that improved diagnoses and optimal therapeutics are needed to achieve the aim of cognitive decline prevention.
Similar content being viewed by others
Introduction
With the anticipated increase in the elderly population, a higher prevalence of hypertension is emerging. Hypertension affected 66.9% of elderly Chinese people in 2010.1 As a result, the treatment and control of hypertension are both considered important public health issues in preventing the traditional risk factors for stroke, cardiovascular events and heart failure.2
In recent years, accumulating epidemiologic and mechanistic evidence has shown that hypertension is also an important risk factor for dementia, Alzheimer’s disease and mild cognitive impairment (MCI).3, 4, 5, 6, 7 However, several authors did not observe such a relationship, and most of the negative associations involved the elderly population.8, 9 One reason for these negative associations is a potential survival bias related to blood pressure reduction.10, 11 In addition, different participant exclusion criteria, definitions of hypertension and cognitive function measurement tools might account for the conflicting relationship between blood pressure and cognitive function.12 A recent meta-analysis failed to demonstrate that antihypertensive treatment is associated with a reduction in cognitive decline.13 To the best of our knowledge, it remains unclear whether lowering blood pressure is effective for preventing cognitive impairment.14, 15
By 2050, adults over 60 years of age will constitute 29.7% of the total Chinese population.16 With the increasing aging population, China is facing serious challenges in terms of the medical demand for cognitive disorders and other chronic diseases.17 Evidence has demonstrated that individuals with MCI are at a higher risk of progressing to dementia, particularly in the elderly population.18 The prevalence of dementia has been rapidly increasing over the past few decades in China.19 Therefore, it is urgent to identify the population at a higher risk of MCI. Moreover, an optimal treatment approach must be developed to prevent the expected social and disease burden. The current study aims to examine the association between the prevalence, treatment and control of hypertension and the increased risk of MCI in participants over 60 years of age in an urban area in Beijing, China.
Methods
Study design
The sampling method was described in our previous study.20 In brief, we conducted a two-stage stratified clustering sampling method and included all participants who were aged ⩾60 years old in the Wanshoulu Community. First, we randomly selected 9 of the 94 communities in the Wanshoulu District. Second, we selected all the households (only one elderly resident from each household was recruited) with elderly residents from these 9 communities. Between September 2009 and June 2010, a total of 2162 of the 2510 elderly subjects completed the survey, resulting in a response rate of 86.1%. After excluding 97 adults with incomplete data, a total of 2065 subjects (839 males and 1226 females) were included in the current survey.
The Independent Ethics Committee of the Chinese People’s Liberation Army General Hospital (No. EC0411-2001) approved the current study. Signed informed consent was obtained from all of the eligible participants.
Data collection and measurement
Each participant completed a standardized questionnaire through a face-to-face interview. Data were collected on the participants’ demographic characteristics, medical histories and lifestyles. Trained observers measured the body height, weight, waist circumference and blood pressure of each participant according to the standardized protocol. While participants were in the standing position, their waist circumference was measured midway between the lower rib margin and the iliac crest. The body height was measured in meters while participants were not wearing shoes. The body weight was measured after participants removed heavy clothing, and 1 kg was deducted for the remaining garments. The body mass index was calculated as weight in kilograms divided by height in meters squared. After an overnight fasting, blood specimens were obtained for the measurements of serum lipids and glucose. Each participant’s specimens were sent to the central certified laboratory of the Chinese People’s Liberation Army General Hospital in fewer than 30 min.
Definition of MCI
Trained neurologists evaluated each participant’s cognitive function with the Mini-Mental State Examination (MMSE), which is a commonly used measurement worldwide.21 MCI was defined as an MMSE score <17 for illiterate subjects, <20 for subjects with 1–6 years of education and <24 for subjects with ⩾7 years of education. These MMSE score cutoff points demonstrated high efficiency in diagnosing MCI among the elderly population in China.22, 23
BP measurement and definitions
Before the survey, each participant was asked to avoid drinking alcohol, smoking cigarettes and drinking coffee or tea. Each participant’s blood pressure records were obtained from 0700 to 0800 hours. Using standardized mercury sphygmomanometers, we obtained the blood pressure records from the right arm of each participant while he/she was in a sitting position. Both diastolic blood pressure and systolic blood pressure were measured twice with a resting interval between the two measurements. The mean of the two readings was calculated to record each participant’s blood pressure value. If the two measurements differed by more than 10 mm Hg, the participant’s blood pressure was measured a third time, and the average of the three measurements was calculated as the final measurement. Trained observers calculated the average of the three records as the final measurement.
Hypertension was defined as systolic blood pressure ⩾140 mm Hg and/or diastolic blood pressure ⩾90 mm Hg and/or the self-reported use of antihypertensive medication.24 Among the hypertensive patients in the review, hypertension treatment was defined as the use of prescribed antihypertensive drugs in the previous 2 weeks. Control of hypertension was defined as pharmacological treatment of hypertension associated with an average systolic blood pressure <140 mm Hg and an average diastolic blood pressure <90 mm Hg.25
Statistical analysis
The data were double entered using Epidata (3.1). SPSS (SPSS Inc., Chicago, IL, USA) for Windows (19.0) was used for the data analysis. A two-sided P<0.05 was defined as statistical significance.
The baseline characteristics were described using descriptive statistics, and the t-test and χ2-test were used to assess differences in the continuous and categorical variables, respectively, unless otherwise specified. The relationship between the prevalence, treatment and control of hypertension and the MMSE score (continuous variable) was examined using a multivariable linear regression model. Logistic regression was used to calculate the unadjusted and adjusted odds ratios (ORs) and the 95% confidence intervals (95% CIs) of the prevalence, treatment and control of hypertension, and the prevalence of MCI. The participants who had cerebrovascular diseases or were <65 years of age were excluded from the sensitivity analysis.
Results
Description of the population
The baseline characteristics of the participants are shown in Table 1. The data for a total of 2065 (839 males and 1226 females) participants were included in the analysis. The mean age of the participants was 71.7±6.6 years, with a range from 60 to 95 years. The male participants were significantly older, were taller and had greater weight, higher waist circumference, lower systolic blood pressure, higher diastolic blood pressure, lower total cholesterol, lower triglycerides, lower high-density lipoprotein-cholesterol, lower low-density lipoprotein-cholesterol and higher MMSE scores than the female participants. The proportions of male participants who were better educated, married, normotensive and currently drinking and smoking were significantly higher than those of the female participants.
Overall, the mean MMSE score was 27.0±3.6, and the prevalences of MCI and hypertension were 15.4% and 68.2%, respectively. In the hypertensive patient population, the rates of hypertension treatment and control were 67.1% and 29.6%, respectively. A rate of hypertension control of 44.1% was achieved in the population of treated hypertensive patients. The prevalence of MCI showed little difference between males (16.0%) and females (15.1%). The prevalence of hypertension in female participants (70.8%) was significantly higher than that in male participants (64.4%). The analysis of the population of treated hypertensive patients revealed that the hypertension control rate in male participants (48.4%) was significantly higher than that achieved in female participants (41.6%). A higher proportion of females (68.9%) than males (64.3%) was treated as hypertensive patients, whereas more males (31.1%) than females (28.7%) were controlled hypertensive patients; however, the differences were not significant.
The association between hypertension and MMSE scores
Table 2 shows the unadjusted and adjusted association between the prevalence, treatment and control of hypertension and the MMSE score by gender. Overall, the prevalence of hypertension was negatively associated with the MMSE score, whereas the treatment and control of hypertension were associated with the MMSE score (all P<0.05). For the MMSE score (as a continuous variable), after adjusting for age, education level, marital status, physical activity, smoking and drinking status, body mass index, triglycerides, high-density lipoprotein, low-density lipoprotein, diabetes mellitus (yes/no), history of stroke and family history of dementia, the hypertensive patients had a significantly lower MMSE score (by 0.68) than the normotensives. The assessment of the population of hypertensive patients (n=1408) revealed that the treated hypertensive patients had a significantly higher MMSE score (by 0.85) than the untreated hypertensive patients. In the population of hypertensive patients (n=1408), the patients with controlled hypertension had a significantly higher MMSE score (by 0.52) compared with those non-controlled hypertension (regardless of treatment). There was no significant difference in the MMSE score between the hypertensive patients who received treatment for hypertension and achieved or did not achieve the treatment goal. Both male and female participants showed trends that were similar to those obtained in the main analyses.
The association between hypertension and MCI
Table 3 shows the unadjusted and adjusted associations between the prevalence, treatment and control of hypertension and the prevalence of MCI by gender. Overall, the prevalence of MCI was higher in hypertensive (16.5%) than in normotensive (13.1%; P=0.043) patients. Furthermore, in those hypertensive patients, the prevalence of MCI was lower in those treated (14.9%) than in those not treated (19.9%; P=0.019) and lower in those controlled (13.4%) than in those uncontrolled (17.9%; P=0.042). For the prevalence of MCI (as a dichotomous variable), after adjusting for age, education level, marital status, physical activity, smoking and drinking status, body mass index, triglycerides, high-density lipoprotein, low-density lipoprotein, diabetes mellitus (yes/no), history of stroke and family history of dementia, the OR (95% CI) of having MCI was 1.59 (1.07–2.35) in those with hypertension compared with those normotensive individuals. In the hypertensive patients (n=1408), the adjusted OR (95% CI) of having MCI in those with treated hypertension was 0.60 (0.42–0.86) compared with those with untreated hypertension, and in those with controlled hypertension was 0.64 (0.43–0.93) compared with those with non-controlled hypertension (regardless of treatment). However, the difference between the treated hypertensive patients who achieved and those who did not achieve their treatment goal was not significant. Both male and female participants showed trends that were similar to those obtained in the main analyses, but the differences were not significant in females.
Table 4 shows the unadjusted and adjusted associations between the prevalence, treatment and control of hypertension and the prevalence of MCI by age. Overall, participants in all age groups showed trends that were similar to those of the general population. In the 60–69 age group (n=748), the adjusted OR (95% CI) of having MCI was 1.90 (1.10–3.29) in those with hypertension compared with those normotensive individuals. In the population of hypertensive patients belonging to the 60–69 age group (n=424), the adjusted OR (95% CI) of having MCI in those with treated hypertension was 0.41 (0.23–0.71) compared with those with untreated hypertension, and in those with controlled hypertension was 0.53 (0.29–0.97) compared with those with non-controlled hypertension (regardless of treatment). However, among the treated hypertensive patients, there was no difference in the prevalence of MCI between the patients who reached and those who did not reach their treatment goal. In addition, the differences were not significant between the age groups of 70–79 years and ⩾80 years.
Sensitivity analysis
We assessed the relationship between the prevalence, treatment and control of hypertension and the prevalence of MCI in the sensitivity analysis (Appendix Tables 1 and 2). The results did not change after excluding the participants with cerebrovascular diseases (n=261, 12.6%) and the participants aged 60–64 years (n=358, 17.3%).
Discussion
The present study is a population-based, cross-sectional study with a strict training process and quality assurance programs. After adjusting for confounding variables, we found that the prevalence of hypertension was positively associated with the prevalence of MCI, whereas the treatment of hypertension was negatively related to the prevalence of MCI, particularly in males and the younger elderly population in an urban community in Beijing, China.
Previous studies on the cognitive consequences of hypertension among the elderly population have yielded inconsistent results. Both positive and negative relationships have been reported between hypertension and cognition decline. A cross-sectional study by Paran et al.26 reported that increasing blood pressure was related to a reduced risk of cognitive impairment in an elderly population aged 70–85 years. Guo et al. also found that lower blood pressure was associated with poor cognitive performance in participants aged 75–101 years. It should be noted that the the participants in the reports mentioned above was older than the participants in the present study. The possible biological mechanism linking blood pressure and cognitive decline has been explored by Skoog,27 who found that age-related changes in the brain might contribute to low blood pressure in very old people. In the present study, we did not find significant differences between hypertension and MCI in the 70–79 and ⩾80 age groups. However, for the 10.6% of the very elderly (⩾80 years) in the present study, we could not make an affirmative conclusion because of the limited sample size.
Nonetheless, the findings of the current study are in accordance with previous authors who have reported a positive relationship between hypertension and cognitive decline. Budge et al.28 reported that blood pressure was negatively related to the MMSE score in an elderly community. A cohort study of 13 476 African-American and white participants indicated that midlife hypertension was associated with more cognitive decline over the 20-year study period.29 Okusaga et al.4 reported that elevated blood pressure might be a risk factor for cognitive decline in a population-based cohort design. For the prevalence of MCI, both male and female participants showed trends that were similar to those of the general population, but the differences were not significant in females. To the best of our knowledge, no previous studies have separately studied men and women. Further prospective cohort studies with larger samples should be conducted to explore possible explanation for potential gender differences.
Whether lowering blood pressure aids in preventing dementia or cognitive decline in hypertensive patients is unclear.30 There have been reports that antihypertensive therapy has a protective effect on cognitive impairment, but other authors report an adverse result. In a meta-analysis, Chang-Quan et al.13 evaluated the association between antihypertensive medication use and the risk of cognitive decline but showed that antihypertensive treatment did not decrease the risk of cognitive decline. The conclusion of Chang-Quan et al. should be further improved because the data from randomized controlled trials and observational studies were pooled together. The findings of the current study were in line with some randomized controlled trials. Tzourio et al.31 confirmed the association between active treatment and the reduced risk of both dementia and cognitive decline, and the treatment group showed a 19% reduction of the risk of cognitive decline. Forette et al.32 reported that antihypertensive treatment was related to a 50% reduction in the incidence of dementia in an elderly population. A 4-year follow-up study by Tzourio et al.33 reported that untreated hypertensive participants displayed significantly worse cognitive performance on the MMSE than did normotensive and treated hypertensive participants. Spinelli et al.6 used various cognitive assessments scores, including MMSE scores, and reported that poorer blood pressure control was associated with impaired cognition among treated hypertensive subjects.
It is worth noting that the two ORs (ORs for the prevalence of MCI in treated hypertensive patients compared with all untreated hypertensive patients and in patients with controlled hypertensive compared with those with non-controlled hypertension regardless of treatment) obtained throughout the main analyses were similar. In addition, the differences in the MMSE score and the prevalence of MCI were not significant between treated hypertensive patients who reached and those who did not reach their treatment goal in the present study. The results suggest that treatment for hypertension by itself appears to exert a protective effect against MCI, but the results show that the aims of controlled and uncontrolled hypertension have almost no impact on the prevalence of MCI. Admittedly, the present study was limited by its small sample size; thus, a larger sample size is required to detect the association between hypertension control and the prevalence of MCI among treated hypertensive patients in future research.
Furthermore, numerous complex factors may be involved in the evaluation of higher blood pressure and poorer cognitive performance. Long-term hypertension might be associated with brain white matter diseases, resulting in cognitive impairment.34, 35 In addition, brain tissue loss might occur as a result of stroke, which is associated with cognitive impairment. As the most important risk factor for stroke, hypertension substantially increases the risk of cognitive impairment.36 Kobayashi et al.37 found that diastolic blood pressure is an independent risk factor affecting the extent of decreased regional cerebral blood flow and is considered an indicator of cognitive impairment.38 In general, hypertension does not exist alone; it is always accompanied by other risk factors, such as metabolic risks39, 40 or stroke-related factors.41, 42 Future research should focus on the interaction of multiple risk factors with a longer follow-up period.
Admittedly, this study has some limitations. First, cross-sectional studies are limited in determining the direction of an association, as both the exposure and the outcome are simultaneously assessed. Second, the information (lifestyles and disease histories) about each participant was self-reported, which might result in recall bias. To avoid these issues, we asked all the participants to bring their certificate of disease diagnosis to the interview, if possible. Third, detailed information on the participants’ diets and types of antihypertensive drugs used was not collected; such factors might be important covariates in the analysis of the study. Fourth, the association between hypertension and cognitive function is multifactorial, and the elderly population often has many risk factors, such as atherosclerosis, cardiovascular disease and diabetes mellitus. Although we have adjusted the potential confounding variables in the analysis, other undetected covariates might affect the results of the current study. Fifth, hypertensive patients who exhibit mild cognitive impairment may experience difficulty in going to a clinic/hospital and/or taking antihypertensive medication. This possible issue may have had a critical influence on the cross-sectional relationship of interest. Sixth, misclassification bias may exist in the present study. Some of the treated hypertensive patients may have not taken antihypertensive medication in the morning of the day of the study because the study participants were asked to undergo this examination without having eaten breakfast that day. This may have led to the misclassification of some of the patients with controlled hypertension as patients with uncontrolled hypertension due to an increase in blood pressure on the day of study. Finally, the Wanshoulu Community is a metropolitan area that is representative of the geographic and economic characteristics of Beijing, but the results are likely difficult to generalize to other areas in China. Further prospective studies with larger sample sizes are required to examine the association between the prevalence, awareness and treatment of hypertension and cognitive performance in the elderly population in China.
Conclusions
In conclusion, the present study showed a positive relationship between the prevalence of hypertension, untreated hypertension and an increased risk of cognitive impairment, particularly in males and the younger elderly population in an urban community of Beijing. The question of whether treatment for hypertension reached or did not reach the treatment goal to have an impact on the prevalence of MCI is an important topic to be addressed with a larger sample size in future research. Our findings suggest that improved diagnoses and optimal therapeutics are needed to achieve the target of cognitive decline prevention in the elderly population.
References
Wang ZH, Wang LH, Li YC, Zhang M, Hu N, Wang LM . Current status of diabetes, hypertension and dyslipidemia among older Chinese adults in 2010. Chin J Prev Med 2012; 46: 922–926.
Bromfield SG, Bowling CB, Tanner RM, Peralta CA, Odden MC, Oparil, Muntner P . Trends in hypertension prevalence, awareness, treatment, and control among US adults 80 years and older, 1988-2010. J Clin Hypertens (Greenwich) 2014; 16: 270–276.
Gorelick PB, Scuteri A, Black SE, Decarli C, Greenberg SM, Iadecola C, Launer LJ, Laurent S, Lopez OL, Nyenhuis D, Petersen RC, Schneider JA, Tzourio C, Arnett DK, Bennett DA, Chui HC, Higashida RT, Lindquist R, Nilsson PM, Roman GC, Sellke FW, Seshadri S, American Heart Association Stroke Council, Council on Epidemiology and Prevention, Council on Cardiovascular Nursing, Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011; 42: 2672–2713.
Okusaga O, Stewart MC, Butcher I, Deary I, Fowkes FG, Price JF . Smoking, hypercholesterolaemia and hypertension as risk factors for cognitive impairment in older adults. Age Ageing 2013; 42: 306–311.
Uiterwijk R, Huijts M, Staals J, Duits A, Gronenschild E, Kroon AA, de Leeuw PW, van Oostenbrugge RJ . Subjective cognitive failures in patients with hypertension are related to cognitive performance and cerebral micro bleeds. Hypertension 2014; 64: 653–657.
Spinelli C, De Caro MF, Schirosi G, Mezzapesa D, De Benedittis L, Chiapparino C, Serio G, Federico F, Nazzaro P . Impaired cognitive executive dysfunction in adult treated hypertensives with a confirmed diagnosis of poorly controlled blood pressure. Int J Med Sci 2014; 11: 771–778.
Yamaguchi Y, Wada M, Sato H, Nagasawa H, Koyama S, Takahashi Y, Kawanami T, Kato T . Impact of nocturnal heart rate variability on cerebral small-vessel disease progression: a longitudinal study in community-dwelling elderly Japanese. Hypertens Res 2015; 38: 564–569.
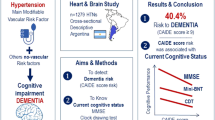
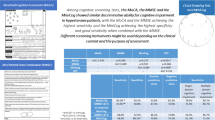
Abete P, Della-Morte D, Gargiulo G, Basile C, Langellotto A, Galizia G, Testa G, Canonico V, Bonaduce D, Cacciatore F . Cognitive impairment and cardiovascular diseases in the elderly. A heart-brain continuum hypothesis. Ageing Res Rev 2014; 18: 41–52.
Barnes DE, Yaffe K . The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol 2011; 10: 819–822.
Pullicino PM, Wadley VG, McClure LA, Safford MM, Lazar RM, Klapholz M, Ahmed A, Howard VJ, Howard G . Factors contributing to global cognitive impairment in heart failure: results from a population-based cohort. J Card Fail 2008; 14: 290–295.
Stewart R, Richards M, Brayne C, Mann A . Vascular risk and cognitive impairment in an older, British, African-Caribbean population. J Am Geriatr Soc 2011; 49: 263–269.
Birns J, Kalra L . Cognitive function and hypertension. J Hum Hypertens 2009; 23: 86–96.
Chang-Quan H, Hui W, Chao-Min W, Zheng-Rong W, Jun-Wen G, Yong-Hong L, Yan-You L, Qing-Xiu L . The association of antihypertensive medication use with risk of cognitive decline and denmentia: a meta-analysis of longitudinal studies. Int J Clin Pract 2011; 65: 1295–1305.
Debette S . Vascular risk factors and cognitive disorders. Rev Neurol (Paris) 2013; 169: 757–764.
Gorelick PB, Nyenhuis D. American Society of Hypertension Writing Group. Blood pressure and treatment of persons with hypertension as it relates to cognitive outcomes including executive function. J Am Soc Hypertens 2012; 6: 309–315.
Population division of the department of economic and social affairs of the United Nations secretariat, World Population Prospects The 2010 revision [on-line]. Available at http://esa.un.org/unpd/wpp/unpp/panel_population.htm Accessed 10 March 2013.
Parekh AK, Goodman RA, Gordon C, Koh HK HHS Interagency Workgroup on Multiple Chronic Conditions. Managing multiple chronic conditions: a strategic framework for improving health outcomes and quality of life. Public Health Rep 2011; 126: 460–471.
Fleisher AS, Sowell BB, Taylor C, Gamst AC, Petersen RC, Thal LJ . Alzheimer’s Disease Cooperative Study. Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment. Neurology 2007; 68: 1588–1595.
Chan KY, Wang W, Wu JJ, Liu L, Theodoratou E, Car J, Middleton L, Russ TC, Deary IJ, Campbell H, Wang W, Rudan I, Global Health Epidemiology Reference Group (GHERG). Epidemiology of Alzheimer’s disease and other forms of dementia in China, 1990-2010: a systematic review and analysis. Lancet 2013; 381: 2016–2023.
Liu M, He Y, Jiang B, Wu L, Yang S, Wang Y, Li X . Association between serum uric acid level and metabolic syndrome and its sex difference in a Chinese community elderly population. Int J Endocrinol 2014; 2014: 754678.
Folstein MF, Folstein SE, McHugh PR . “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189–198.
Peng D, Xu X, Liu J, Jiao Y, Zhuang H . Discussion on application of mmse for senile dementia patients. Chinese J Neuroimmunol Neurol 2005; 4: 187–190.
Liu M, He Y, Jiang B, Wu L, Wang J, Yang S, Wang Y . Association between metabolic syndrome and mild cognitive impairment and its age difference in a Chinese community elderly population. Clin Endocrinol (Oxf) 2015; 82: 844–853.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr . Seventh report of joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003; 42: 1206–1252.
Gu D, Reynolds K, Wu X, Chen J, Duan X, Muntner P, Huang G, Reynolds RF, Su S, Whelton PK, He J, InterASIA Collaborative Group. The International Collaborative Study of Cardiovascular Disease in ASIA. Prevalence, awareness, treatment, and control of hypertension in china. Hypertension 2002; 40: 920–927.
Paran E, Anson O, Reuveni H . Blood pressure and cognitive functioning among independent elderly. Am J Hypertens 2003; 16: 818–826.
Skoog I . A review on blood pressure and ischaemic white matter lesions. Dement Geriatr Cogn Disord 1998; 9: 13–19.
Budge MM, de Jager C, Hogervorst E, Smith AD Oxford Project To Investigate Memory and Ageing (OPTIMA). Total plasma homocysteine, age, systolic blood pressure, and cognitive performance in older people. J Am Geriatr Soc 2002; 50: 2014–2018.
Gottesman RF, Schneider AL, Albert M, Alonso A, Bandeen-Roche K, Coker L, Coresh J, Knopman D, Power MC, Rawlings A, Sharrett AR, Wruck LM, Mosley TH . Midlife hypertension and 20-year cognitive change: the atherosclerosis risk in communities neuro cognitive study. JAMA Neurol 2014; 71: 1218–1227.
McGuinness B, Todd S, Passmore P, Bullock R . The effects of blood pressure lowering on development of cognitive impairment and dementia in patients without apparent prior cerebrovascular disease. Cochrane Database Syst Rev 2006; 19: CD004034.
Tzourio C, Anderson C, Chapman N, Woodward M, Neal B, MacMahon S, Chalmers J, PROGRESS Collaborative Group. Effects of blood pressure lowering with perindopril and in dapamide therapy on dementia and cognitive decline in patients with cerebrovascular disease. Arch Intern Med 2003; 163: 1069–1075.
Forette F, Seux ML, Staessen JA, Thijs L, Babarskiene MR, Babeanu S, Bossini A, Fagard R, Gil-Extremera B, Laks T, Kobalava Z, Sarti C, Tuomilehto J, Vanhanen H, Webster J, Yodfat Y, Birkenhäger WH Systolic hypertension in Europe Investigators. The prevention of dementia with antihypertensive treatment: new evidence from the Systolic Hypertension in Europe (Syst-Eur) study. Arch Intern Med 2002; 162: 2046–2052.
Tzourio C, Dufouil C, Ducimetie`re P, Alpéovitch A . Cognitive decline in individuals with high blood pressure. Neurology 1999; 53: 1948–1952.
Pantoni L . Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 2010; 9: 689–701.
Hoffman LB, Schmeidler J, Lesser GT, Beeri MS, Purohit DP, Grossman HT, Haroutunian V . Less Alzheimer disease neuropathology in medicated hypertensive than nonhypertensive persons. Neurology 2009; 72: 1720–1726.
Gorelick PB . Status of risk factors for dementia associated with stroke. Stroke 1997; 28: 459–463.
Kobayashi S, Mochida Y, Ishioka K, Oka M, Maesato K, Moriya H, Hidaka S, Ohtake T . The effects of blood pressure and the renin-angiotensin-aldosterone system on regional cerebral blood flow and cognitive impairment in dialysis patients. Hypertens Res 2014; 37: 636–641.
Derejko M, Sławek J, Wieczorek D, Brockhuis B, Dubaniewicz M, Lass P . Regional cerebral blood flow in Parkinson’s disease as an indicator of cognitive impairment. Nucl Med Commun 2006; 27: 945–951.
Chang T, Lung F, Yen Y . Depressive symptoms, cognitive impairment, and metabolic syndrome in community-dwelling elderly in Southern Taiwan. Psychogeriatrics. 2015; 15: 109–115.
Magierski R, Kłoszewska I, Sobow T . Evaluation of the influence of metabolic processes and body composition on cognitive functions: Nutrition and Dementia Project (Nutr Dem Project). Eur J Clin Nutr 2014; 68: 1200–1203.
Huang Y, Yang S, Jia J . Factors related to long-term post-stroke cognitive impairment in young adult ischemic stroke. Med Sci Monit 2015; 21: 654–660.
Paran E, Anson O, Reuveni H . Blood pressure and cognitive functioning among independent elderly. Am J Hypertens 2003; 16: 818–826.
Acknowledgements
This study was supported by research grants from the National Natural Science Foundation of China (81373080), the Beijing Municipal Science and Technology Commission (D121100004912003) and the Military Medicine Innovation Fund (13CXZ029).
Author contributions
YH and BJ helped design the study and analyzed the data. BJ and JW helped with the data collection and field operations. All of the authors helped prepare the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Appendices
Appendix Table 1
Appendix Table 2
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Wu, L., He, Y., Jiang, B. et al. The association between the prevalence, treatment and control of hypertension and the risk of mild cognitive impairment in an elderly urban population in China. Hypertens Res 39, 367–375 (2016). https://doi.org/10.1038/hr.2015.146
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2015.146
Keywords
This article is cited by
-
Association between physical activity and falls among older adults in rural China: are there gender and age related differences?
BMC Public Health (2022)
-
Poor sleep quality is negatively associated with low cognitive performance in general population independent of self-reported sleep disordered breathing
BMC Public Health (2022)
-
Body mass index and mild cognitive impairment among rural older adults in China: the moderating roles of gender and age
BMC Psychiatry (2021)
-
Prevalence of mild cognitive impairment in community-dwelling Chinese populations aged over 55 years: a meta-analysis and systematic review
BMC Geriatrics (2021)
-
Socioeconomic and lifestyle determinants of the prevalence of hypertension among elderly individuals in rural southwest China: a structural equation modelling approach
BMC Cardiovascular Disorders (2021)
