
Key Points
-
Bariatric surgery provides substantial and durable weight loss, indicating that the gastrointestinal tract has key gut–brain signalling pathways that can alter control of central energy balance
-
Gastrointestinal devices assisting weight management can be placed endoscopically or laparoscopically, and aim at filling the safety and effectiveness therapeutic gap between lifestyle interventions and more invasive bariatric surgery
-
Laparoscopic adjustable gastric bands provide the largest amount of durable weight loss compared with other devices, and tailored, multidisciplinary aftercare programmes reduce explant rates and adverse outcomes
-
Intragastric balloon therapy is indicated in individuals with a BMI 30–40 kg/m2 for a maximum duration of 6 months; advances have enabled swallowable balloons not requiring endoscopic placement
-
Vagal blockade involves the surgical placement of a neuromodulator device with electrodes connected to the infradiaphragmatic vagal trunks, and achieves modest weight loss
-
A novel gastric emptying system that enables patients to aspirate gastric contents and ingested food via an endoscopically placed gastrostomy tube displays a promising benefit–risk profile
Abstract
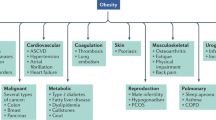
Obesity is a major public health concern that leads to numerous metabolic, mechanical and psychological complications. Although lifestyle interventions are the cornerstone of obesity management, subsequent physiological neurohormonal adaptations limit weight loss, strongly favour weight regain and counteract sustained weight loss. A range of effective therapies are therefore needed to manage this chronic relapsing disease. Bariatric surgery delivers substantial, durable weight loss but limited access to care, perceived high risks and costs restrict uptake. Medical devices are uniquely positioned to bridge the gap between more conservative lifestyle intervention and weight-loss pharmacotherapy and more disruptive bariatric surgery. In this Review, we examine the range of gastrointestinal medical devices that are available in clinical practice to treat obesity, as well as those that are in advanced stages of development. We focus on the mechanisms of action as well as the efficacy and safety profiles of these devices. Many of these devices are placed endoscopically, which provides gastroenterologists with exciting opportunities for treatment.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout






Similar content being viewed by others

References
World Health Organization. Global Health Observatory (GHO) data: overweight and obesity. WHO http://www.who.int/gho/ncd/risk_factors/overweight_text/en/ (2016).
Stevens, J., Oakkar, E. E., Cui, Z., Cai, J. & Truesdale, K. P. US adults recommended for weight reduction by 1998 and 2013 obesity guidelines, NHANES 2007–2012. Obesity (Silver Spring) 23, 527–531 (2015).
Apovian, C. M. et al. Best practice updates for multidisciplinary care in weight loss surgery. Obesity (Silver Spring) 17, 871–879 (2009).
Magkos, F. et al. Effects of moderate and subsequent progressive weight loss on metabolic function and adipose tissue biology in humans with obesity. Cell Metab. 23, 591–601 (2016).
Jensen, M. D. et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and The Obesity Society. Circulation 129, S102–S138 (2014).
Sumithran, P. et al. Long-term persistence of hormonal adaptations to weight loss. N. Engl. J. Med. 365, 1597–1604 (2011).
Rosenbaum, M., Hirsch, J., Gallagher, D. A. & Leibel, R. L. Long-term persistence of adaptive thermogenesis in subjects who have maintained a reduced body weight. Am. J. Clin. Nutr. 88, 906–912 (2008).
Apovian, C. M. et al. Pharmacological management of obesity: an Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 100, 342–362 (2015).
Apovian, C. M., Garvey, W. T. & Ryan, D. H. Challenging obesity: patient, provider, and expert perspectives on the roles of available and emerging nonsurgical therapies. Obesity (Silver Spring) 23 (Suppl. 2), S1–S26 (2015).
Angrisani, L. et al. Bariatric surgery worldwide 2013. Obes. Surg. 25, 1822–1832 (2015).
Afonso, B. B., Rosenthal, R., Li, K. M., Zapatier, J. & Szomstein, S. Perceived barriers to bariatric surgery among morbidly obese patients. Surg. Obes. Relat. Dis. 6, 16–21 (2010).
Wharton, S. et al. Interest, views and perceived barriers to bariatric surgery in patients with morbid obesity. Clin. Obes. 6, 154–160 (2016).
Hallberg, D. & Forsell, P. Ballongband vid behandling av massiv övervikt [Swedish]. Svensk Kirurgi. 43, 106 (1985).
Belachew, M. et al. Laparoscopic placement of adjustable silicone gastric band in the treatment of morbid obesity: how to do it. Obes. Surg. 5, 66–70 (1995).
DeMaria, E. J., Pate, V., Warthen, M. & Winegar, D. A. Baseline data from American Society for Metabolic and Bariatric Surgery-designated Bariatric Surgery Centers of Excellence using the Bariatric Outcomes Longitudinal Database. Surg. Obes. Relat. Dis. 6, 347–355 (2010).
Longitudinal Assessment of Bariatric Surgery Consortium et al. Perioperative safety in the longitudinal assessment of bariatric surgery. N. Engl. J. Med. 361, 445–454 (2009).
Dixon, A. F., Dixon, J. B. & O'Brien, P. E. Laparoscopic adjustable gastric banding induces prolonged satiety: a randomized blind crossover study. J. Clin. Endocrinol. Metab. 90, 813–819 (2005).
Burton, P. R. et al. Changes in satiety, supra- and infraband transit, and gastric emptying following laparoscopic adjustable gastric banding: a prospective follow-up study. Obes. Surg. 21, 217–223 (2011).
Dixon, J. B., Lambert, E. A. & Lambert, G. W. Neuroendocrine adaptations to bariatric surgery. Mol. Cell. Endocrinol. 418, 143–152 (2015).
Dixon, A. F. et al. Pancreatic polypeptide meal response may predict gastric band-induced weight loss. Obes. Surg. 21, 1906–1913 (2011).
Aneta Stefanidis, P. D. et al. An investigation of the neural mechanisms underlying the efficacy of the adjustable gastric band. Surg. Obes. Relat. Dis. 12, 828–838 (2016).
Dixon, J. B., Straznicky, N. E., Lambert, E. A., Schlaich, M. P. & Lambert, G. W. Laparoscopic adjustable gastric banding and other devices for the management of obesity. Circulation 126, 774–785 (2012).
O'Brien, P. E. et al. Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program: a randomized trial. Ann. Intern. Med. 144, 625–633 (2006).
Dixon, J. B. et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA 299, 316–323 (2008).
O'Brien, P. E. et al. Laparoscopic adjustable gastric banding in severely obese adolescents: a randomized trial. JAMA 303, 519–526 (2010).
O'Brien, P. E., MacDonald, L., Anderson, M., Brennan, L. & Brown, W. A. Long-term outcomes after bariatric surgery: fifteen-year follow-up of adjustable gastric banding and a systematic review of the bariatric surgical literature. Ann. Surg. 257, 87–94 (2013).
Rogers, C. A. et al. The By-Band study: gastric bypass or adjustable gastric band surgery to treat morbid obesity: study protocol for a multi-centre randomised controlled trial with an internal pilot phase. Trials 15, 53 (2014).
Dixon, J. B. & O'Brien, P. E. Changes in comorbidities and improvements in quality of life after LAP-BAND placement. Am. J. Surg. 184, 51S–54S (2002).
Chen, S. B. et al. Serum C-reactive protein and white blood cell count in morbidly obese surgical patients. Obes. Surg. 19, 461–466 (2009).
Buchwald, H. et al. Weight and type 2 diabetes after bariatric surgery: systematic review and meta-analysis. Am. J. Med. 122, 248–256.e5 (2009).
Busetto, L. et al. Comparative long-term mortality after laparoscopic adjustable gastric banding versus nonsurgical controls. Surg. Obes. Relat. Dis. 3, 496–502 (2007).
Peeters, A. et al. Substantial intentional weight loss and mortality in the severely obese. Ann. Surg. 246, 1028–1033 (2007).
Watkins, B. M. et al. Laparoscopic adjustable gastric banding in an ambulatory surgery center. Surg. Obes. Relat. Dis. 4, S56–S62 (2008).
Cobourn, C., Mumford, D., Chapman, M. A. & Wells, L. Laparoscopic gastric banding is safe in outpatient surgical centers. Obes. Surg. 20, 415–422 (2010).
Chapman, A. E. et al. Laparoscopic adjustable gastric banding in the treatment of obesity: a systematic literature review. Surgery 135, 326–351 (2004).
Buchwald, H., Estok, R., Fahrbach, K., Banel, D. & Sledge, I. Trends in mortality in bariatric surgery: a systematic review and meta-analysis. Surgery 142, 621–632 (2007).
Lancaster, R. T. & Hutter, M. M. Bands and bypasses: 30-day morbidity and mortality of bariatric surgical procedures as assessed by prospective, multi-center, risk-adjusted ACS-NSQIP data. Surg. Endosc. 22, 2554–2563 (2008).
Parikh, M. S., Laker, S., Weiner, M., Hajiseyedjavadi, O. & Ren, C. J. Objective comparison of complications resulting from laparoscopic bariatric procedures. J. Am. Coll. Surg. 202, 252–261 (2006).
Egberts, K., Brown, W. A. & O'Brien, P. E. Systematic review of erosion after laparoscopic adjustable gastric banding. Obes. Surg. 21, 1272–1279 (2011).
Dixon, J., Eaton, L., Cobourn, C. & Curry, T. A prospective, international, multi-center, non-randomized, open label study (HERO) of health outcomes and the rates of explants and reoperations after 5 years of treatment with laparoscopic adjustable gastric banding. Surg. Obes. Relat. Dis. 12, S79 (2016)
Khan, S. et al. Trends in bariatric surgery from 2008 to 2012. Am. J. Surg. 211, 1041–1046 (2016).
ASGE/ASMBS Task Force on Endoscopic Bariatric Therapy. A pathway to endoscopic bariatric therapies. Surg. Obes. Relat. Dis. 7, 672–682 (2011).
Nieben, O. G. & Harboe, H. Intragastric balloon as an artificial bezoar for treatment of obesity. Lancet 1, 198–199 (1982).
Kramer, F. M. et al. Limited weight losses with a gastric balloon. Arch. Intern. Med. 149, 411–413 (1989).
Schapiro, M. et al. Obesity and the gastric balloon: a comprehensive workshop. Tarpon Springs, Florida, March 19–21, 1987. Gastrointest. Endosc. 33, 323–327 (1987).
Galloro, G. et al. Preliminary endoscopic technical report of a new silicone intragastric balloon in the treatment of morbid obesity. Obes. Surg. 9, 68–71 (1999).
Genco, A. et al. BioEnterics intragastric balloon: the Italian experience with 2,515 Patients. Obes. Surg. 15, 1161–1164 (2005).
Roman, S. et al. Intragastric balloon for “non-morbid” obesity: a retrospective evaluation of tolerance and efficacy. Obes. Surg. 14, 539–544 (2004).
Sallet, J. A. et al. Brazilian multicenter study of the intragastric balloon. Obes. Surg. 14, 991–998 (2004).
Totte, E., Hendrickx, L., Pauwels, M. & Van Hee, R. Weight reduction by means of intragastric device: experience with the bioenterics intragastric balloon. Obes. Surg. 11, 519–523 (2001).
Imaz, I., Martinez-Cervell, C., Garcia-Alvarez, E. E., Sendra-Gutierrez, J. M. & Gonzalez-Enriquez, J. Safety and effectiveness of the intragastric balloon for obesity. A meta-analysis. Obes. Surg. 18, 841–846 (2008).
Courcoulas, A. et al. Intragastric balloon as an adjunct to lifestyle intervention: a randomized controlled trial. Int. J. Obes. (Lond.) 41, 427–433 (2017).
Ponce, J. et al. The REDUCE pivotal trial: a prospective, randomized controlled pivotal trial of a dual intragastric balloon for the treatment of obesity. Surg. Obes. Relat. Dis. 11, 874–881 (2015).
Mion, F. et al. Swallowable Obalon® gastric balloons as an aid for weight loss: a pilot feasibility study. Obes. Surg. 23, 730–733 (2013).
U.S. Food and Drug Administration. Summary of safety and effectiveness data: Obalon Balloon System — P160001. FDA http://www.accessdata.fda.gov/cdrh_docs/pdf16/P160001b.pdf (2016).
Machytka, E. et al. Elipse, a procedureless gastric balloon for weight loss: a proof-of-concept pilot study. Obes. Surg. 26, 512–516 (2016).
Marinos, G., Eliades, C., Raman Muthusamy, V. & Greenway, F. Weight loss and improved quality of life with a nonsurgical endoscopic treatment for obesity: clinical results from a 3- and 6-month study. Surg. Obes. Relat. Dis. 10, 929–934 (2014).
US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/NCT02518685 (2017).
Ritter, R. C. Gastrointestinal mechanisms of satiation for food. Physiol. Behav. 81, 249–273 (2004).
de Lartigue, G. Role of the vagus nerve in the development and treatment of diet-induced obesity. J. Physiol. 594, 5791–5815 (2016).
Berthoud, H. R. Vagal and hormonal gut-brain communication: from satiation to satisfaction. Neurogastroenterol. Motil. 20 (Suppl. 1), 64–72 (2008).
Mion, F. et al. Effects of intragastric balloon on gastric emptying and plasma ghrelin levels in non-morbid obese patients. Obes. Surg. 15, 510–516 (2005).
Martinez-Brocca, M. A. et al. Intragastric balloon-induced satiety is not mediated by modification in fasting or postprandial plasma ghrelin levels in morbid obesity. Obes. Surg. 17, 649–657 (2007).
Mathus-Vliegen, E. M. & Eichenberger, R. I. Fasting and meal-suppressed ghrelin levels before and after intragastric balloons and balloon-induced weight loss. Obes. Surg. 24, 85–94 (2014).
Konopko-Zubrzycka, M. et al. The effect of intragastric balloon on plasma ghrelin, leptin, and adiponectin levels in patients with morbid obesity. J. Clin. Endocrinol. Metab. 94, 1644–1649 (2009).
Mathus-Vliegen, E. M. & de Groot, G. H. Fasting and meal-induced CCK and PP secretion following intragastric balloon treatment for obesity. Obes. Surg. 23, 622–633 (2013).
Kumar, N. Endoscopic therapy for weight loss: gastroplasty, duodenal sleeves, intragastric balloons, and aspiration. World J. Gastrointest. Endosc. 7, 847–859 (2015).
Issa, I., Taha, A. & Azar, C. Acute pancreatitis caused by intragastric balloon: a case report. Obes. Res. Clin. Pract. 10, 340–343 (2016).
Mohammed, A. E. & Benmousa, A. Acute pancreatitis complicating intragastric balloon insertion. Case Rep. Gastroenterol. 2, 291–295 (2008).
U.S. Food and Drug Administration. The FDA alerts health care providers about potential risks with fluid-filled intragastric balloons. FDA http://www.fda.gov/MedicalDevices/ResourcesforYou/HealthCareProviders/ucm540655.htm (2017).
De Castro, M. L. et al. Efficacy, safety, and tolerance of two types of intragastric balloons placed in obese subjects: a double-blind comparative study. Obes. Surg. 20, 1642–1646 (2010).
Machytka, E. et al. Adjustable intragastric balloons: a 12-month pilot trial in endoscopic weight loss management. Obes. Surg. 21, 1499–1507 (2011).
Yap Kannan, R. & Nutt, M. R. Are intra-gastric adjustable balloon system safe? A case series. Int. J. Surg. Case Rep. 4, 936–938 (2013).
Dumonceau, J. M. Evidence-based review of the Bioenterics intragastric balloon for weight loss. Obes. Surg. 18, 1611–1617 (2008).
Genco, A. et al. BioEnterics Intragastric Balloon (BIB): a short-term, double-blind, randomised, controlled, crossover study on weight reduction in morbidly obese patients. Int. J. Obes. (Lond.) 30, 129–133 (2006).
Alfalah, H. et al. Intragastric balloon for preoperative weight reduction in candidates for laparoscopic gastric bypass with massive obesity. Obes. Surg. 16, 147–150 (2006).
Gottig, S., Weiner, R. A. & Daskalakis, M. Preoperative weight reduction using the intragastric balloon. Obes. Facts 2 (Suppl. 1), 20–23 (2009).
Frutos, M. D. et al. Intragastric balloon reduces liver volume in super-obese patients, facilitating subsequent laparoscopic gastric bypass. Obes. Surg. 17, 150–154 (2007).
Coffin, B. et al. Impact of intragastric balloon before laparoscopic gastric bypass on patients with super obesity: a randomized multicenter study. Obes. Surg. 27, 902–909 (2017).
Kral, J. G. & Gortz, L. Truncal vagotomy in morbid obesity. Int. J. Obes. 5, 431–435 (1981).
Kral, J. G. Surgical treatment of obesity. Med. Clin. North Am. 73, 251–264 (1989).
Lebovitz, H. E. Interventional treatment of obesity and diabetes: an interim report on gastric electrical stimulation. Rev. Endocr. Metab. Disord. 17, 73–80 (2016).
Camilleri, M. et al. Intra-abdominal vagal blocking (VBLOC therapy): clinical results with a new implantable medical device. Surgery 143, 723–731 (2008).
Ikramuddin, S. et al. Effect of reversible intermittent intra-abdominal vagal nerve blockade on morbid obesity: the ReCharge randomized clinical trial. JAMA 312, 915–922 (2014).
Shikora, S. A. et al. Sustained weight loss with vagal nerve blockade but not with sham: 18-month results of the ReCharge trial. J. Obes. 2015, 365604 (2015).
Apovian, C. M. et al. Two-year outcomes of vagal nerve blocking (vBloc) for the treatment of obesity in the ReCharge trial. Obes. Surg. 27, 169–176 (2017).
Shikora, S. A. et al. Implantable gastric stimulation for the treatment of clinically severe obesity: results of the SHAPE trial. Surg. Obes. Relat. Dis. 5, 31–37 (2009).
Lebovitz, H. E. et al. Fasting plasma triglycerides predict the glycaemic response to treatment of type 2 diabetes by gastric electrical stimulation. A novel lipotoxicity paradigm. Diabet. Med. 30, 687–693 (2013).
Lebovitz, H. E. et al. Treatment of patients with obese type 2 diabetes with tantalus-DIAMOND® gastric electrical stimulation: normal triglycerides predict durable effects for at least 3 years. Horm. Metab. Res. 47, 456–462 (2015).
Lebovitz, H. E. et al. Gastric electrical stimulation treatment of type 2 diabetes: effects of implantation versus meal-mediated stimulation. A randomized blinded cross-over trial. Physiol. Rep. 3, e12456 (2015).
Miras, M., Serrano, M., Duran, C., Valino, C. & Canton, S. Early experience with customized, meal-triggered gastric electrical stimulation in obese patients. Obes. Surg. 25, 174–179 (2015).
Horbach, T. et al. Abiliti closed-loop gastric electrical stimulation system for treatment of obesity: clinical results with a 27-month follow-up. Obes. Surg. 25, 1779–1787 (2015).
Horbach, T. et al. Closed-loop gastric electrical stimulation versus laparoscopic adjustable gastric band for the treatment of obesity: a randomized 12-month multicenter study. Int. J. Obes. (Lond.) 40, 1891–1898 (2016).
Pellegrini, C. A. et al. The comparison of a technology-based system and an in-person behavioral weight loss intervention. Obesity (Silver Spring) 20, 356–363 (2012).
Polzien, K. M., Jakicic, J. M., Tate, D. F. & Otto, A. D. The efficacy of a technology-based system in a short-term behavioral weight loss intervention. Obesity (Silver Spring) 15, 825–830 (2007).
Jakicic, J. M. et al. Effect of wearable technology combined with a lifestyle intervention on long-term weight loss: the IDEA randomized clinical trial. JAMA 316, 1161–1171 (2016).
Forssell, H. & Noren, E. A novel endoscopic weight loss therapy using gastric aspiration: results after 6 months. Endoscopy 47, 68–71 (2015).
Sullivan, S., Stein, R., Jonnalagadda, S., Mullady, D. & Edmundowicz, S. Aspiration therapy leads to weight loss in obese subjects: a pilot study. Gastroenterology 145, 1245–1252.e5 (2013).
Thompson, C. C. et al. Percutaneous gastrostomy device for the treatment of class II and class III obesity: results of a randomized controlled trial. Am. J. Gastroenterol. 112, 447–457 (2017).
U.S. Food and Drug Administration. Summary of safety and effectiveness data: AspireAssist®. FDA http://www.accessdata.fda.gov/cdrh_docs/pdf15/p150024b.pdf (2016).
Koehestanie, P. et al. The effect of the endoscopic duodenal-jejunal bypass liner on obesity and type 2 diabetes mellitus, a multicenter randomized controlled trial. Ann. Surg. 260, 984–992 (2014).
Kaplan, L. M. et al. Endobarrier therapy is associated with glycemic improvement, weight loss and safety issues in patients with obesity and type 2 diabetes on oral antihyperglycemic agents. Presented at the American Diabetes Association 76th Scientific Sessions, New Orleans, USA (2016)
Rohde, U., Hedback, N., Gluud, L. L., Vilsboll, T. & Knop, F. K. Effect of the EndoBarrier Gastrointestinal Liner on obesity and type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes. Metab. 18, 300–305 (2016).
Rubino, F. et al. The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes. Ann. Surg. 244, 741–749 (2006).
de Jonge, C. et al. Endoscopic duodenal-jejunal bypass liner rapidly improves type 2 diabetes. Obes. Surg. 23, 1354–1360 (2013).
Vilarrasa, N. et al. Endobarrier® in grade I obese patients with long-standing type 2 diabetes: role of gastrointestinal hormones in glucose metabolism. Obes. Surg. 27, 569–577 (2016).
Rohde, U. et al. The impact of EndoBarrier Gastrointestinal Liner in obese patients with normal glucose tolerance and patients with type 2 diabetes. Diabetes Obes. Metab. 19, 189–199 (2017).
de Moura, E. G. et al. Effects of duodenal-jejunal bypass liner (EndoBarrier®) on gastric emptying in obese and type 2 diabetic patients. Obes. Surg. 25, 1618–1625 (2015).
Betzel, B. et al. Safety experience with the duodenal-jejunal bypass liner: an endoscopic treatment for diabetes and obesity. Gastrointest. Endosc. 82, 845–852 (2015).
Zechmeister-Koss, I., Huic, M., Fischer, S. & European Network for Health Technology Assessment. The duodenal-jejunal bypass liner for the treatment of type 2 diabetes mellitus and/or obesity: a systematic review. Obes. Surg. 24, 310–323 (2014).
GI Dynamics. TGA cancellation of EndoBarrier listing. GI Dynamics http://gidynamics.com/2016/10/24/tga-cancellation-of-endobarrier-listing/ (2016).
Sandler, B. J. et al. Human experience with an endoluminal, endoscopic, gastrojejunal bypass sleeve. Surg. Endosc. 25, 3028–3033 (2011).
Sandler, B. J. et al. One-year human experience with a novel endoluminal, endoscopic gastric bypass sleeve for morbid obesity. Surg. Endosc. 29, 3298–3303 (2015).
Neylan, C. J., Dempsey, D. T., Tewksbury, C. M., Williams, N. N. & Dumon, K. R. Endoscopic treatments of obesity: a comprehensive review. Surg. Obes. Relat. Dis. 12, 1108–1115 (2016).
Rajagopalan, H. et al. Endoscopic duodenal mucosal resurfacing for the treatment of type 2 diabetes: 6-month interim analysis from the first-in-human proof-of-concept study. Diabetes Care 39, 2254–2261 (2016).
Dargent, J. Novel endoscopic management of obesity. Clin. Endosc. 49, 30–36 (2016).
Kipshidze, N., Archvadze, A., Bertog, S., Leon, M. B. & Sievert, H. Endovascular bariatrics: first in humans study of gastric artery embolization for weight loss. JACC Cardiovasc. Interv. 8, 1641–1644 (2015).
Simonson, D. C. et al. Treatment of obese T2DM and pre-diabetes with dual-path enteral bypass created by an incisionless anastomosis system (IAS). Presented at the American Diabetes Association Scientific Sessions, New Orleans, USA (2016).
U.S. Food and Drug Administration. U.S. Food and Drug Administration letter. FDA http://www.accessdata.fda.gov/cdrh_docs/pdf15/den150033.pdf (2016).
Lerner, H., Whang, J. & Nipper, R. Benefit-risk paradigm for clinical trial design of obesity devices: FDA proposal. Surg. Endosc. 27, 702–707 (2013).
Brethauer, S. A. et al. Endoluminal procedures for bariatric patients: expectations among bariatric surgeons. Surg. Obes. Relat. Dis. 5, 231–236 (2009).
Talamini, M. A. Benefit-risk paradigm for clinical trial design of obesity devices: FDA proposal. Surg. Endosc. 27, 701 (2013).
Cawley, J. & Meyerhoefer, C. The medical care costs of obesity: an instrumental variables approach. J. Health Econ. 31, 219–230 (2012).
Finkelstein, E. A., Trogdon, J. G., Cohen, J. W. & Dietz, W. Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Aff. (Millwood) 28, w822–w831 (2009).
Colagiuri, S. et al. The cost of overweight and obesity in Australia. Med. J. Aust. 192, 260–264 (2010).
Tsai, A. G., Williamson, D. F. & Glick, H. A. Direct medical cost of overweight and obesity in the USA: a quantitative systematic review. Obes. Rev. 12, 50–61 (2011).
Trogdon, J. G., Finkelstein, E. A., Hylands, T., Dellea, P. S. & Kamal-Bahl, S. J. Indirect costs of obesity: a review of the current literature. Obes. Rev. 9, 489–500 (2008).
Cremieux, P. Y. et al. A study on the economic impact of bariatric surgery. Am. J. Manag. Care 14, 589–596 (2008).
Keating, C. L. et al. Cost-effectiveness of surgically induced weight loss for the management of type 2 diabetes: modeled lifetime analysis. Diabetes Care 32, 567–574 (2009).
Dixon, J. B., Eaton, L. L., Vincent, V. & Michaelson, R. LAP-BAND for BMI 30-40: 5-year health outcomes from the multicenter pivotal study. Int. J. Obes. (Lond.) 40, 291–298 (2016).
Michaelson, R., Murphy, D. K., Gross, T. M., Whitcup, S. M. & LAP-BAND Lower BMI Study Group. LAP-BAND for lower BMI: 2-year results from the multicenter pivotal study. Obesity (Silver Spring) 21, 1148–1158 (2013).
Phillips, E. et al. Safety and effectiveness of Realize adjustable gastric band: 3-year prospective study in the United States. Surg. Obes. Relat. Dis. 5, 588–597 (2009).
Acknowledgements
J.D. acknowledges the support of the National Health and Medical Research Council through a senior research fellowship.
Author information
Authors and Affiliations
Contributions
Both authors contributed equally to this manuscript
Corresponding author
Ethics declarations
Competing interests
J.D. has provided consultancy services to Apollo Endosurgery, Bariatric Advantage, Covidien, Nestle Health Science, iNova Pharmaceuticals and Novo Nordisk. P.C.L. declares no competing interests.
Rights and permissions
About this article

Cite this article
Lee, P., Dixon, J. Medical devices for the treatment of obesity. Nat Rev Gastroenterol Hepatol 14, 553–564 (2017). https://doi.org/10.1038/nrgastro.2017.80
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrgastro.2017.80
This article is cited by
-
Intragastric satiety-inducing device reduces food intake and suppresses body weight gain in a rodent model
Surgical Endoscopy (2021)
-
A Novel Intragastric Satiety-Inducing Device to Inhibit Weight Gain in Juvenile Pigs: a Pilot Study
Obesity Surgery (2020)
-
Bioelectric neuromodulation for gastrointestinal disorders: effectiveness and mechanisms
Nature Reviews Gastroenterology & Hepatology (2019)
-
IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures
Obesity Surgery (2018)
