
Abstract
Study design:
Systematic review about randomised trials comparing different training strategies to improve gait in people with spinal cord injuries (SCI).
Objectives:
The aim of this systematic review was to compare the effectiveness of body-weight-supported treadmill training (BWSTT) and robotic-assisted gait training with overground gait training and other forms of physiotherapy in people with traumatic SCI.
Setting:
Systematic review conducted by researchers from Germany and Australia.
Methods:
An extensive search was conducted for randomised controlled trials involving people with traumatic SCI that compared either BWSTT or robotic-assisted gait training with overground gait training and other forms of physiotherapy. The two outcomes of interest were walking speed (m s−1) and walking distance (m). BWSTT and robotic-assisted gait training were analysed separately, and data were pooled across trials to derive mean between-group differences using a random-effects model.
Results:
Thirteen randomised controlled trials involving 586 people were identified. Ten trials involving 462 participants compared BWSTT to overground gait training and other forms of physiotherapy, but only nine trials provided useable data. The pooled mean (95% confidence interval (CI)) between-group differences for walking speed and walking distance were −0.03 m s−1 (−0.10 to 0.04) and −7 m (−45 to 31), respectively, favouring overground gait training. Five trials involving 344 participants compared robotic-assisted gait training to overground gait training and other forms of physiotherapy but only three provided useable data. The pooled mean (95% CI) between-group differences for walking speed and walking distance were −0.04 m s−1 (95% CI −0.21 to 0.13) and −6 m (95% CI −86 to 74), respectively, favouring overground gait training.
Conclusions:
BWSTT and robotic-assisted gait training do not increase walking speed more than overground gait training and other forms of physiotherapy do, but their effects on walking distance are not clear.
Similar content being viewed by others

Introduction
Many different treatment strategies are advocated to improve the gait of people with spinal cord injuries (SCI).1, 2, 3, 4 Overground gait training has been the predominant approach until recent years when the emphasis shifted to other forms of locomotor training. This includes body-weight-supported treadmill training (BWSTT) and robotic-assisted gait training with or without functional electrical stimulation (FES) and manual guidance. Despite early reports suggesting promising results from these types of locomotor training programmes,4, 5 it is not clear whether they are superior to overground gait training and other forms of physiotherapy.
We conducted a Cochrane Systematic Review in 2012 to investigate the effectiveness of different gait training strategies.1 At the time, we concluded that the relative effectiveness of different locomotor training approaches was not clear, and there was no evidence to indicate that any one approach was superior to another. However, since this review, there have been a growing number of clinical trials and increasing uncertainty about the effectiveness of these interventions.6, 7, 8, 9 The aim, therefore, of this review was to update our 2012 review. Specifically, we sought to compare the effectiveness of BWSTT and robotic-assisted gait training with overground gait training and other forms of physiotherapy on walking speed and walking distance in people with traumatic SCI. Hence, the two comparisons of interest were as follows:
-
Comparison no. 1: BWSTT versus overground gait training and other forms of physiotherapy (not including robotic-assisted gait training)
-
Comparison no. 2: Robotic-assisted gait training versus overground gait training and other forms of physiotherapy (not including BWSTT)
Materials and methods
Trials that met the following inclusion criteria were included:
Types of trials
Randomised controlled trials of parallel-groups or cross-over trials. Only the first period of cross-over trials was analysed.
Participants
Participants of any age and gender and any type of traumatic SCI regardless of time since injury or level of initial walking ability.
Interventions and comparisons
Trials that compared:
-
Comparison no. 1: BWSTT versus overground gait training and other forms of physiotherapy (not including robotic-assisted gait training)
-
Comparison no. 2: Robotic-assisted gait training versus overground gait training and other forms of physiotherapy (not including BWSTT)
BWSTT included treadmill gait training with body-weight support, manual guidance, FES or some additional overground gait training. Robotic-assisted gait training included gait training with automated electromechanical devices or robotic devices with or without body-weight support, manual guidance, FES or some additional overground gait training. Overground gait training included gait training that involved moving across the floor with or without body-weight support (for example, with the use of a fixed track or moving overhead walking frame), FES, orthoses, aids or manual assistance. Other forms of physiotherapy were also grouped with overground gait training. This included generic physiotherapy programmes that may have included strength and fitness training exercises. It did not include any passive interventions that did not require a participant to actively contract their lower limb muscles (for example, muscle stretching). In trials with three or more groups, consideration was given to collapsing two or more groups into one group. For example, in trials that provided BWSTT in two different ways, the results of the two groups were collapsed into one group reflecting BWSTT, provided there was a third group that included either overground gait training or another form of physiotherapy. In trials that compared BWSTT, robotic-assisted gait training and overground gait training groups, the results of the BWSTT and robotic groups were separately included in the two comparisons of interest.
Outcomes
The two outcomes of interest were walking speed or walking distance. Walking speed could be measured in any way but was typically measured using the 10- or 15-m walk test. These data were expressed in metres per second (m s−1). Walking distance was defined as the distance to walk a set distance in 6 min, expressed in metres. In trials that measured distance walked in 2 min (instead of 6 min), the data were multiplied by three to enable pooling. Tests that captured either fastest or casual walking speed were accepted and assistance of either another person or walking aids was ignored. If participants were unable to walk with assistance, their walking speed and walking distance was entered into the analyses as zero. If trials measured walking speed or walking distance in more than one way, then the review authors independently identified the most appropriate measure and resolved any differing opinions through discussion. In trials that measured walking speed or walking distance at more than one end point (for example, trials that measured at 6 weeks and 6 months), then measurements taken at the end of the intervention were used.
Adverse events
Data on adverse events were also extracted. This included any unwarranted or deleterious event for either patient or therapist. Adverse events included thrombosis, major cardiovascular events, injuries (for example, injurious falls or other injuries), pain or any other reported adverse event that occurred during the study period.
Search strategy
The same systematic search strategy as previously published in the protocol for our original systematic review1 was used to identify published, unpublished and ongoing trials. The searches were last updated in September 2016 and were not restricted by language or date.
Data collection and analysis
Two authors (JM and BE) independently examined titles and abstracts of citations identified through the search strategy. The full text of all potentially relevant trials was then retrieved and two authors (JM and ST) independently assessed the trials for inclusion against the pre-defined criteria. Disagreements were resolved through discussion with all review authors. If further trial information was needed, the authors of the original trial were contacted if possible in an effort to obtain missing data.
Assessment of risk of bias
Three items from the Cochrane Risk of Bias Tool were used to assess the risk of bias of each trial. Each item was rated as high risk, low risk or unclear risk. The three items captured the method used to generate the random sequence (selection bias), and the use of concealed allocation (selection bias) and blinded assessors (detection bias).
Data extraction
Two authors (JM and ST) independently extracted data from the included trials. This included data to describe the study, participants and intervention, as well as data for walking speed and walking distance. Any differences were arbitrated by a third author (BE). Data from unpublished trials and trials, which did not provide sufficient information were attained from the authors where possible.
Data synthesis
Data for the gait outcomes were pooled into four meta-analyses if the trials were similar and if there was not excessive clinical or statistical heterogeneity. A random-effects model was used for each meta-analysis to provide a conservative estimate of treatment effectiveness. For each meta-analysis, an overall mean difference (MD) and 95% confidence interval (CI) was calculated because all trials in each analysis used a comparable scale. The approach of Wan et al.10 was used to impute missing mean and s.d. from median and interquartile ranges. Data for the adverse events were pooled into two meta-analyses to determine risk differences and 95% CI. The number of participants in each meta-analysis corresponds with the number of participants randomised, not the number of participants included in the analysis of the published trials. This assumed that all missing data were missing at random. All statistical analyses were conducted using The Cochrane Collaboration's Review Manager software RevMan Version: 5.3.5.11
Results
Characteristics of included trials
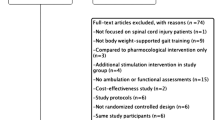
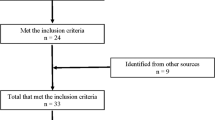
The search identified 1312 unique records. Sixty three full-text articles were assessed for eligibility. Two potentially eligible trials involving robotic-assisted gait training were excluded because the comparison was either no intervention12 or a home passive stretching intervention.13 Another potentially eligible trial14 was excluded because it appeared to include data of at least some participants from a similar trial from the same set of authors, which was included in the review.15 Ultimately, 13 randomised controlled trials involving 586 patients met our inclusion criteria and were included in the analysis.15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27 This included eight new trials since our 2012 Cochrane review.15, 19, 21, 22, 24, 25, 26, 27 Three trials used a cross-over design21, 23, 27 and the other seven trials used a parallel group design. The details of the included trials are described in Table 1. Three trials did not provide useable data for any of the meta-analyses.21, 25, 26 Additional data were obtained from authors for three trials;17, 20, 27 one was an unpublished trial.20
Risk of bias of included trials
The results from our assessment of the risk of bias for each trial are shown in Figure 1. Six trials were rated as low risk of bias for random sequence generation, five trials were rated as low risk of bias for concealed allocation and eight trials were rated as low risk of bias for blinding of assessors. Two and five trials were rated as high risk of bias for concealed allocation and blinding of assessors, respectively.

Risk of bias of each trial from the method of generating the random number sequence; concealing allocation; and blinding assessors are shown where green indicates a low risk of bias, yellow indicates an unclear risk of bias and red indicates a high risk of bias. A full colour version of this figure is available at the Spinal Cord journal online.
Participants
The number of participants in each trial ranged from 921 to 146.17 The mean age of the participants was 37 years and ranged from 1617 to 6817 years, with more men (n=404) than women (n=96). All trials provided information on the level of SCI (C1–L4) and baseline severity (ASIA impairment Scale (AIS) grades A–D).
The training
Five trials examined robotic-assisted gait training,15, 18, 20, 21, 26 10 trials examined BWSTT,16, 17, 18, 22, 23, 24, 25, 27 and 2 trials examined both robotic-assisted gait and BWSTT training.18, 20 In most but not all trials, the groups receiving BWSTT and robotic-assisted gait training also received some general rehabilitation often including other forms of physiotherapy. Importantly, these types of additional therapies did not involve gait training and were provided to all groups in the trial. All but one trial21 in the comparison group received some type of overground training typically in combination with a generic physiotherapy programme of strengthening, stretching and fitness exercises. Treatments were provided between two22 and five times a week15, 17, 18, 23, 27 for 421, 23, 26–16 weeks.19 Each treatment lasted between 2523 and 60 min15, 16, 17, 24, and there was no difference in the dosage of gait training provided to groups within a trial.
Main findings
Comparison no. 1: BWSTT versus overground gait training and other forms of physiotherapy
Ten trials with a total of 462 participants included at least two groups that compared BWSTT with overground gait training (or some other form or physiotherapy; Table 2). BWSTT was provided in various ways including with overhead weight suspension, FES and manual guidance.
Walking speed
Nine trials involving 375 participants compared BWSTT with overground gait training (or some other form or physiotherapy), measured walking speed in m s−1 and provided useable data. The pooled MD was −0.03 m s−1 favouring overground gait training (95% CI, −0.10 to 0.04; P=0.37; I2=0%; Figure 2). The upper end of the 95% CI (that is, 0.04 m s−1) indicates that the treatment effect would not be >0.04 m s−1. Few clinicians or patients would consider a possible increase of 0.04 m s−1 as clinically meaningful. Therefore, these results indicate that BWSTT does not have clinically important effects on walking speed when compared to overground gait training.

Results of the meta-analysis for comparison no. 1 comparing body-weight-supported treadmill training with overground gait training and other forms of physiotherapy on walking speed (m s−1). Risk of bias from (A) the method of generating the random number sequence; (B) concealing allocation; and (C) blinding assessors are shown where green indicates a low risk of bias, yellow indicates an unclear risk of bias and red indicates a high risk of bias. The data from Dobkin et al.17 were not in the published paper but were provided by the author/s and as published in the Mehrholz Cochrane Review of 2012.1 The study by Hornby et al.20 was not published, and the data were provided by the author/s and as published in the Mehrholz Cochrane Review of 2012.1 The data from Yang et al.27 were provided by the author/s. A full colour version of this figure is available at the Spinal Cord journal online.
Walking distance
Eight trials involving a total of 335 participants measured walking distance and provided useable data. The pooled MD was −7 m favouring overground gait training (95% CI −45 to 31; P=0.73; I2=71%; Figure 3). The upper end of the 95% CI (that is, 31 m) indicates that the treatment effect may be as large as 31 m. Most would consider a possible increase of 31 m as clinically meaningful. Therefore, these results indicate that BWSTT may have clinically important effects on walking distance when compared to overground gait training, but these results are not certain because the 95% CI spans down to −45 m, favouring overground training.

Results of the meta-analysis for comparison no. 1 comparing body-weight-supported treadmill training with overground gait training and other forms of physiotherapy on walking distance (m). Risk of bias from (A) the method of generating the random number sequence; (B) concealing allocation; and (C) blinding assessors are shown, where green indicates a low risk of bias, yellow indicates an unclear risk of bias and red indicates a high risk of bias. The data from Dobkin et al.17 were not in the published paper but were provided by the author/s and as published in the Mehrholz Cochrane Review of 2012.1 The study by Hornby et al.20 was not published and the data were provided by the author/s and as published in the Mehrholz Cochrane Review of 2012.1 The data from Yang et al.27 were provided by the author/s. A full colour version of this figure is available at the Spinal Cord journal online.
Adverse events
Five trials involving a total of 309 participants provided information about adverse events. The rates of adverse events was between 0 (three studies) and 4%. The risk difference (95% CI) of an adverse event was 0.03 (−0.01 to 0.07; P=0.21; I2=0%; figure not included).
Comparison no. 2: robotic-assisted gait training versus overground gait training and other forms of physiotherapy
Five trials with a total of 344 participants included at least two groups, which compared robotic-assisted gait training with overground gait training (or some other form or physiotherapy; Table 3). Robotic-assisted gait training was provided in various ways including with overhead body-weight support and on a treadmill.18
Walking speed
Three trials involving 141 participants measured walking speed and provided useable data. The pooled MD was −0.04 m s−1 favouring overground gait training (95% CI −0.21 to 0.13; P=0.66; I2=57%; Figure 4). The upper end of the 95% CI (that is, 0.13 m s−1) indicates that the treatment effect would not be >0.13 m s−1. Few would consider a possible increase of 0.13 m s−1 as clinically meaningful. Therefore, these results indicate that robotic-assisted gait training does not have clinically important effects on walking speed when compared to overground gait training.

Results of the meta-analysis for comparison no. 2 comparing robotic-assisted gait training with overground gait training and other forms of physiotherapy on walking speed (m s−1). Risk of bias from (A) the method of generating the random number sequence; (B) concealing allocation; and (C) blinding assessors are shown where green indicates a low risk of bias, yellow indicates an unclear risk of bias and red indicates a high risk of bias. The study by Hornby et al.20 was not published and the data were provided by the author/s and as published in the Mehrholz Cochrane Review of 2012.1 A full colour version of this figure is available at the Spinal Cord journal online.
Walking distance
Three trials trial involving 141 participants measured walking distance and provided useable data. The pooled MD was −6 m favouring overground gait training (95% CI −86 to 74; P=0.88; I2=68%; Figure 5). The upper end of the 95% CI (that is, 74 m) indicates that the treatment effect may be as large as 74 m. Most would consider a possible increase of 74 m as clinically meaningful. Therefore, these results indicate that robotic-assisted gait training may have clinically important effects on walking distance when compared to overground gait training, but these results are not certain because the 95% CI spans down to −86 m, favouring overground training.

Results of the meta-analysis for comparison no. 2 comparing robotic-assisted gait training with overground gait training and other forms of physiotherapy on walking distance (m). Risk of bias from (A) the method of generating the random number sequence; (B) concealing allocation; and (C) blinding assessors are shown where green indicates a low risk of bias, yellow indicates an unclear risk of bias and red indicates a high risk of bias. The study by Hornby et al.20 was not published, and the data were provided by the author/s and as published in the Mehrholz Cochrane Review of 2012.1 A full colour version of this figure is available at the Spinal Cord journal online.
Adverse events
Four trials involving a total of 136 participants provided information about adverse events during the trial period. The risk difference (95% CI) of an adverse event was 0.01 (−0.06 to 0.08; P=0.79; I2=0%; figure not included).
Discussion
The aim of this review was to compare the effectiveness of BWSTT and robotic-assisted gait training with overground gait training and other forms of physiotherapy on walking speed and walking distance in people with traumatic SCI. Our results indicate that neither BWSTT nor robotic-assisted gait training increases walking speed more than overground gait training and other forms of physiotherapy. These results cannot be dismissed on the basis of an insufficient sample size or insufficient number of trials. The only grounds for caution are whether readers consider a possible increase in walking speed of 0.04 and 0.13 m s−1 as sufficiently meaningful to justify the additional cost of BWSTT and robotic-assisted gait training, respectively, in which case our results are inconclusive. Our results for walking distance fail to rule out the possibility that BWSTT or robotic-assisted gait training improve walking distance more than overground gait training and other forms of physiotherapy do. This interpretation assumes that possible increases in walking distance of 31 (for BWSTT) or 74 m (for robotic-assisted gait training) in 6 min justify the cost of BWSTT and robotic-assisted gait training.
The interpretation of our results rely on articulating a minimally worthwhile treatment effect for walking speed and walking distance. The size of the minimally worthwhile treatment effect for each outcome is ambiguous. It depends on the time, cost, inconvenience and potential for harm (to both patients and therapists) of BWSTT, robotic-assisted gait training and overground gait training.28 These need to be weighed up against the functional implications of any therapeutic effects. Decisions about minimally worthwhile treatment effects therefore vary from country to country, and person to person. For example, in less wealthy countries, the benefits of BWSTT and robotic-assisted gait training may need to be substantially higher than overground gait training to justify the additional cost of BWSTT and robotic devices. Similarly, some people with SCI and their therapists may value any improvement in gait regardless of how small it may be. There is no one answer that is appropriate for all. This makes the interpretation of our results complex.
Most of the trials included in our systematic review were vulnerable to bias. For example, only three trials were rated as low risk of bias for random sequence generation, concealed allocation and blinding of assessors. The other trials had high or unclear risk of bias for one, two or three of these items. Bias tends to inflate the relative effectiveness of BWSTT and robotic-assisted gait training compared to overground gait training.29 Therefore, our point estimates are probably overly conservative favouring BWSTT and robotic-assisted gait training. Future trials need to pay particular attention to methodological quality to ensure that their results are not biased.
The dosage of training differed markedly between trials. For example, some trials provided BWSTT for 4 weeks while others provided it for 16 weeks. Similarly, some treatment sessions were 25 min while others were 60 min. It is not unreasonable to believe that the effectiveness of BWSTT and robotic-assisted gait training may be dependent on dosage and that some trials may have provided an insufficient dosage. However, and importantly, all trials provided the same dosage of treatment to all groups in their trials. Therefore, if the dosage of BWSTT or robotic-assisted gait training was insufficient then so too was the dosage of overground gait training. Therefore, the inclusion of trials with low dosages of treatment would not have systematically biased the results one way or the other although they may have decreased the precision of the pooled estimate.
There is always the possibility that certain types of participants respond better to an intervention than other types of participants. This may also be the case for BWSTT and robotic-assisted gait training. For example, perhaps those with AIS C or AIS D lesions respond better to BWSTT and robotic-assisted gait training than those with AIS A or AIS B lesions, or perhaps those with more recent injuries respond better than those with more established injuries. However, there were insufficient trials and participants to conduct subgroup analyses, and results of subgroup analyses are often difficult to interpret.30
A limitation of this systematic review is our assumption that the missing data in the included trials were missing at random.31 If this is not the case then our point estimates are overly precise because our four meta-analyses are based on the number of participants randomised to groups rather than the number of participants who completed the trials.32 However, our conclusions are robust to this assumption. Another limitation of our systematic review is that we were forced to extrapolate data from one study from distance walking in 2 min to distance walked in 6 min. This may have introduced error but it is unlikely that this analytic strategy introduced bias or distorted the between-group differences.
In summary, the results of this review indicate that BWSTT and robotic-assisted gait training do not increase walking speed more than overground gait training and other forms of physiotherapy do. These results are robust despite the inclusion of trials with high susceptibility to bias unless readers value a possible treatment effect as small as 0.13 m s−1. Future trials are most unlikely to change these conclusions, and we therefore do not recommend further research on this particular issue. In contrast, our results fail to rule out a possible treatment effect on walking distance. Future trialists could try to clarify this issue although it will be hard to justify BWSTT or robotic-assisted gait training on the basis of increased walking distance without accompanying increases in walking speed.
References
Mehrholz J, Kugler J, Pohl M . Locomotor training for walking after spinal cord injury. Cochrane Database Syst Rev 2012, CD006676.
Harvey L Management of Spinal Cord Injuries: a Guide for Physiotherapists. Elsevier: London, UK, 2008.
Harkema SJ . Neural plasticity after human spinal cord injury: application of locomotor training to the rehabilitation of walking. Neuroscientist 2001; 7: 455–468.
Behrman AL, Harkema SJ . Locomotor training after human spinal cord injury: a series of case studies. Phys Ther 2000; 80: 688–700.
Wirz M, Zemon DH, Rupp R, Scheel A, Colombo G, Dietz V et al. Effectiveness of automated locomotor training in patients with chronic incomplete spinal cord injury: a multicenter trial. Arch Phys Med Rehabil 2005; 86: 672–680.
Dobkin BH, Duncan PW . Should body weight-supported treadmill training and robotic-assistive steppers for locomotor training trot back to the starting gate? Neurorehabil Neural Repair 2012; 26: 308–317.
Morawietz C, Moffat F . Effects of locomotor training after incomplete spinal cord injury: a systematic review. Arch Phys Med Rehabil 2013; 94: 2297–2308.
Harvey LA, Glinsky JV, Bowden JL . The effectiveness of 22 commonly administered physiotherapy interventions for people with spinal cord injury: a systematic review. Spinal Cord 2016; 54: 914–923.
Wolpaw JR . Treadmill training after spinal cord injury: good but not better. Neurology 2006; 66: 466–467.
Wan X, Wang W, Liu J, Tong T . Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014; 14: 135.
Review Manager (RevMan). The Nordic Cochrane Centre. The Cochrane Collaboration: Copenhagen, Denmark, 2015..
Niu X, Varoqui D, Kindig M, Mirbagheri MM . Prediction of gait recovery in spinal cord injured individuals trained with robotic gait orthosis. J Neuroeng Rehabil 2014; 11: 42.
Gorman PH, Scott W, York H, Theyagaraj M, Price-Miller N, McQuaid J et al. Robotically assisted treadmill exercise training for improving peak fitness in chronic motor incomplete spinal cord injury: a randomized controlled trial. J Spinal Cord Med 2016; 39: 32–44.
Alcobendas-Maestro M, Esclarin-Ruz A, Casado-Lopez RM, Munoz-Gonzalez A, Perez-Mateos G, Gonzalez-Valdizan E et al. Lokomat robotic-assisted versus overground training within 3 to 6 months of incomplete spinal cord lesion: randomized controlled trial. Neurorehabil Neural Repair 2012; 26: 1058–1063.
Esclarin-Ruz A, Alcobendas-Maestro M, Casado-Lopez R, Perez-Mateos G, Florido-Sanchez MA, Gonzalez-Valdizan E et al. A comparison of robotic walking therapy and conventional walking therapy in individuals with upper versus lower motor neuron lesions: a randomized controlled trial. Arch Phys Med Rehabil 2014; 95: 1023–1031.
Alexeeva N, Sames C, Jacobs PL, Hobday L, Distasio MM, Mitchell SA et al. Comparison of training methods to improve walking in persons with chronic spinal cord injury: a randomized clinical trial. J Spinal Cord Med 2011; 34: 362–379.
Dobkin B, Apple D, Barbeau H, Basso M, Behrman A, Deforge D et al. Weight-supported treadmill vs over-ground training for walking after acute incomplete SCI. Neurology 2006; 66: 484–493.
Field-Fote EC, Roach KE . Influence of a locomotor training approach on walking speed and distance in people with chronic spinal cord injury: a randomized clinical trial. Phys Ther 2011; 91: 48–60.
Kapadia N, Masani K, Craven BC, Giangregorio LM, Hitzig SL, Richards K et al. A randomized trial of functional electrical stimulation for walking in incomplete spinal cord injury: effects on walking competency. J Spinal Cord Med 2014; 37: 511–524.
Hornby TG, Campbell DD, Zemon DH, Kahn JH, Moore J, Roth H. Assessment of robotic-assisted locomotor training in individuals with subacute, motor incomplete SCI: a randomized, controlled pilot study. 2007.
Labruyère R, van Hedel HJ . Strength training versus robot-assisted gait training after incomplete spinal cord injury: a randomized pilot study in patients depending on walking assistance. J Neuroeng Rehabil 2014; 11: 4.
Lucareli PR, Lima MO, Lima FPS, De Almeida JG, Brech GC, D'Andréa Greve JM . Gait analysis following treadmill training with body weight support versus conventional physical therapy: a prospective randomized controlled single blind study. Spinal Cord 2011; 49: 1001–1007.
Postans NJ, Hasler JP, Granat MH, Maxwell DJ . Functional electrical stimulation to augment partial weight-bearing supported treadmill training for patients with acute incomplete spinal cord injury: a pilot study. Arch Phys Med Rehabil 2004; 85: 604–610.
Sadhegi H, Banitalebi E, Dehkordi M . The effect of body-weight-supported training exercises on functional ambulation profile in patients with paraplegic spinal cord injury. Phys Treat 2015; 4: 205–212.
Senthilvelkumar T, Magimairaj H, Fletcher J, Tharion G, George J . Comparison of body weight-supported treadmill training versus body weight-supported overground training in people with incomplete tetraplegia: a pilot randomized trial. Clin Rehabil 2015; 29: 42–49.
Shin JC, Kim JY, Park HK, Kim NY . Effect of robotic-assisted gait training in patients with incomplete spinal cord injury. Ann Rehabil Med 2014; 38: 719–725.
Yang JF, Musselman KE, Livingstone D, Brunton K, Hendricks G, Hill D et al. Repetitive mass practice or focused precise practice for retraining walking after incomplete spinal cord injury? A pilot randomized clinical trial. Neurorehabil Neural Repair 2014; 28: 314–324.
Barrett B, Brown D, Mundt M, Brown R . Sufficiently important difference: expanding the framework of clinical significance. Med Decis Making 2005; 25: 250–261.
Wood L, Egger M, Lotte Gluud L, Schulz KF, Jüni P, Altman DG et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta-epidemiological study. BMJ 2008; 336: 601–605.
Sun X, Briel M, Busse JW, You JJ, Akl EA, Mejza F et al. Credibility of claims of subgroup effects in randomised controlled trials: systematic review. BMJ 2012; 344: e1553.
Sterne JAC, White IR, Carlin JB, Spratt M, Royston P, Kenward MG et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 2009; 339: 157–160.
Higgins J, Green S (eds) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available at: www.cochrane-handbook.org..
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Mehrholz, J., Harvey, L., Thomas, S. et al. Is body-weight-supported treadmill training or robotic-assisted gait training superior to overground gait training and other forms of physiotherapy in people with spinal cord injury? A systematic review. Spinal Cord 55, 722–729 (2017). https://doi.org/10.1038/sc.2017.31
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2017.31
This article is cited by
-
Effects of dynamic body weight support on functional independence measures in acute ischemic stroke: a retrospective cohort study
Journal of NeuroEngineering and Rehabilitation (2023)
-
Exoskeleton-based training improves walking independence in incomplete spinal cord injury patients: results from a randomized controlled trial
Journal of NeuroEngineering and Rehabilitation (2023)
-
Transcutaneous spinal cord stimulation combined with locomotor training to improve walking ability in people with chronic spinal cord injury: study protocol for an international multi-centred double-blinded randomised sham-controlled trial (eWALK)
Spinal Cord (2022)
-
Body weight-supported gait training for patients with spinal cord injury: a network meta-analysis of randomised controlled trials
Scientific Reports (2022)
-
Systematic review on wearable lower-limb exoskeletons for gait training in neuromuscular impairments
Journal of NeuroEngineering and Rehabilitation (2021)
