
Abstract
Study design:
A 3-month follow-up, observational, prospective, multicenter, study in traumatic spinal cord-injured (SCI) patients with neuropathic pain (NP).
Objectives:
To assess the effectiveness and safety of oxycodone treatment in SCI patients with anticonvulsants-refractory NP.
Setting:
‘Spinal injury follow-up units’ throughout Spain.
Methods:
Data regarding NP characteristics were collated from male and female adults with traumatic SCI and difficult-to-control central NP of moderate-to-severe intensity (visual analog scale (VAS) ⩾4) persisting ⩾1 month, who had been para- or tetraplegic for ⩾2 months, had been previously treated with anticonvulsants and were now treated with oxycodone.
Results:
In all, 54 out of the 57 patients recruited were assessable. A total of 81% were men and the mean age was 46.4. Patients were treated with oxycodone, 83% combined with anticonvulsant. Pain intensity (VAS: 7.1±1.3–4.3±1.7) and Lattinen total score (13.2±3–7.7±3.4) decreased significantly (P<0.001) along the study. No patient got worse regarding pain impact on physical activity and on sleep (Lattinen scale). EQ-5D VAS showed a trend to increase (P=0.061) and the index of preference values increased significantly from baseline to month 3 (0.26–0.62; P<0.001). A total of 53.7% patients showed at least one treatment-related adverse event, with constipation being the most frequent one (33.3%).
Conclusion:
Oxycodone treatment, mostly in combination with anticonvulsants, in SCI patients with NP decreases pain intensity, improves health-related quality of life and diminishes the impact of pain on physical activity and sleep.
Sponsorship:
This study has been sponsored by Mundipharma, SL, Madrid, Spain.
Similar content being viewed by others
Introduction
A spinal cord injury (SCI) imposes on patients not only physical disabilities but also a great impact on their social life with severe psychological implications and decreased quality of life. The global annual incidence has been estimated at 10–80 cases per million inhabitants. In Spain, the incidence is 12–20 patients per million inhabitants per year and the estimated prevalence in 1997 was 14 000.1
One of the more disabling consequences of SCI and with more impact on the quality of life of the patient is chronic pain.2 The prevalence of chronic pain after SCI ranges from 26 to 96%,3 with pain being moderate-to-severe in 25–60% of patients.4, 5 Chronic pain has a great impact on the ability to regain optimal level of activity and on employment status, interferes with sleep and causes anxiety and depression,5, 6 which are also a direct effect of the disabling consequences of the SCI, having a negative effect on the quality of life and imposing a major burden on patients.
SCI-related pain can be classified in nociceptive or neuropathic (NP).3 The percentage of patients with NP after SCI ranges from 20 to 75%,4, 6 and are the ones with more psychological distress and more refractory to treatment.7 Despite the high prevalence of post-SCI NP and its highly negative impact on the quality of life, there are few studies regarding this type of pain. Anticonvulsants, tricyclic antidepressants and some opioids have been used;8, 9 however, management is still a challenge, as patients are not satisfied with the pain control obtained.10 Oxycodone has level A evidence efficacy for NP in postherpetic neuralgia and diabetic neuropathy.11 A sustained release form of oxycodone in a case of central pain provided greater pain reduction when added to dextromethorphan12 and in central NP studies with anticonvulsants resulting in treatment success, opioids, including oxycodone, were the concomitant therapy in half the patients.13
Therefore, this study aimed to assess the effectiveness of oxycodone treatment in SCI patients with anticonvulsants-refractory NP, aiming to find a treatment for better NP control.
Methods
A 3-month follow-up, observational, prospective, multicenter study was carried out to assess the oxycodone treatment in SCI patients with anticonvulsants-refractory NP. The study followed the International Guidelines for Ethical Review of Epidemiological Studies (Council for the International Organizations of Medical Sciences, Geneve 1991), and Declaration of Helsinki (amended in Tokyo, 2004) and previous to start-up, it was approved by the Ethic Committee of Hospital Insular de Gran Canaria, Spain.
The study aimed to assess the effectiveness of oxycodone as SCI-related NP treatment, specifically its effect on pain intensity, patients’ quality of life and pain impact on physical activity and sleep quality; and to determine prevalence of adverse reactions associated to this treatment.
Patients included were male and female adults with spinal injury of traumatic origin and central NP (by International Association for the Study of Pain classification)14 of moderate-to-severe intensity (visual analog scale (VAS) ⩾4) persisting ⩾1 month, who had been para- or tetraplegic for ⩾2 months and had been previously treated with anticonvulsants. Exclusion criteria were psychiatric or neurologic disorder that might affect the patient's ability to participate in the study, drugs and/or alcohol use, enteral nutrition by nasogastric tube or gastrostomy, severe respiratory disease and severe hepatic or renal insufficiency, which might limit pain management.
Patients gave their informed consent and the information for the study was obtained from the clinical history and from the patients themselves, following routine clinical practice. Four ‘SCI units’ throughout Spain, whose usual protocols for SCI refractory NP included oxycodone, mostly associated to anticonvulsant, participated in the study. Patients were included from September 2008 to April 2009 and followed up from January to July 2009.
The following data were collated at baseline: demographic data; SCI etiology, date of occurrence, American Spinal Injury Association level and classification and spasticity rating (Ashworth); type of pain according to the classification of the International Association for the Study of Pain,14 and description using a SCI pain classification system (above level, at level and below level),15 NP characterization by DN4 scale, presence of allodynia and/or hyperalgesia, intensity (by means of a VAS) and frequency of pain, frequency of analgesia use, and pain impact on physical activity and on sleep (Lattinen scale); quality of life (EuroQoL 5D); analgesic treatment, need for treatment change, new treatment and concomitant antiemetic or laxative treatment. At 1 and 3-month visits, the following parameters were assessed: NP intensity, spasticity, irruptive or breakthrough pain crisis and treatment, analgesic, antiemetic and laxative treatment and adverse reactions related to the analgesic treatment, and the Lattinen and EuroQoL 5D (this last one only at 3-month) scales were administered.
Scales used
The DN4 scale is a diagnostic test for NP. This 10-item questionnaire consists on pain descriptors and signs that are yes (1) or no (0) evaluated, with a diagnosis breakpoint of 4.
The Lattinen test or index is a scale composed of five categories: pain intensity, patient activity, pain frequency, use of analgesics and hours of sleep. Each category comprises five Likert-type items scored from 0 (better) to 4 (worse). Maximum score of the scale is 20 and a decrease in the score indicates an improvement in patient status.
The modified Ashworth scale assigns grades to a manually determined resistance of muscle to passive stretching and hence, it assesses spasticity. Grades are 0, 1, 1+, 2, 3 and 4, with 0 being normal muscle tone and 4 limb rigid in flexion or extension.
As there is no validated scale to measure the quality of life, specifically in SCI patients, the EuroQOL-5D (EQ-5D) from the EuroQol Group was used, but questions about ability to walk was replaced with the ability to move with a wheelchair. EQ-5D is a standardized, non-disease-specific instrument for describing and valuing health-related quality of life. The Spanish version rates mobility, self-care, usual activities, pain/discomfort and anxiety/depression in three severity levels (no problem=1, some or moderate problems=2, many problems=3). The different combinations of the values of the five dimensions give 243 possible health statuses. There is also a 100 mm visual analog scale (VAS) with two reference ends that express the worst (0 equivalent to death) and best imaginable health status (100), wherein the patient indicates the perception of his own overall health. The third element of the EQ-5D is the index of social preference values, obtained for each health status from studies of the overall population. The index varies from 1 (best health status possible) to 0 (death), although negative values exist corresponding to health status considered as worse than death.
The American Spinal Injury Association scale assesses the most caudal segment with motor and with sensorial normal function (neurological level) and classifies the lesion in an impairment scale from A (complete) through B–D (incomplete) and E (normal). Incomplete lesions can be classified in a specific clinical syndrome (Hemisection of the spinal cord or Brown-Sequard, Central Cord, Anterior Cord, Posterior Cord, Conus Medullaris and Cauda Equina).
Statistics
Descriptive statistics were applied to all variables, including measures of central tendency and of statistical variability for quantitative variables, as well as absolute and relative frequencies for qualitative variables, with a bilateral confidence interval (CI) of 95%, as well as for all changes from baseline.
Student's t-test was used to compare pair-wise samples (data between two different time points) and Wilcoxon test was used in non-parametric distributions. Student's t-test was used to compare independent samples and Mann–Whitney test was used in non-parametric distributions. Analysis of variance was used to compare a continuous variable with a variable of more than two categories. The statistics program SPSS version 17.0 was used. The assessments were considered statistically significant when the two-sided P-value was <0.05.
Results
In all, 57 patients were included in the study and 54 were assessable, as three had neither follow-up data nor reason for withdrawal. In all, 48 (89%) patients completed the study; 4 out of the 6 patients who withdrew had no available data, as they did not take the analgesic treatment, and the other two suffered from adverse reactions (1 headache and hallucinations and 1 headache and dry mouth). Patients were treated with oxycodone in combination with anticonvuslants (83%) or alone (17%), in similar percentages at baseline and along the study (Table 1). Antiemetics and laxatives were used, depending on the time of assessment, from 22.2 to 31.3% and from 78.8 to 91.7% of patients, respectively (data not shown).
Baseline patients’ characteristics are described in Table 2. A total of 81.5% were men and the mean age was 46.4. The most frequent causes of injury were road traffic (25.9%) and industrial accidents (24.1%). 51.9% of patients had a dorsal lesion level and 50% had a complete lesion. Mean pain intensity (VAS) at baseline was 7.1±1.3. All patients showed NP with DN4 mean 4.7±2.1 and in 81.5% of patients NP was below level.20.4% of patients showed nociceptive pain, all of it musculoskeletal. The most frequent anticonvulsant treatment previously used was gabapentin (94.4%), mostly in combination with analgesics other than fentanyl. In all 52 patients changed the treatment and the most frequent motive was uncontrolled pain (94.4%), followed by somnolence (14.8%), gastrointestinal disorders (11.1%) and asthenia (1.9%).
Pain intensity (VAS: 7.1±1.3 at baseline to 4.3±1.7 at month 3 (Figure 1)) and Lattinen total score (13.2±3 at baseline to 7.7±3.4 at month 3 (Figure 2)) decreased significantly (P<0.001) from one visit to the next (Table 3). The percentage of patients suffering from irruptive pain crisis also decreased from 24.1% at 7 days to 13% at month 3 (Table 3). Only two patients increased their spasticity degree at 3 months compared with baseline, whereas most (79.2%) stayed the same and 16.7% decreased it (data not shown).

Pain evolution. Mean VAS and CI 95%.

Lattinen total score evolution. Mean (CI 95%).
No patient got worse regarding pain impact on the physical activity and on sleep (Lattinen scale). Although because of the sample distribution it was not possible to determine the statistical significance, 18.75% of patients showed same and 81.25% better physical activity, and 39.58% same and 60.42% better sleep at month 3 than at baseline Figure 3 shows increases in patients percentages with no or mild activity and sleep impairment and decreases of patients percentages with moderate or severe activity and sleep impairment at 3 months, as compared with baseline.

Pain impact on the physical activity and on sleep quality (Lattinen). Percentage of the patients at the baseline and at 3 months. Percentage over assessed patients at each time point.
Although EQ-5D VAS did not change significantly from the baseline to month 3 (54.19 (CI 95%: 47.39–60.98) to 62.60 (CI 95%: 56.98–68.23); P=0.061), there was a trend to increase, with a larger percentage of patients showing ‘no problems’ for each dimension at month 3 than at baseline (Table 4). At baseline 20.4% of patients showed the worst possible health status (code 33 333), whereas only 2.1% did at 3 months. The index of preference values increased significantly from baseline to month 3 (0.26 (CI 95%: 0.19–0.33) to 0.62 (CI 95%: 0.56–0.68); P<0.001) (Figure 4).

Quality of life evolution. Mean EQ-5D (preference index) and CI 95%.
No significant differences were found in pain intensity (VAS) or in Lattinen total score according to American Spinal Injury Association classification (in complete or incomplete lesion) or lesion level (data not shown). Neither did we observe any significant differences (P=0.093) in the pain VAS percentage decrease from baseline to month 3 among the three different previous anticonvulsant treatment groups (gabapentin + fentanyl ± other analgesics, pregabalin± other analgesics and gabapentin ± other analgesics).
The mean (CI 95%) VAS percentage change at day 7 with respect to baseline was −9.98 (−14.44; −5.53); at month 1 with respect to day 7: −10.8 (−15.24; −6.37); at month 2 with respect to month 1: −13.8 (−18.74; −8.87) and at month 3 with respect to month 2: −12.54 (−16.76; −12.54).
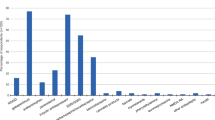
A safety analysis was performed in all 54 patients. In all, 29 (53.7%) patients showed at least one adverse event (AE) related to the analgesic treatment, with constipation being the most frequent one (33.3%) (Figure 5). No event was threatening to life or caused hospitalization. A total of patients (14.8% of total number of patients or 27.6% of patients with at least one AE) suffered from AEs related to anticonvulsants and 28 (51.9% of total patients and 96.6% of patients with at least one AE) from AEs related to opioids.

Adverse events. * Hallucinations.
Discussion
NP is common after SCI (20–75%), impacting greatly in the quality of life of these patients.2 Post-SCI NP is frequently refractory to treatment7, 8 and patients are dissatisfied with the level of knowledge that family physicians have of it16 and the pain control obtained.10 Oxycodone has shown to be effective in peripheral NP treatment11 and as concomitant treatment in central NP.12, 13 This study characterizes oxycodone treatment in SCI patients with refractory NP to assess its efficacy and help physicians to improve the management of this condition.
In all, 81.5% of patients were male and mean age was 46 years old in agreement with most of the studies, wherein more than two-third of the patients are male of middle or younger ages.1, 17, 18 The most frequent etiology was car accident, which is the most frequent cause of traumatic SCI in developed countries.1, 18 The level of the lesion was mainly dorsal, followed by cervical, as it was in a previous Spanish study by Mazaira et al.,1 and lesions were complete in 50% of cases, as traumatic SCI have a high risk to produce complete lesions. NP was mainly below level (81.5%), in contrast with the results of the study of Siddall et al.5 in 100 traumatic SCI patients, in which NP was roughly 50% at level and below level. The level or completeness of the lesion had no effect on pain intensity (VAS) or Lattinen score, in agreement with previous studies.5
Opioids have shown efficacy in the treatment of peripheral NP,19 with oxycodone showing level A evidence for postherpetic neuralgia and painful polyneuropathy and level B for trigeminal neuralgia.11 Siddall et al.20 suggested a weak opioid, or a tricyclic antidepressant, as second line treatment in NP SCI patients if gabapentin failed. In central NP studies resulting in treatment success, opioids, including oxycodone, were used with anticonvulsants as concomitant therapy.13 In our study, oxycodone treatment, 83% in different combinations with anticonvulsants, decreased pain intensity 39.3% (VAS percentage change) at month 3 with respect to the baseline.
EQ-5D VAS has been previously used to assess the evolution of overall health in patients with central NP submitted to treatment;13 in our study, there was a decrease in the percentage of patients who showed problems in mobility, self-care, usual activities, pain/discomfort and anxiety/depression (Table 4) and there was a trend (P=0.061) for improvement in the patients health self-perception. Also the index of preference values increased significantly from baseline to month 3 (0.26–0.62; P<0.001; Figure 4), which suggests that treatment with oxycodone, mostly in combination with anticonvulsants, improves the health-related quality of life of these patients. Patients also improved their physical activity and sleep (Lattinen scale) with the treatment administered.
Constipation and nausea, which were the most frequently reported AEs, are characteristic of opiod-treated patients. However, in contrast to the other studies using weak opioids, such as tramadol,9 in which there was a high withdrawal rate (43%) because of the AEs, in our study using oxycodone, although 54% patients showed at least one treatment-related AE, only two (3.7%) withdrew because of the AEs. In fact, in clinical trials of NP, the side effect profile of opioids has been reported to be good, particularly for oxycodone.11
Conclusion
These data suggest that oxycodone treatment, mostly in combination with anticonvulsants, in SCI patients with previous anticonvulsants refractory NP, decreases pain intensity and accordingly, improves health-related quality of life (assessed by EQ-5D) and diminishes the impact of pain on physical activity and sleep. The treatment is well tolerated with constipation as the main AE, which might be better controlled with newer laxative therapies.
References
Mazaira J, Labanda F, Romero J, Garcia ME, Gambarruta C, Sanchez A et al. Epidemiología de la lesión medular y otros aspectos. Rehabilitación 1998; 32: 365–372.
Baastrup C, Finnerup NB . Pharmacological management of neuropathic pain following spinal cord injury. CNS Drugs 2008; 22: 455–475.
Dijkers M, Bryce T, Zanca J . Prevalence of chronic pain after traumatic spinal cord injury: a systematic review. J Rehabil Res Dev 2009; 46: 13–29.
Ravenscroft A, Ahmed YS, Burnside IG . Chronic pain after SCI A patient survey. Spinal Cord 2000; 38: 611–614.
Siddall PJ, McClelland JM, Rutkowski SB, Cousins MJ . A longitudinal study of the prevalence and characteristics of pain in the first 5 years following spinal cord injury. Pain 2003; 103: 249–257.
Widerstrom-Noga EG, Felipe-Cuervo E, Yezierski RP . Chronic pain after spinal injury: interference with sleep and daily activities. Arch Phys Med Rehabil 2001; 82: 1571–1577.
Ragnarsson KT . Management of pain in persons with spinal cord injury. J Spinal Cord Med 1997; 20: 186–199.
Cardenas DD, Felix ER . Pain after spinal cord injury: a review of classification, treatment approaches, and treatment assessment. Pm R 2009; 1: 1077–1090 (Review).
Norrbrink C, Lundeberg T . Tramadol in neuropathic pain after spinal cord injury: a randomized, double-blind, placebo-controlled trial. Clin J Pain 2009; 25: 177–184.
Murphy D, Reid DB . Pain treatment satisfaction in spinal cord injury. Spinal Cord 2001; 39: 44–46.
Attal N, Cruccu G, Haanpaa M, Hansson P, Jensen TS, Nurmikko T et al. EFNS guidelines on pharmacological treatment of neuropathic pain. Eur J Neurol 2006; 13: 1153–1169.
Cohen SP, Abdi S . Venous malformations associated with central pain: report of a case. Anesth Analg 2002; 95: 1358–1360, Table of contents.
Vranken JH, Dijkgraaf MG, Kruis MR, van der Vegt MH, Hollmann MW, Heesen M . Pregabalin in patients with central neuropathic pain: a randomized, double-blind, placebo-controlled trial of a flexible-dose regimen. Pain 2008; 136: 150–157.
IASP. Classification of Chronic Pain Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms, 2nd edn. IASP task force on taxonomy: Seattle, 1994.
Siddall PJ, Yezierski RP, Loeser JD . Pain following spinal cord injury: Clinical features, prevalence, and taxonomy. IASP Newsletter 2000; 3: 3–7.
Norman C, Bender JL, Macdonald J, Dunn M, Dunne S, Siu B et al. Questions that individuals with spinal cord injury have regarding their chronic pain: A qualitative study. Disabil Rehabil 2010; 32: 114–124.
Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning M . A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord 2010; 48: 313–318, Epub 2009 Oct 13.
Pagliacci MC, Celani MG, Zampolini M, Spizzichino L, Franceschini M, Baratta S et al. An Italian survey of traumatic spinal cord injury. The Gruppo Italiano Studio Epidemiologico Mielolesioni study. Arch Phys Med Rehabil 2003; 84: 1266–1275.
Finnerup NB, Otto M, McQuay HJ, Jensen TS, Sindrup SH . Algorithm for neuropathic pain treatment: an evidence based proposal. Pain 2005; 118: 289–305.
Siddall PJ, Middleton JW . A proposed algorithm for the management of pain following spinal cord injury. Spinal Cord 2006; 44: 67–77.
Acknowledgements
We thank Almudena Pardo Mateos for writing the first draft of the paper and Nuria Pajuelo for performing the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Barrera-Chacon, J., Mendez-Suarez, J., Jáuregui-Abrisqueta, M. et al. Oxycodone improves pain control and quality of life in anticonvulsant-pretreated spinal cord-injured patients with neuropathic pain. Spinal Cord 49, 36–42 (2011). https://doi.org/10.1038/sc.2010.101
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.101
Keywords
This article is cited by
-
Neuropathic Pain and Spinal Cord Injury: Management, Phenotypes, and Biomarkers
Drugs (2023)
-
Central Neuropathic Pain Syndromes: Current and Emerging Pharmacological Strategies
CNS Drugs (2022)
-
The CanPain SCI clinical practice guidelines for rehabilitation management of neuropathic pain after spinal cord injury: 2021 update
Spinal Cord (2022)
-
Empfehlungen der zweiten Aktualisierung der Leitlinie LONTS
Der Schmerz (2020)
-
Are Opioids Effective in Relieving Neuropathic Pain?
SN Comprehensive Clinical Medicine (2019)
