
Abstract
Study design:
Retrospective follow-up study.
Objectives:
To assess the occurrence of bladder stones in patients with spinal cord injury (SCI).
Setting:
Single SCI rehabilitation center in Switzerland.
Methods:
We searched our database for SCI patients who had undergone surgery due to bladder stones between 2004 and 2012. In all patients retrieved, personal characteristics, bladder management, bladder stone occurrence and time to stone formation/recurrence were recorded.
Results:
We identified 93 (3.3%) of 2825 patients with bladder stones, 24 women and 69 men, with a mean age 50 years (17–83) years. We observed bladder stones in patients with suprapubic catheter (SPC) in 11% (50/453), transurethral catheter (TC) in 6.6% (5/75), with intermittent catheterization (IC) in 2% (27/1315) and with reflex micturition (RM) in 1.1% (11/982), respectively. The mean time period to stone development was 95 months. The TC group had the shortest time interval (31 months), followed by the SPC group (59 months), individuals performing IC (116 months) and RM (211 months), respectively. Bladder stone recurrence rate was 23%. Recurrences were most frequent in the TC group (40%), followed by SPC (28%) and IC (22%), whereas no recurrences occurred in the RM group. Time to recurrence was shortest in the SPC group (14 months), followed by the IC (26 months) and the TC group (31 months), respectively.
Conclusion:
In SCI patients, bladder management has an important role in the development of bladder stones. Indwelling catheters (TC/SPC) are associated with the highest risk to develop bladder stones and therefore should be avoided if possible. If unavoidable, SPC are superior to TC.
Similar content being viewed by others

Introduction
After spinal cord injury (SCI), the loss of sensory and motor function can lead to secondary urologic complications, such as neurogenic lower urinary tract dysfunction (NLUTD).1 NLUTD is associated with the risk for several urologic complications including renal failure, bladder cancer, urinary tract infection, incontinence, and morphologic alterations of bladder and urethra.2
In addition, bladder stones are a frequent complication of NLUTD. Generally, the risk to develop bladder stones is increased due to recurrent urinary tract infections with urease-producing organisms, incomplete bladder emptying, and use of permanent catheters, immobilization and hypercalcuria.3, 4 Bladder stones can cause recurrent urinary tract infections, hematuria, and catheter blockage and bladder irritation with autonomic dysreflexia in SCI patients with a level of injury above T6.5
The optimal bladder management should prevent secondary complications and ensure patients quality of life.6 Today, modern bladder management has substantially reduced morbidity and mortality of NLUTD. Therefore, the number of bladder stones should be substantially reduced in SCI patients with state of the art bladder management7 compared with patients with indwelling catheters. This study aims to determine the occurrence of bladder stones and the possible association with the type of bladder management in SCI patients.
Materials and methods
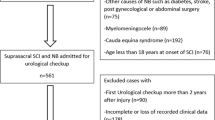
In a retrospective study, the charts of all SCI patients treated at our institution between 2004 and 2012 were reviewed to identify those with bladder stones.
In general, we found bladder stones in regular yearly follow-up, by ultrasound or videourodynamics. In symptomatic patient, we performed ultrasound immediately. If there were some unclear findings we performed cystoscopy. All bladder stones were treated by endoscopic lithotrypsy, without open surgery under general anesthesia. We excluded sludge from the study, which could be ‘washed out’ during cystoscopy.
If patient changed their method of bladder emptying and new yearly follow-up showed a stone, then we associated the stone to this new method. Patients were excluded if they were lost to follow-up or underwent major urologic surgery (augmentation, Brindley stimulation), at all 14.7% patients (487/3312) were excluded. We included all patients with bladder stones that required a surgical procedure for stone treatment. Demographic characteristics and clinical features were investigated.
Each patient was categorized by bladder management, such as intermittent catheterization (IC), reflex micturition (RM), suprapubic catheter (SPC) and transurethral catheter (TC).
We evaluated the association between bladder management and bladder stone occurrence, time to stone formation and time to stone recurrence.
The study had been approved by the local ethical committee.
Results
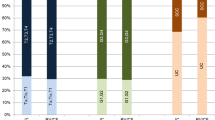
From the 3312 SCI patients in our database between 2004 and 2012, 2825 patients were included in our analysis and 93 SCI patients were diagnosed with bladder stones requiring surgical removal. Table 1 gives an overview about demographic and clinical features. Bladder stone occurred three times more in male than in female. Patients with bladder stone with cervical and thoracic lesion emptied there bladder mostly by SPC and TC (52/93) as against IC and RM (31/93). We found mostly yellow compact stones. All our analyzed stones consist of struvite or apatite stones, which can be classified as infect-related stones and in 20% with small part of calcium-oxalat. Overall, SCI patients emptied their bladder between 2004 and 2012 by IC 46.5% (1315/2825), RM 34.8% (982/2825), SPC 16.0% (453/2825) and TC 2.6% (75/2825). Bladder stones occurred in 2.8% of the patients. We observed bladder stone by SPC in 11% (n=50/453), by TC in 6.6% (n=5/75), by IC in 2% (n=27/1315) and by RM in 1.1% (n=11/982), respectively (Table 2). We detected more bladder stones in SCI patients using indwelling catheters like SPC and TC 10.4% (55/528) than without using like IC and RM 1.65% (38/2297).
The shortest period to stone development was found in patients with TC 31 (5–84) months and with SPC 59 (2–199) months, the longest time interval was found in patients performing IC 116 (2–480) months and RM 211 (7–606) months (Table 3).
We observed a bladder stone recurrence rate of 23% after 19 (2–79) months, most frequently in the TC group (40%), followed by the SPC group (28%) and patients with IC (22%), whereas no recurrence was found in patients with RM. The shortest time to recurrence was detected in the SPC group 14 (2–48) months, followed by persons on IC 26 (4–79) months and patients with TC 31 (3–60) months (Table 4).
Discussion
Bladder stones are a common urological complication in patients with NLUTD.4 Nevertheless, data in literature are contradictory. Linsenmeyer et al.5 noted that bladder stones are the second most frequent urological complication in patients with SCI. Chen et al.8 observed that the 5-year cumulative incidence rate of an initial bladder stone decreased from 29% (1973–1977) to 8% (1992–1996).
The incidence of bladder stones varies depending on the bladder management. Particularly indwelling catheters are associated with a higher risk of stone formation. Ord et al.9 reported an absolute annual risk of bladder stone formation in SCI patients with indwelling catheters of 4% compared with a rate of 0.2% for those on intermittent self-catheterization. The bladder stone incidence was not significantly different between patients with suprapubic or urethral catheters.10, 11 Ku et al.12 determined that bladder stones were more common in patients with urethral catheters than in those without. Hansen et al.13, however, did not detect significant differences regarding bladder stone formation between the different bladder-emptying methods.
De Vivo et al.14 estimated that 36% of patients with indwelling catheters develop bladder stones within 8 years. Nagashima et al.15 found that indwelling catheters for longer than a month were a risk factor for bladder stone formation in SCI patients.
Our study demonstrated bladder stone by SPC in 11%, by TC in 6.6%, by IC in 2% and by RM in 1.65%. We can conclude that bladder stones in SCI patients used indwelling catheters like SPC and TC more common (10.4%) than without, using like IC and RM (1.1%).
In addition, the development of bladder stones in SCI patients seems to depend on the duration of SCI. Hansen et al.13 described the highest risk for bladder stones within the first 6 months post-injury. According to De Vivo et al.14, bladder calculi were most likely to develop within the first year after injury and in younger patients within 2 years of hospital discharge. We found a low occurrence of bladder stones in our patients (2.8%), which, however, increased in the last years. One possible explanation is the aging of the SCI patients that we followed up, which, because of the increasing morbidity of the ageing persons, leads to a higher rate of bladder management with indwelling catheters. This must be taken into account when following up SCI patients in order to early identify and to avoid complications by bladder stones.3
The retrospective nature is one of the major drawbacks of our study, as it did not allow evaluating the incidence and the causative organisms of urinary tract infections in the patients with bladder stone formation. As all patients presented with urinary tract infection at the time of stone surgery, it is virtually impossible to state if these infection were cause or consequence of the bladder stones, as it is well known that urinary tract infections, especially with urease-producing bacteria, may lead to stone formation. Our stone analysis showed 100% infect-related stones supported that in case of recurrent urinary tract infections a stone must be excluded. As >70% of all SCI patients present with significant bacteriuria16 and in 92.8% in patients with SPC irrespective of bladder stone formation.17 The impact of chronic bacteriuria on stone formation should be assessed in a prospective study. In addition, we did not evaluate other important risk factors for the development of bladder stones in SCI patients, like immobilization or hypercalcuria. Another limit of our study was that each patient was categorized by a predominant bladder management, defined as the method used for the majority of time since injury with a minimum of 1 year.
If a SCI patient already had a bladder stone, the risk for recurrence is increased. Reasons for this may be pre-existing risk factors,3, 4 in particular bladder management, that were not altered after removal of the bladder stone. Hansen et al.13 found that during follow-up 14% had at least one episode of bladder stone recurrence. Those patients not having suffered from bladder calculi within the first 2 years after SCI have a 5% risk of stone formation during the following 43 years. Ord et al.9 described a 16% risk for stone recurrence per year. In our study, bladder stone recurrence occurred in 23%, most common in patients with indwelling catheters, most frequent in those with TC, followed by those with SPC. Bladder stones recurred twice as fast in the SPC group than in the TC group.
These data suggest that an optimized bladder management, without indwelling catheters, can aid in preventing recurrence of bladder stones in SCI patients.
Conclusion
In SCI patients, bladder management has an important role regarding the development of bladder stones. Therefore, indwelling catheters should be avoided if possible. An optimized bladder management seems to be associated with a low occurrence of bladder stones in SCI patients.
Data archiving
There were no data to deposit.
References
Yezierski RP . Review spinal cord injury pain: spinal and supraspinal mechanisms. J Rehabil Res Dev 2009; 46: 95–107.
Gormley EA . Urologic complications of the neurogenic bladder. Urol Clin North Am 2010; 37: 601–607.
Ost MC, Lee BR . Review urolithiasis in patients with spinal cord injuries: risk factors, management, and outcomes. Curr Opin Urol 2006; 16: 93–99.
Grima F, Chartier-Kastler E, Ruffion A . Surgical management of bladder stones in neurogenic bladder. Prog Urol 2007; 17: 465–469.
Linsenmeyer TA, Stone JM, Stein S . Neurogenic bladder and bowel dysfunction. In: DeLisa JA (eds).. Rehabilitation Medicine Principles and Practice 4th edn Lippincott-Raven: Philadelphia, PA, pp 1619–1653 2004.
Weld KJ, Dmochowski RR . Effect of bladder management on urological complications in spinal cord injured patients. J Urol 2000; 163: 768–772.
Stöhrer M, Blok B, Castro-Diaz D, Chartier-Kastler E, Del Popolo G, Kramer G et al. EAU guidelines on neurogenic lower urinary tract dysfunction. Eur Urol 2009; 56: 81–88.
Chen Y, DeVivo MJ, Lloyd LK . Bladder stone incidence in persons with spinal cord injury: determinants and trends, 1973-1996. Urology 2001; 58: 665–670.
Ord J, Lunn D, Reynard J . Bladder management and risk of bladder stone formation in spinal cord injured patients. J Urol 2003; 170: 1734–1737.
Favazza T, Midha M, Martin J, Grob BM . Factors influencing bladder stone formation in patients with spinal cord injury. J Spinal Cord Med 2004; 27: 252–254.
Katsumi HK, Kalisvaart JF, Ronningen LD, Hovey RM . Urethral versus suprapubic catheter: choosing the best bladder management for male spinal cord injury patients with indwelling catheters. Spinal Cord 2010; 48: 325–329.
Ku JH, Jung TY, Lee JK, Park WH, Shim HB . Risk factors for urinary stone formation in men with spinal cord injury: a 17-year follow-up study. BJU Int 2006; 97: 790–793.
Hansen RB, Biering-Sørensen F, Kristensen JK . Urinary calculi following traumatic spinal cord injury. Scand J Urol Nephrol 2007; 41: 115–119.
DeVivo MJ, Fine PR, Cutter GR, Maetz HM . The risk of bladder calculi in patients with spinal cord injuries. Arch Intern Med 1985; 145: 428–430.
Nagashima M, Taziri T, Tanaka K . A clinical study of bladder stone with spinal cord injury in subacute stage. Hinyokika Kiyo 2008; 54: 647–650.
Ryu KH, Kim YB, Yang SO, Lee JK, Jung TY . Results of urine culture and antimicrobial sensitivity tests according to the voiding method over 10 years in patients with spinal cord injury. Korean J Urol 2011; 52: 345–349.
Pannek J, Göcking K, Bersch U . To clamp or not to clamp? Bladder management by suprapubic catheterization in patients with neurogenic bladder dysfunction. World J Urol 2010; 28: 637–641.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Bartel, P., Krebs, J., Wöllner, J. et al. Bladder stones in patients with spinal cord injury: a long-term study. Spinal Cord 52, 295–297 (2014). https://doi.org/10.1038/sc.2014.1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.1
Keywords
This article is cited by
-
Squamous cell carcinoma of the renal pelvis in a patient with long-term spinal cord injury—a case report
Spinal Cord Series and Cases (2021)
-
Surveillance and management of urologic complications after spinal cord injury
World Journal of Urology (2018)
-
Influence of bladder lithiasis on lower urinary tract dynamics in patients with spinal cord injury
Spinal Cord (2017)
