
Abstract
Cardiorespiratory fitness (CRF) is an established predictor of adverse health outcomes. The aim of this study is to investigate potential behavioral, interpersonal and socioeconomic correlates of CRF among men and women living in Germany using data from a population-based nationwide cross-sectional study. 1,439 men and 1,486 women aged 18–64 participated in the German Health Interview and Examination Survey (2008–2011) and completed a standardized sub-maximal cycle ergometer test. Maximal oxygen consumption (\(\dot{V}{O}_{2}max\)) in ml·min−1·kg−1 was estimated. Mean values of VO2max for various anthropometric, behavioral, interpersonal, and sociodemographic variables were estimated. Linear regression analyses using multiple imputations technique for missing values was performed to analyze the influence of potential correlates on CRF. Women with high alcohol consumption had higher \(\dot{V}{O}_{2}max\), (β = 2.20; 95% CI 0.98 to 3.42) than women with low alcohol consumption and women with high occupational status had higher \(\dot{V}{O}_{2}max\) (β = 1.83; 95% CI 0.21 to 3.44) in comparison to women with low occupational status. Among men, high fruit intake (β = 1.52; 95% CI 0.63 to 2.40), compared to low or medium fruit intake and performing at least 2.5 hours of total PA per week (β = 2.19; 95% CI 1.11 to 3.28), compared to less than 2.5 hours was associated with higher \(\dot{V}{O}_{2}max\). Among both men and women, lower body mass index, lower waist circumference and higher levels of physical exercise were considerably associated with higher \(\dot{V}{O}_{2}max\). Among women, those in higher age groups showed a considerably lower level of \(\dot{V}{O}_{2}max\) compared with those aged 18–24. Furthermore, mean estimated \(\dot{V}{O}_{2}max\) was higher among men (36.5; 95% CI 36.0 to 37.0) than among women (30.3; 95% CI 29.8 to 30.7). Despite the cross-sectional nature of the current study, we conclude that several behavioral, anthropometric, and sociodemographic factors are associated with CRF in the general adult population in Germany. These results can provide evidence to tailor prevention measures according to the needs of specific subgroups.
Similar content being viewed by others

Introduction
Cardiorespiratory fitness (CRF) is an important marker of cardiovascular health and thus a crucial factor in the prevention of non-communicable diseases. CRF, defined as the ability of circulatory, respiratory and muscular systems to supply oxygen during prolonged physical exercise1, has a strong inverse relation to the incidence cardiovascular diseases2, cancer3, diabetes mellitus, depression4 and all-cause mortality2. Taking into account the impact of CRF on individual health, efforts should be taken to enhance fitness in the general population. For the development of adequate interventions, knowledge about the causes of CRF, as well as population groups at elevated risk of having a low CRF, is crucial. Figure 1 shows a conceptual framework of the potential correlates of CRF adapted from a model proposed by Després5. Although CRF is partly genetically determined6, it can be enhanced by regular endurance exercise7, and further factors may play a role8. CRF has been shown to decrease with age9,10 and is on average lower among women than men11. Furthermore, numerous studies have demonstrated an association between anthropometric measures, such as waist circumference (WC) or body mass index (BMI), with CRF8. Following explanatory ecological models on physical activity (PA)12,13, one can postulate that further determinants and correlates of CRF on the individual, interpersonal, socioeconomic or environmental level could exist5,8,14. In fact, CRF has been linked to behavioral (e.g., alcohol consumption15), socioeconomic (e.g., education16) and environmental factors (e.g., commuting distance17). Finally, all of these factors are influenced by an environmental and political framework.

Schematic conceptual framework of the correlates of cardiorespiratory fitness (adapted from5). Solid lines: potential domains of the correlates of cardiorespiratory fitness investigated in the present study. Dotted lines: potential domains of the correlates of cardiorespiratory fitness not investigated in the present study. *Genetic factors were not investigated in the present study. PA physical activity, CRF cardiorespiratory fitness, NCDs non-communicable diseases.
However, evidence of consistent associations between CRF and many of these factors is limited8. While basic sociodemographic factors such as age and sex as well as physical activity and anthropometric factors have been investigated in multiple settings, research on other health behaviors or interpersonal factors is scarce. Furthermore, to our knowledge, no study has yet examined potential influencing factors of CRF within the German general population. We therefore aimed to investigate potential behavioral, interpersonal and socioeconomic correlates of CRF among men and women living in Germany using data from a population-based nationwide cross-sectional study.
Methods
Study design
The present analysis uses cross-sectional data from the German Health Interview and Examination Survey for Adults (DEGS1). DEGS1, a nationwide population based health examination survey, is part of the Federal Health Monitoring System operated by the Robert Koch Institute18. The study design is described in detail elsewhere19. Briefly, 7,238 individuals aged 18 to 79 years participated in the physical measurements component of the DEGS1. The survey design is based on a two-stage cluster random sampling procedure. In the first step, 180 sample points were randomly selected and stratified to represent regional distributions. In the second step, within these 180 units, adults were randomly drawn from local population registries stratified by 10-year age groups. Data collection took place between November 2008 and December 2011. The response rate was 42%. All methods were performed in accordance with the relevant guidelines and regulations.
Of the total sample of 5,262 individuals aged 18 to 64 years, 3,110 subjects were categorized as test-qualified for the cycle ergometer test test. Overall, 3,030 participants completed the exercise test (97.4%). \(\dot{V}{O}_{2}max\) was estimated for all participants reaching at least 75% of the age-predicted maximum heart rate. 204 (6.7%) of the participants terminated the test before reaching this heart rate. As a result, the final study sample comprised of 2,826 participants, 1,447 of whom were women and 1,379 were men (see flow diagram of participants; Supplementary Fig. 1, Additional File 1).
Outcome variable: cardiorespiratory fitness
CRF was measured in participants aged 18–64 years using a standardized, submaximal cycle ergometer test (Ergosana Sana Bike 350/450, Ergosana, Bitz, Germany). Test methodology, test protocol, and exclusion criteria are described in detail elsewhere11,20. The participants initially completed a modified version of the Physical Activity Readiness-Questionnaire (PAR-Q)21,22. In participants with contradictions reported according to PAR-Q, a physician decided whether or not such participants should be enrolled into the exercise test. CRF was assessed using the test protocol recommended by the World Health Organization (WHO)23: Beginning at 25 watts, the workload was incrementally increased by 25 watts every two minutes until 85% of the estimated age-specific maximal heartrate was exceeded, a maximum level of 350 watts was achieved or the test personnel terminated the test. Heart rate was monitored continuously throughout the test. The formula 208–0.7 · Age was used to calculate the age-predicted maximum heart rate (HRmax)24. To derive physical work capacity at HRmax (PWC100%), the measured heart rate (beats per minute) during the incremental phase was regressed against corresponding workload in watts for each participant. Assuming a linear relationship between heart rate and workload, PWC100% was obtained by extrapolation using the individual regression equation PWC100% = intercept + HRmax · slope25. PWC100% was further converted to \(\dot{V}{O}_{2}max\) using a metabolic equation provided by the American College of Sports Medicine26: 3.5 ml·min−1·kg−1 + 12.24·(PWC100%)·(body weight−1).
Potential correlates of cardiorespiratory fitness
A comprehensive systematic literature review was performed in order to identify potential individual and socioeconomic correlates of CRF8,14,16. Potential interpersonal correlates of CRF were derived from evidence regarding the association of these factors and PA12,27,28. Based on this evidence, we developed a conceptual framework that depicts potential interrelations (Fig. 1,8). Corresponding covariates described below were then selected out of the DEGS1 variable list. Information on these covariates in the DEGS1 was assessed with self-administered questionnaires, physical examinations or tests by trained study personnel following standardized procedures19.
Behavioral factors
Smoking status was classified as current (including occasional smoking), ex- or never smoking. A self-administered food frequency questionnaire was used to measure intake frequency and portion size in the last four weeks for a total of 53 food and beverage groups. This food frequency questionnaire was validated and showed reasonable validity against two 24-hour recalls29. We selected specific food-groups distinguishing between health enhancing (“fruits” and “vegetables”) and health compromising products (“sugar rich drinks”, “sugar rich foods” and “junk foods”) based on evidence from the literature30. Quantities of intake of the food-groups were calculated by combining the frequency of intake and the portion size of the relevant food and beverage groups, and classifying them into two categories using sex-specific quintiles: low to moderate intake (quintile 1–3) and high intake (quintile 4–5). A detailed flowchart of food group selection and categorization can be found in Supplementary Fig. 2, Additional File 1. Ethanol in grams per day was estimated by multiplying the calculated quantity of each alcoholic beverage with standard ethanol content. Cumulated consumption was classified as low alcohol consumption (quintile 1), medium alcohol consumption (quintile 2–4), and high alcohol consumption (quintile 5) using sex-specific quintiles (Supplementary Fig. 2, Additional File 1).
Socioeconomic factors
Participants’ need-weighted household net income (net equivalent income) was calculated based on information about estimated net income per month and number of individuals living in the household31. Income was then grouped into three categories: below 60%, 60–150% and above 150% of the median net household equivalent income, representing an income below the relative poverty line and an intermediate or relatively high income, respectively32. Educational level was assessed using the ‘Comparative Analysis of Social Mobility in Industrial Nations’ (CASMIN)33 and classified into three categories (primary, secondary, and tertiary education). Occupational status was determined using the International Socio-Economic Index of Occupational Status (ISEI)34 based on current occupation of the participants. The variable was classified into three groups: low (quintile 1), medium (quintile 2–4), high occupational status (quintile 5). Participants were further asked if they were born in Germany or abroad.
Interpersonal factors
Social support was assessed using the Oslo Three-Item Social Support Scale (OSS-3)35 and classified as poor (3–8), moderate (9–11), and strong (12–14) social support. Marital status was grouped as single, married (while living together), and separated/divorced/widowed.
Anthropometric factors
Body weight and height was measured using portable electronic scales (SECA, Germany) and stadiometer (Holtain, UK). BMI (kg/m2) was categorized according to the WHO guidelines36 into underweight (BMI <18.5), normal weight (18.5≤ BMI <25), overweight (25 ≤ BMI <30) and obese (BMI ≥30). WC was measured at the smallest site between the lowest rib and the superior border of the iliac crest with flexible, non-stretchable measurement tape37. WC was categorized as ‘normal’, ‘increased’ and ‘strongly increased’ according to international guidelines38.
Physical activity-related factors
Total PA was assessed by asking participants the number of days in an average week where they were physically active enough to start sweating or get out of breath. If they reported any PA, they were further asked about the duration of PA on such days39. Based on this information participants were classified into 2 groups, using the WHO recommendation as cut-off: <2.5 hours per week and ≥2.5 hours per week. Participants were asked “How often do you engage in physical exercise?”39, with responses categorized into three groups: no physical exercise, <2 hours/week, ≥2 hours/week.
Statistical analyses
All statistical analyses were performed with Stata 15.1 (Stata Corp., College Station, TX, USA). Stata survey commands were used to adequately account for the cluster sampling design when calculating confidence intervals. Weighting factors were used, unless otherwise noted, to adjust the distribution of the sample to match those of the German population by sex, age, education and region for all calculations40. Scatterplots were computed to show the crude, unweighted association between age, WC and BMI with \(\dot{V}{O}_{2}max\). Fractional-polynomial prediction plots with 95%-confidence intervals (95% CI) were then fitted to show the estimated associations between these variables. Mean \(\dot{V}{O}_{2}max\) with 95% CI was calculated by behavioral, sociodemographic and interpersonal, anthropometric, and PA indicators. Multivariable linear regression models were computed to estimate the associations between potential correlates and estimated \(\dot{V}{O}_{2}max\), stratified by sex. In Model 1 only age and behavioral factors (without total PA/ physical exercise) were included. In the next model (Model 2), sociodemographic and interpersonal factors were added. The subsequent models included the anthropometric (Model 3) and PA-related factors (Model 4). A complete case analysis would have led to a considerably reduced and less representative sample (n = 573 with missing values in at least one covariate; 20.3% of eligible cases [see Supplementary Fig. 1, Additional File 1]). Thus, we conducted multiple missing values imputation using chained equations41 for BMI, WC, occupational status, education, migration status, marital status, total PA, physical exercise, smoking status, alcohol consumption as well as all food variables. We imputed 30 sex-specific datasets. Linear regression analyses were performed with each of the 30 datasets and the final coefficients are the results from all datasets combined. Multivariable linear regressions were performed using Stata multiple imputation commands in combination with the survey commands.
Ethics approval and consent to participate
The study protocol was approved by the Federal and State Commissioners for Data Protection and by the ethics committee of the Charité-University Medicine Berlin (No. EA2/047/08). Informed written consent was obtained from all participants.
Results
Overall, 47.4% of the included survey participants were women and the mean age of all participants was 38.4 years (95% CI: 37.9 to 38.8). CRF test participants were younger, not retired, higher educated, and reported higher levels of physical exercise than individuals who were not qualified for the test (Supplementary Table 1, Additional File 1).
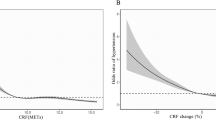
Figure 2 shows the crude and fitted association between age, BMI and WC with estimated \(\dot{V}{O}_{2}max\), indicating clear inverse associations between age, BMI, and WC with estimated \(\dot{V}{O}_{2}max\).

Association of (A) age, (B) body mass index and (C) waist circumference with cardiorespiratory fitness (\(\dot{V}{O}_{2}max\)) in men and women. \(\dot{V}{O}_{2}max\) Maximal oxygen consumption; CI confidence interval.
Mean \(\dot{{\boldsymbol{V}}}\)O 2max
Table 1 presents mean \(\dot{V}{O}_{2}max\) by covariates selected for this study. Mean \(\dot{V}{O}_{2}max\) (in ml·min−1·kg−1) was higher among men (36.5; 95% CI 36.0 to 37.0) than among women (30.3; 95% CI 29.8 to 30.7). \(\dot{V}{O}_{2}max\) decreased with age in both women and men.
Further descriptive binary analyses showed that mean \(\dot{V}{O}_{2}max\) was higher among women with high levels of alcohol consumption, secondary or tertiary education, high occupational status, high income, being single, having normal or underweight BMI, having a normal WC, being physically active and participating in physical exercise. Among men, mean \(\dot{V}{O}_{2}max\) was higher among those with high junk food intake, being born in Germany, having secondary or tertiary education, being single, having normal or underweight BMI, having a normal WC, being physically active and participating in physical exercise.
Multivariable analyses
Multivariable analyses indicated that age, smoking, alcohol consumption, fruit intake, place of birth, WC, BMI, and physical exercise were associated with estimated \(\dot{V}{O}_{2}max\) in both sexes (Table 2 and Table 3). While vegetable intake, income and occupational status were only observed to be associated with \(\dot{V}{O}_{2}max\) among women, sugar-rich food intake, marital status and total PA showed a considerable association with \(\dot{V}{O}_{2}max\) only among men.
The fully adjusted Model 4 showed a considerably lower level of \(\dot{V}{O}_{2}max\) for women in higher age groups compared with those aged 18–24: among women aged 45 to 54 years, \(\dot{V}{O}_{2}max\) decreased by \(\beta \) = −2.08 (95% CI −3.49 to −0.67) and in women aged 55 to 64 years by (\(\beta \) = −4.27; 95% CI −5.94 to −2.60), respectively (Table 2). Women with high alcohol consumption had higher \(\dot{V}{O}_{2}max\), (\(\beta \) = 2.20; 95% CI 0.98 to 3.42) than women with low alcohol consumption. Similarly, women with high occupational status had higher \(\dot{V}{O}_{2}max\) (\(\beta \) = 1.83; 95% CI 0.21 to 3.44) in comparison to women with low occupational status and those with increased and strongly increased WC had lower \(\dot{V}{O}_{2}max\) than those with normal WC (increased WC: \(\beta \) = −1.56; 95% CI −2.45 to −0.68, and strongly increased WC: \(\beta \) = −1.61; 95% CI −2.85 to −0.38). In addition, an inverse association was observed between BMI and \(\dot{V}{O}_{2}max\) among women: while underweight women had higher \(\dot{V}{O}_{2}max\) compared to normal-weight women (\(\beta \) = 3.13; 95% CI 0.58 to 5.69), overweight (\(\beta \) = −2.36; 95% CI −3.26 to −1.46) and obese (\(\beta \) = −4.88; 95% CI −6.19 to −3.57) women showed considerably lower \(\dot{V}{O}_{2}max\) compared to normal-weight women. Furthermore, among women \(\dot{V}{O}_{2}max\) increased with the amount of physical exercise per week, with \(\beta \) = 1.68 (95% CI 0.84 to 2.52) for up to two hours and \(\beta \) = 4.20 (95% CI 3.10 to 5.30) for more than two hours of physical exercise per week compared to women not engaging in any physical exercise.
Among men high fruit intake was associated with higher \(\dot{V}{O}_{2}max\), (\(\beta \) = 1.52; 95% CI 0.63 to 2.40), compared to low or medium fruit intake (Table 3). As among women, \(\dot{V}{O}_{2}max\) was lower among men with increased WC (\(\beta \) = −1.58; 95% CI −2.71 to −0.45) and strongly increased WC (\(\beta \) = −2.92; 95% CI −4.23 to −1.60) in comparison to men with normal WC. Overweight (\(\beta \) = −3.00; 95% CI −4.00 to −1.99) and obese (\(\beta \) = −5.79; 95% CI −7.39 to −4.20) men had lower \(\dot{V}{O}_{2}max\) compared to men with normal weight. Both total PA and physical exercise were considerably associated with \(\dot{V}{O}_{2}max\) among men. Men who met the WHO PA recommendation of at least 2.5 hours of total PA per week showed higher \(\dot{V}{O}_{2}max\) (\(\beta \) = 2.19; 95% CI 1.11 to 3.28) than men who did not meet the PA recommendation. An increasing level of \(\dot{V}{O}_{2}max\) was also associated with increasing weekly hours of physical exercise participation: men with up to two hours of physical exercise per week, (\(\beta \) = 1.99; 95% CI 1.00 to 2.98), and men with two hours or more of physical exercise per week (\(\beta \) = 3.74; 95% CI 2.59 to 4.88) showed higher \(\dot{V}{O}_{2}max\) compared to men who did not engage in any physical exercise.
Model comparison and additional analyses
Explained variance (R2) increased from 13.6% in Model 1 to 35.6% in Model 4 for women and from 9.8% to 34.1% for men. Age was negatively associated with \(\dot{V}{O}_{2}max\) among both sexes and indicated a strong effect size in Model 1 and Model 2. After adjustment for BMI and WC (Model 3), the effect size of age decreased for both sexes, but more strongly for men than for women. The coefficients of behavioral, interpersonal and socioeconomic factors slightly decreased after additional adjustments but the associations remained relatively stable overall. Among women, the effect size of high income on \(\dot{V}{O}_{2}max\) became smaller after adjustment for BMI and WC (Model 3) and the effect sizes of fruit intake, vegetable intake and of being born outside Germany all became smaller after adjustment for PA-related factors (Model 4). Among men, the effects of being divorced, separated or widowed and being a former smoker decreased after adjustment for anthropometric measures (Model 3). After adjustment for PA-related factors (Model 4), coefficients remained relatively stable.
As additional analyses the final Model 4 for the non sex-stratified full sample using sex as an additional covariate was computed (Supplementary Table 2, Additional File 1). Even after full adjustment women showed lower levels of estimated \(\dot{V}{O}_{2}max\) than men (\(\beta \) = −6.56; 95% CI (−7.17 to −5.94)). Furthermore, we conducted a sensitivity analysis and compared the final imputed model with a complete-case model without imputation of missing values: Despite slightly wider confidence intervals, only small deviations among the coefficients appeared (see Supplementary Figs. 3, 4, Additional File 1).
Discussion
In this study we were able to replicate the well-established relationships in the literature between anthropometric measures (BMI and WC), total PA and physical exercise, and estimated \(\dot{V}{O}_{2}max\) using data from a nation-wide, population-based cross-sectional health examination survey among adults in Germany. In addition, we demonstrated associations between a range of additional individual and interpersonal factors and CRF. Among women, high levels of alcohol consumption, high occupational status, lower BMI, smaller WC and higher physical exercise level were associated with higher \(\dot{V}{O}_{2}max\). Among men, lower age, high intake of fruits, lower BMI, smaller WC, at least 2.5 hours of PA per week and higher physical exercise level were associated with higher \(\dot{V}{O}_{2}max\).
Sex and age differences
The observation that men have a higher CRF than women has been reported in a number of previous studies, both internationally and in Germany8,11,42,43. In the current study, women had 17% lower \(\dot{V}{O}_{2}max\) than men, which is comparable to an often reported sex difference in CRF of about 20%8,11. Lower fitness among women compared to men is commonly explained by women’s smaller organ and body size and higher percentage of body fat on average and lower skeletal muscle mass7,44. Additional analyses with sex as an additional covariate showed that sex differences are not mediated by the anthropometric, behavioral, sociodemographic and interpersonal factors used in the fully adjusted model.
Our finding of decreasing \(\dot{V}{O}_{2}max\) with increasing age corresponds with evidence from both cross-sectional and cohort studies8,9,10. Potential explanations are physiological adjustments during the aging process, such as muscle mass atrophy, increasing burden of disease, and onset of physical limitations. Although, the use of coronary drugs and cardiovascular diseases were contraindications for test participation in this study, other illnesses and medications could affect the results20. Therefore, our study-sample consists of a relatively healthy population aged <65 years.
After adjustment for total PA and physical exercise (Model 4), there was no considerable age-effect among men. According to the literature, the effect of PA on the decline in CRF over the life course is inconclusive45,46. While longitudinal studies found that individuals with enhanced PA levels had a smaller decline in CRF than sedentary individuals46, there was no evidence for the mitigation of the effect by PA in meta-analyses of cross-sectional data47,48.
Behavioral factors
Former smokers demonstrated lower fitness compared to non-smokers in bivariate analyses and Model 2, but the effect decreased when controlling for anthropometric and PA-related factors. Most studies investigating the association between smoking and CRF have found lower fitness levels among smokers compared with non-smokers, but some other studies have not found such association8. Two studies with NHANES data, adjusted for multiple variables, even observed higher fitness levels among young to middle-aged adult current smokers in both sexes49 or in the male subsample50. While all studies observing no or a positive association had a cross sectional design, all longitudinal studies observed lower CRF levels among smokers compared with non-smokers51,52,53,54,55. Thus, in a cross-sectional study design, the effect of smoking on CRF might be hidden due to confounding, e.g. by age, as especially ex-smokers are usually older than current or never smokers. They may also have quit smoking because of health problems. In our analysis, the adequate elucidation of the effect of smoking on CRF could be hampered by the use of smoking status instead of quantitative measures of smoking (e.g., pack years).
We observed higher CRF among women with high levels of alcohol consumption. A study investigating the association between alcohol consumption and CRF based on five independent population-based studies from the US and Germany (including DEGS1) found an inverse u-shaped association with higher fitness levels among moderately drinking men and women15. However, these findings are in line with the results of our study, as Baumeister et al. observed a maximum of the curve at a very high level of consumption among women (ca. 35 g/d). In DEGS1, few women (<2%) reach this high level of consumption and correspondingly most women in the high consumption category consume less alcohol per day. Higher levels of fitness among individuals who consume alcohol are consistent with research on PA and alcohol intake. Studies in the past found that moderate or even high alcohol consumption is associated with higher levels of PA56. However, the mechanisms behind this relation are not fully understood. One possible explanation is that both PA and alcohol consumption work as rewarding stimuli and have overlapping effects in individuals stress regulation mechanisms56. Another possible explanation could be that specific personality characteristics like extroversion might correlate with both alcohol consumption (opportunities) and physical exercise (with others). Finally, confounding has to be considered as a possible explanation, as alcohol consumption is more common among higher educated women in Germany57,58 who are practicing a lifestyle that includes more physical exercise39,59 translating into higher CRF.
We observed higher CRF among men with high fruit intake. This is in line with results from the CARDIA-Study, where higher CRF was observed among men with a relative high level of fruit and vegetable intake60. Although in the final model of our study none of the other food groups (sugar-rich foods, sugar-rich drinks, junk food, vegetables) showed association with \(\dot{V}{O}_{2}max\), for most food groups a tendency toward higher CRF among participants with high intake could be observed. The food frequency questionnaire used in DEGS1 included a limited number of food groups of which some are relatively broad. Therefore, we did not adjust for overall energy intake29. Thus, higher CRF among participants with high intake of any food- and beverage group could be related to a higher energy requirement. However, the inclusion of physical activity as well as body mass index may partly adjust for energy needs.
Socioeconomic and interpersonal factors
In the multivariable analyses, fitness was not associated with education or income, but we observed considerably higher fitness among women with high occupational status. While a previous study found that for other health indicators (e.g., smoking and obesity), education showed stronger effect sizes than occupational status, this was not the case for PA61. Other studies showed mixed results regarding the association between CRF and education, with a tendency for higher fitness levels among the highly educated16. A meta-analysis of four population-based studies (including DEGS1) found a positive association between education and CRF, but no relation after adjustment for PA16. While this meta-analysis adjusted for important confounders, no other measures of SES, such as occupational status or income were included. This may explain the differences with the results found in our study.
Higher fitness among individuals with high occupational status is in line with previous research16, although studies investigating the effect of occupational status on fitness are scarce. It is possible that lower occupational status is associated with higher levels of occupational PA62,63. Described as the ‘physical activity paradox’64, recent research suggests that there are no positive health effects of occupational PA. In fact, the effects of occupational PA might be inverse65,66,67. One hypothesized explanation for this paradox is that occupational PA is usually of too low intensity or too long duration without recovery time to improve CRF68. In addition, individuals with high occupational status tend to be more active during leisure time, improving their CRF61,69,70.
We found no evidence that interpersonal factors (social support and marital status) are strongly correlated with individual fitness. Overall, research on this topic is scarce. To our knowledge, there is no study that has investigated this association of social support with CRF so far. Regarding the relation of social support and PA, there is inconclusive evidence that social support is higher among more active individuals12,71.
Marital status was not considerably associated with CRF in our analysis, but, in contrast to women, divorced men tended to have higher fitness on average than married men. A longitudinal study from the US found that changes in marital status influence fitness status in men and women differently, supporting our observations: among men, the transition to being married was associated with a decrease in \(\dot{V}{O}_{2}max\), while being divorced was associated with a modest non-significant increase. In contrast, no clear patterns were observed among women72.
Anthropometric factors
We observed strong associations between the anthropometric measures BMI and WC and \(\dot{V}{O}_{2}max\). In fact, the anthropometric factors showed the largest association among all behavioral, interpersonal and socioeconomic factors investigated, with the exception of PA-related variables.
Consistent with the findings of other studies, women and men with overweight or obesity had lower \(\dot{V}{O}_{2}max\) than individuals with a normal BMI73,74,75,76. Furthermore, our results indicated a higher CRF for underweight women, but no relation between underweight and \(\dot{V}{O}_{2}max\) was observed in men. Compared with the large number of studies that have investigated the association between continuous BMI or overweight or obesity (as measured by BMI), and CRF8, we are aware of only one study examining the association between underweight (defined by BMI) and CRF in adults. The study, conducted in a population-based sample from Taiwan reported lower CRF in underweight men, but not in women77. The strong relation between \(\dot{V}{O}_{2}max\) and BMI may be generated by the definition of \(\dot{V}{O}_{2}max\) as being relative to body weight75. Nevertheless, a study investigating \(\dot{V}{O}_{2}max\) relative to fat-free mass also showed a negative association with obesity, as measured by BMI, in both men and women78.
Independent of BMI, increased WC was strongly associated with lower CRF in men and women. This is in line with previous findings investigating the association between abdominal obesity measured by WC and CRF8,79,80. It has been hypothesized that for specific health outcomes, a low CRF attenuates the health risk of obesity as measured by BMI81. Simultaneously, studies have shown that higher CRF is associated with less abdominal fat and visceral adipose tissue82. Thus, it can be argued that the larger health effects of CRF compared to BMI may be mediated by the reduced abdominal adiposity in individuals with higher fitness levels82.
Physical activity-related factors
We observed strong associations between physical exercise as well as total PA and CRF among men and between physical exercise and CRF among women. It is empirically well documented that most people respond to regular physical exercise and training with short- and long-term physiological adaptations, which improve the CRF83,84. Greater activity amounts and intensities result, in general, in greater improvement of CRF7. Our results confirm this dose-response relationship with further increases of CRF with higher amounts of physical exercise per week. However, not all types of PA have the same beneficial effects for CRF, which could explain the differences for total PA compared with physical exercise found in our study. For example, occupational PA might be either of too low intensity or of too long duration to improve CRF. This might be the reason why total PA showed smaller effects sizes than physical exercise67,85.
Practical implications
In Germany, there is great potential to increase the CRF of the general population11,86. The results of our study provide evidence to tailor interventions or prevention measures according to the needs of specific subgroups. For example, women with a low occupational position should be enabled to perform sufficient physical exercise to enhance their fitness levels. The suggested measures of the Global Action Plan on Physical Activity by the World Health Organization87 can be a good reference when planning measures to enhance the activity level of the population. Following the recommendations of the WHO, such measures should not solely focus on the individual, but also address the environment. In the case of women with low occupational status, this can for example translate into support for active transport to work or political measures to reconcile work and family life to enable more time for recreational PA. Furthermore, the association of \(\dot{V}{O}_{2}max\) and consumption of specific foods might be an indication that different favorable health behaviors should not necessarily be seen separately, but rather be addressed at the same time. Again, such measures should focus on improvements of the living environment to foster individuals to make healthy choices.
Strengths and limitations
Strengths of this study include the large population-based sample and its comprehensive nature, allowing for the investigation of a broad range of behavioral, interpersonal, and socioeconomic factors as potential correlates of CRF. Nonetheless, due to the cross-sectional design of the present study, no conclusions regarding causality can be drawn and there may have been potential bias related to reverse causality. The study sample consisted of a relatively healthy population that was rated as being test-qualified according to the PAR-Q screener, which could compromise the generalizability of the results. Another strength of the present study is that the measurement of CRF is based on a highly standardized and quality assured survey procedure20,88. In this study, as in most epidemiological studies investigating large populations7,8, we did not assess \(\dot{V}{O}_{2}max\) directly via breath gas analyses, but estimated \(\,\dot{V}{O}_{2}max\) based on a submaximal ergometer test. However, previous validation studies have shown that directly measured \(\dot{V}{O}_{2}max\) in a maximal test and estimated \(\dot{V}{O}_{2}max\) in a submaximal test are highly correlated89. Furthermore, the exposure variable physical exercise included information about the weekly duration but not about intensity which can have great impact on CRF7. Even though DEGS1 includes a wide range of health-related variables, some known correlates of CRF which were investigated in previous studies, e.g. caffeine consumption90, were not considered due to lacking information in the DEGS1 data set. Major efforts during the study process were made to reduce potential sources of bias19. Nevertheless, as most of the covariates were based on self-reporting by participants, reporting bias cannot be ruled out. Despite the various measures that were taken to enhance the willingness to participate, to account for unequal sampling probabilities and to adjust the distribution of the sample to the official population statistics, it cannot be ruled out that the relatively low response rate could have contributed to a potential selection bias. Although we used weighting factors, specific population groups, such as those with lower education status and individuals with migration background, may be underrepresented in our study.
Conclusions
Despite the cross-sectional nature of the current study, we conclude that several factors at different domains of the conceptual framework are associated with CRF in the general adult population in Germany. These results can provide evidence to tailor prevention measures according to the needs of specific subgroups. Such measures should not solely focus on the individual, but also include actions on the environmental and political level.
Data availability
Datasets of DEGS1 are available as Public Use File: https://www.rki.de/EN/Content/Health_Monitoring/Public_Use_Files/application/application_node.html.
References
World Health Organization. Global recommendations on physical activity for health. Appendix 5. (WHO, Geneva, 2010).
Kodama, S. et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 301, 2024–2035 (2009).
Schmid, D. & Leitzmann, M. F. Cardiorespiratory fitness as predictor of cancer mortality: a systematic review and meta-analysis. Ann. Oncol. 26, 272–278 (2015).
Schuch, F. B. et al. Are lower levels of cardiorespiratory fitness associated with incident depression? A systematic review of prospective cohort studies. Prev. Med. 93, 159–165 (2016).
Després, J. P. Physical Activity, Sedentary Behaviours, and Cardiovascular Health: When Will Cardiorespiratory Fitness Become a Vital Sign? Can. J. Cardiol. 32, 505–513 (2016).
Bouchard, C. et al. Familial aggregation of VO2max response to exercise training: results from the HERITAGE Family Study. J. Appl. Physiol. 87, 1003–1008 (1999).
Ross, R. et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 134, e653–e699 (2016).
Zeiher, J. et al. Correlates and determinants of cardiorespiratory fitness in adults: a systematic review. Sports Med. Open, 5, 39 (2019).
Schneider, J. Age dependency of oxygen uptake and related parameters in exercise testing: an expert opinion on reference values suitable for adults. Lung 191, 449–458 (2013).
Shvartz, E. & Reibold, R. C. Aerobic fitness norms for males and females aged 6 to 75 years: a review. Aviat. Space Environ. Med. 61, 3–11 (1990).
Finger, J. D., Krug, S., Gößwald, A., Härtel, S. & Bös, K. Cardiorespiratory fitness among adults in Germany. Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56, 772–778 (2013).
Bauman, A. E. et al. Correlates of physical activity: why are some people physically active and others not? Lancet 380, 258–271 (2012).
Sallis, J. F. et al. An ecological approach to creating active living communities. Annu. Rev. Public. Health 27, 297–322 (2006).
Perumal, N., Mensink, G. B. M., Keil, T. & Finger, J. D. Why are some people more fit than others? Correlates and determinants of cardiorespiratory fitness in adults: protocol for a systematic review. Syst. Rev. 6, 102 (2017).
Baumeister, S. E. et al. Alcohol consumption and cardiorespiratory fitness in five population-based studies. Eur. J. Prev. Cardiol. 25, 164–172 (2018).
Ombrellaro, K. J. et al. Socioeconomic Correlates and Determinants of Cardiorespiratory Fitness in the General Adult Population: a Systematic Review and Meta-Analysis. Sports Med. Open. 4, 25 (2018).
Hoehner, C. M. et al. Understanding the independent and joint associations of the home and workplace built environments on cardiorespiratory fitness and body mass index. Am. J. Epidemiol. 178, 1094–1105 (2013).
Kurth, B.-M. Das RKI-Gesundheitsmonitoring - Was es enthält und wie es genutzt werden kann [The RKI health monitoring - What it contains and how it can be used]. Public. Health Forum 20(4), e1-4. e3 (2012).
Scheidt-Nave, C. et al. German health interview and examination survey for adults (DEGS) - design, objectives and implementation of the first data collection wave. BMC Public. Health 12, 730 (2012).
Finger, J. D. et al. Measurement of cardiorespiratory fitness in the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56, 885–893 (2013).
Deutsche Gesellschaft für Sportmedizin und Prävention (DGSP). PAR-Q-Fragebogen (German version) (2007).
Canadian Society for Exercise Physiology. Physical Activity Readiness Questionnaire - PAR-Q (revised 2002), (Health Canada, Ottawa, 2002).
Andersen, K.L., Shephard, R., Denolin, H., Varnauskas, E. & Masironi, R. Fundamentals of exercise testing. (1971).
Tanaka, H., Monahan, K. D. & Seals, D. R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 37, 153–156 (2001).
Gore, C. J., Booth, M. L., Bauman, A. & Owen, N. Utility of pwc75% as an estimate of aerobic power in epidemiological and population-based studies. Med. Sci. Sports Exerc. 31, 348–351 (1999).
American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. 5th Edition ed., (Williams & Wilkins, Baltimore:, 1995, p.280).
Choi, J., Lee, M., Lee, J. K., Kang, D. & Choi, J. Y. Correlates associated with participation in physical activity among adults: a systematic review of reviews and update. BMC Public. Health 17, 356 (2017).
Jaeschke, L. et al. Socio-cultural determinants of physical activity across the life course: a ‘Determinants of Diet and Physical Activity’ (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 14, 173 (2017).
Haftenberger, M., et al. Relative validation of a food frequency questionnaire for national health and nutrition monitoring. Nutr. J. 9 (2010).
Afshin, A. et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 393, 1958–1972 (2019).
Lampert, T., Kroll, L. E., Müters, S. & Stolzenberg, H. Measurement of socioeconomic status in the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz 56, 1–5 (2013).
Federal Ministry of Labour and Social Affairs [Bundesministerium für Arbeit und Soziales] (ed.) Life Situations in Germany. The German Federal Government’s 3rd Report on Poverty and Wealth. Executive Summary, (BMAS, Berlin, 2008).
Brauns, H., Scherer, S. & Steinmann, S. The CASMIN Educational Classification in International Comparative Research. In Advances In Cross-National Comparison (eds. Hoffmeyer-Zlotnik, J. H. P. & Wolf, C.) 221-244 (Springer US, Boston, MA, 2003).
Ganzeboom, H. B. G., De Graaf, P. M. & Treiman, D. J. A Standard International Socio-Economic Index of Occupational Status. Soc. Sci. Res. 21, 1–56 (1992).
Meltzer, H. Development of a common instrument for mental health. In EUROHIS: Developing common instruments for health surveys (eds. Nosikov, A. & Gudex, C.) (IOS Press, Amsterdam, 2003).
World Health Organization. BMI classification (2019).
Haftenberger, M. et al. Changes in Waist Circumference among German Adults over Time - Compiling Results of Seven Prospective Cohort Studies. Obes. Facts 9, 332–343 (2016).
World Health Organization. Obesity: preventing and managing the global epidemic, (World Health Organization, Genf, 2000).
Krug, S. et al. Physical activity. Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56, 765–771 (2013).
Kamtsiuris, P. et al. The first wave of the German Health Interview and Examination Survey for Adults (DEGS1). Sampling design, response, weighting, and representativeness. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56, 1–10 (2013).
White, I. R., Royston, P. & Wood, A. M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 30, 377–399 (2011).
Wang, C. Y. et al. Cardiorespiratory fitness levels among US adults 20–49 years of age: findings from the 1999–2004 National Health and Nutrition Examination Survey. Am. J. Epidemiol. 171, 426–435 (2010).
Loe, H., Rognmo, Ø., Saltin, B. & Wisløff, U. Aerobic Capacity Reference Data in 3816 Healthy Men and Women 20–90 Years. PLoS ONE 8, e64319 (2013).
Al-Mallah, M. H. et al. Sex Differences in Cardiorespiratory Fitness and All-Cause Mortality: The Henry Ford ExercIse Testing (FIT) Project. Mayo Clin. Proc. 91, 755–762 (2016).
Zoeller, R. F. Gender Differences in Cardiorespiratory Fitness With Advancing Age: Is the Age-Associated Decline in VO2max More Rapid in Men and Do Older Men and Women Respond Differently to Exercise? Am. J. Lifestyle Med. 2, 492–499 (2008).
Hawkins, S. A. & Wiswell, R. A. Rate and Mechanism of Maximal Oxygen Consumption Decline with Aging. Sports Med. 33, 877–888 (2003).
Wilson, T. M. & Tanaka, H. Meta-analysis of the age-associated decline in maximal aerobic capacity in men: relation to training status. Am. J. Physiol. Heart Circ. Physiol 278, H829–H834 (2000).
Fitzgerald, M. D., Tanaka, H., Tran, Z. V. & Seals, D. R. Age-related declines in maximal aerobic capacity in regularly exercising vs. sedentary women: a meta-analysis. J. Appl. Physiol. 83, 160–165 (1997).
Thai, A., Papapanou, P. N., Jacobs, D. R. Jr., Desvarieux, M. & Demmer, R. T. Periodontal infection and cardiorespiratory fitness in younger adults: Results from continuous National Health and Nutrition Examination Survey 1999–2004. PLoS ONE 9 (2014).
Ceaser, T. G., Fitzhugh, E. C., Thompson, D. L. & Bassett, D. R. Jr. Association of physical activity, fitness, and race: NHANES 1999–2004. Med. Sci. Sports Exerc. 45, 286–293 (2013).
Bernaards, C. M., Twisk, J. W., Van Mechelen, W., Snel, J. & Kemper, H. C. A longitudinal study on smoking in relationship to fitness and heart rate response. Med. Sci. Sports Exerc. 35, 793–800 (2003).
Fleg, J. L. et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation 112, 674–682 (2005).
Jackson, A. S., Sui, X., Hebert, J. R., Church, T. S. & Blair, S. N. Role of lifestyle and aging on the longitudinal change in cardiorespiratory fitness. Arch. Intern. Med. 169, 1781–1787 (2009).
Sandvik, L., Erikssen, G. & Thaulow, E. Long term effects of smoking on physical fitness and lung function: a longitudinal study of 1393 middle aged Norwegian men for seven years. BMJ 311, 715–718 (1995).
Sidney, S. et al. Seven-year change in graded exercise treadmill test performance in young adults in the CARDIA study. Cardiovascular Risk Factors in Young Adults. Med. Sci. Sports Exerc. 30, 427–433 (1998).
Leasure, J. L., Neighbors, C., Henderson, C. E. & Young, C. M. Exercise and Alcohol Consumption: What We Know, What We Need to Know, and Why it is Important. Front Psychiatry 6 (2015).
Lange, C., Manz, K. & Kuntz, B. Alcohol consumption among adults in Germany: risky drinking levels. J. Health Monit. 2, 64–70 (2017).
Bloomfield, K., Grittner, U., Kramer, S. & Gmel, G. Social inequalities in alcohol consumption and alcohol-related problems in the study countries of the EU concerted action ‘Gender, Culture and Alcohol Problems: a Multi-national Study’. Alcohol. Alcohol 41, i26–36 (2006).
Beenackers, M. A. et al. Socioeconomic inequalities in occupational, leisure-time, and transport related physical activity among European adults: a systematic review. Int. J. Behav. Nutr. Phys. Act. 9, 116 (2012).
Shikany, J. M. et al. Associations between food groups, dietary patterns, and cardiorespiratory fitness in the Coronary Artery Risk Development in Young Adults study. Am. J. Clin. Nutr. 98, 1402–1409 (2013).
Nocon, M., Keil, T. & Willich, S. N. Education, income, occupational status and health risk behaviour. J. Public. Health 15, 401–405 (2007).
Smith, L. et al. A review of occupational physical activity and sedentary behaviour correlates. Occup. Med. (Lond.) 66, 185–192 (2016).
Finger, J. D., Tylleskär, T., Lampert, T. & Mensink, G. B. Physical activity patterns and socioeconomic position: the German National Health Interview and Examination Survey 1998 (GNHIES98). BMC Public. Health 12, 1079 (2012).
Holtermann, A., Hansen, J. V., Burr, H., Søgaard, K. & Sjøgaard, G. The health paradox of occupational and leisure-time physical activity. Br. J. Sports Med. 46, 291–295 (2012).
Li, J., Loerbroks, A. & Angerer, P. Physical activity and risk of cardiovascular disease: what does the new epidemiological evidence show? Curr. Opin. Cardiology 28, 575–583 (2013).
Li, J. & Siegrist, J. Physical activity and risk of cardiovascular disease–a meta-analysis of prospective cohort studies. Int. J. Env. Res. Public. Health 9, 391–407 (2012).
Coenen, P. et al. Do highly physically active workers die early? A systematic review with meta-analysis of data from 193 696 participants. Br. J. Sports Med. 52, 1320–1326 (2018).
Holtermann, A., Krause, N., van der Beek, A. J. & Straker, L. The physical activity paradox: six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 52, (149–150 (2018).
Gidlow, C., Johnston, L. H., Crone, D., Ellis, N. & James, D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ. J. 65, 338–367 (2006).
Hoebel, J., Finger, J. D., Kuntz, B. & Lampert, T. Sozioökonomische Unterschiede in der körperlich-sportlichen Aktivität von Erwerbstätigen im mittleren Lebensalter [Socioeconomic differences in physical activity in the middle-aged working population. The role of education, occupation, and income]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 59, 188–196 (2016).
Wendel-Vos, W., Droomers, M., Kremers, S., Brug, J. & van Lenthe, F. Potential environmental determinants of physical activity in adults: a systematic review. Obes. Rev. 8, 425–440 (2007).
Ortega, F. B. et al. In fitness and health? A prospective study of changes in marital status and fitness in men and women. Am. J. Epidemiol. 173, 337–344 (2011).
Carnethon, M. R., Gulati, M. & Greenland, P. Prevalence and cardiovascular disease correlates of low cardiorespiratory fitness in adolescents and adults. JAMA 294, 2981–2988 (2005).
Lakoski, S. G. et al. Impact of Body Mass Index, Physical Activity, and Other Clinical Factors on Cardiorespiratory Fitness (from the Cooper Center Longitudinal Study). Am. J. Cardiol. 108, 34–39 (2011).
Fogelholm, M. et al. Waist circumference and BMI are independently associated with the variation of cardio-respiratory and neuromuscular fitness in young adult men. Int. J. Obes. 30, 962–969 (2006).
Sui, X. et al. Physical activity/fitness peaks during perimenopause and BMI change patterns are not associated with baseline activity/fitness in women: a longitudinal study with a median 7-year follow-up. Br. J. Sports Med. 47, 77–82 (2013).
Hung, T. H., Liao, P. A., Chang, H. H., Wang, J. H. & Wu, M. C. Examining the relationship between cardiorespiratory fitness and body weight status: Empirical evidence from a population-based survey of adults in Taiwan. Scientific World Journal 2014 (2014).
Duvigneaud, N. et al. Relationship of obesity with physical activity, aerobic fitness and muscle strength in Flemish adults. J. Sports Med. Phys. Fit. 48, 201–210 (2008).
Ross, R. & Katzmarzyk, P. T. Cardiorespiratory fitness is associated with diminished total and abdominal obesity independent of body mass index. Int. J. Obes. 27, 204 (2003).
Dagan, S. S., Segev, S., Novikov, I. & Dankner, R. Waist circumference vs body mass index in association with cardiorespiratory fitness in healthy men and women: a cross sectional analysis of 403 subjects. Nutr. J. 12, 12 (2013).
Fogelholm, M. Physical activity, fitness and fatness: relations to mortality, morbidity and disease risk factors. A systematic review. Obes. Rev. 11, 202–221 (2010).
Wong, S. L. et al. Cardiorespiratory fitness is associated with lower abdominal fat independent of body mass index. Med. Sci. Sports Exerc. 36, 286–291 (2004).
Hawley, J. A., Hargreaves, M., Joyner, M. J. & Zierath, J. R. Integrative biology of exercise. Cell 159, 738–749 (2014).
Lin, X. et al. Effects of Exercise Training on Cardiorespiratory Fitness and Biomarkers of Cardiometabolic Health: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Am Heart Assoc 4 (2015).
Savinainen, M., Nygard, C. H. & Ilmarinen, J. A 16-year follow-up study of physical capacity in relation to perceived workload among ageing employees. Ergonomics 47, 1087–1102 (2004).
Finger, J. D. et al. Referenzwerte für die kardiorespiratorische Fitness der allgemeinen Bevölkerung: Die Studie zur Gesundheit Erwachsener in Deutschland (DEGS1) 2008–2011 [Reference Values for Cardiorespiratory Fitness of the General Population: The German National Health Interview and Examination Survey for Adults (DEGS1) 2008–2011]. Gesundheitswesen https://doi.org/10.1055/a-1026-6220 (2019).
World Health Organization. Global action plan on physical activity 2018–2030: more active people for a healthier world, (WHO, Geneva, 2018).
Gößwald, A., Lange, M., Dölle, R. & Hölling, H. The first wave of the German Health Interview and Examination Survey for Adults (DEGS1). Recruitment of participants, fieldwork, and quality assurance. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 56, 1–8 (2013).
Noonan, V. & Dean, E. Submaximal exercise testing: Clinical application and interpretation. Phys. Ther. 80, 782–807 (2000).
Tripette, J. et al. Caffeine Consumption Is Associated With Higher Level of Physical Activity in Japanese Women. Int. J. Sport. Nutr. Exerc. Metab. 28, 474–479 (2018).
Acknowledgements
We thank Marion Barnett and Maurice Duch for editing a draft of this manuscript. No external funding was received. The study was financed by the Robert Koch Institute which is a federal institute within the portfolio of the German Federal Ministry of Health.
Author information
Authors and Affiliations
Contributions
G.B.M.M. and J.D.F. were involved in the design and conduct of DEGS1, J.D.F. in particular for the ergometer testing. J.Z., N.P. and J.D.F. conceptualized the current study. J.Z. conducted the present analysis and drafted the manuscript. G.B.M.M. and T.K. contributed to the analysis plan and interpretation of the results. K.M., B.K., N.P., T.K., G.B.M.M. and J.D.F. critically revised it. K.M. and J.D.F. contributed to the writing of the manuscript. All authors contributed to the interpretation of findings, reviewed, edited and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zeiher, J., Manz, K., Kuntz, B. et al. Individual and interpersonal correlates of cardiorespiratory fitness in adults – Findings from the German Health Interview and Examination Survey. Sci Rep 10, 445 (2020). https://doi.org/10.1038/s41598-019-56698-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-56698-z
This article is cited by
-
Sociodemographic correlates of physical activity and sport among adults in Germany: 1997–2018
German Journal of Exercise and Sport Research (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
