
Key Points
-
This study examines parents' preferences for the dental care of their children and the influences on these choices.
-
Approximately two thirds of parents preferred the dentist to decide on the treatment.
-
If their child had a carious but symptomless primary tooth 33% of parents wanted the dentist to monitor the tooth but provide no treatment and only 6% would want the tooth restored.
-
Parents whose children had experienced fillings or extractions in the past were more likely to show a preference for these treatments if their child had toothache.
-
Parents living in deprived areas were more likely to choose extraction as a treatment option than parents living in more affluent areas.
Abstract
Objectives To examine parents' attitudes to the dental care of their children, taking into account the family's socio-economic background, dentally-related behaviour including the child's level of dental anxiety and dental treatment history.
Methods A cross sectional study of all 5-year-old children living in Ellesmere Port and Chester. All children were clinically examined; dmft and its components were recorded. A postal questionnaire was sent to the children's parents to measure their preferences for dental care with reference to two scenarios, (1) if their child had a carious but asymptomatic primary tooth, or (2) if their child had a carious primary tooth which was causing toothache. Parents were also asked to provide information on the dental attendance pattern of their child and an assessment of their child's dental anxiety. Family socio-economic status was recorded using the Townsend material deprivation index of the electoral ward in which they resided.
Results Questionnaires were distributed to the home addresses of the 1,745 children who were clinically examined, and 1,437 were returned, giving a response rate of 82%. In both scenarios the majority of parents were happy to leave the decision on treatment to the dentist. In the asymptomatic tooth scenario, approximately one third of parents wanted the tooth to remain untreated but periodically monitored, only 6% expressed a desire to have their child's tooth restored. Multivariate analysis showed that parents of children who had a filling (OR 4.32 95%CI 2.21–8.43) or extraction (OR 2.24 95%CI 1.11–4.53) in the past were significantly more likely to want restorative care for their children. In the scenario where the child had toothache, multivariate analysis confirmed that parents had a preference for an intervention (extraction or filling) if they lived in a deprived area (Townsend score OR 1.10, 95% CI 1.04, 1.16) or if their child had had an extraction (OR 4.35, 95% CI 1.59, 11.88) or filling (OR 2.39, 95% CI 1.05, 5.45) in the past, after controlling for gender, attendance and parentally reported anxiety. When preference for an extraction was considered as the dependent variable, there was no significant relationship with past restorative treatment. In both scenarios there was no association between parentally reported anxiety of the child and parental preferences for treatment.
Conclusions In this part of the UK, there was little explicit support amongst parents for the restoration of asymptomatic carious primary teeth. Parental expectations for the dental care of young children with caries in their primary teeth, were closely related to the treatment experiences of the child. Families living in deprived areas expressed a preference for more interventionist care than their more affluent counterparts. Parentally judged anxiety of the child or their past dental attendance behaviour had no association with parents' preferences for the care of their children.
Similar content being viewed by others


Introduction
Recent studies1,2,3,4 have indicated that the care of children with carious primary teeth provided by many UK general dental practitioners (GDPs) is at variance to the guidance issued by specialist paediatric dentists.5 Many paediatric dentists advocate that a carious lesion, which has breached the marginal ridge of a primary molar tooth, should be treated using pulp therapy followed by restoration with a preformed crown.6 However, primary care-based studies have demonstrated that GDPs in the UK preferentially use glass ionomer as a restorative material,7 very rarely prescribe pulp therapy and preformed stainless steel crowns and leave some carious primary teeth unrestored.2 These findings are supported by statistics produced by the Dental Practice Board. For example, in 2001/2 only 4,255 stainless steel crown restorations were claimed for by GDPs in England and Wales; a minuscule number given that 5.07 million children under the age of 12 were registered with a GDP in the period October to December 20018 and that the prevalence of disease in UK five-year-olds in 1999/2000 was 39%.9
Dental treatment of young children is usually provided only after close consultation with parents. Given the disparity between the approach to care advocated by specialists and the care provided by GDPs several questions arise. How much influence do parents' wishes have on the treatment of young children? Do they have strong preferences for the type of care provided or are they content to leave the treatment decisions solely to the dentist? The existing dental literature is not very helpful in answering these questions. Studies in the medical field may be of assistance; some have advocated detailed assessment of parental opinion associated with completing treatment procedures.10,11 Parents are encouraged to enter into the decision processes involved in managing ill children.12 However, investigators less frequently assess parental preferences and do not extend this to understanding if parents desire to be offered such choices. A notable exception is Yamomoto and colleagues13 who found that 98% of parents preferred to be included in medical decision-making for their children in the choice of anaesthesia or sedation for repair of lacerations.
Another aspect of this issue is to consider how closely attuned the dental profession is to the wishes of parents. For example, a recent study14 showed that 53% of parents assessed their children as having a tendency to cry when receiving dental care, while only 25% of children were assessed as such by their dentist. Professional guidance, based on expert advice or even randomised controlled trials, cannot be adopted by dentists if that guidance is unacceptable to parents and children. For instance, the 'papoose board' described in American studies15,16 may be an effective, short-term means of ensuring that uncooperative, distressed children can be operated upon, but it is unlikely that this model of care would be acceptable to UK parents.
Social norms should also be noted when considering parental preferences for care. For example UK parents have commonly accepted the widespread use of general anaesthetic to manage the dental care of young children. One reason for this could be that many parents were treated using this method when they were young and have little experience of other methods of patient management, therefore they may expect the same type of care for their children. However, recent high profile cases involving deaths during a dental anaesthetic may have changed parents' views. Advice given during dental consultations may have also altered parental views; GDPs tend to treat caries conservatively and this approach may be more acceptable to parents after their dentist has explained this philosophy.
Behavioural and social factors, such as attendance patterns, parents' perceptions of their children's level of dental anxiety and the socio-economic status of the family may also influence parental attitudes to dental care. For example, five-year-old children in the north west of England who were irregular asymptomatic dental attenders had significantly more untreated decayed teeth and extractions, but less filled teeth than regular asymptomatic attenders.17 Another recent paper from a study undertaken in the north west of England has also reported that young children from disadvantaged backgrounds are more likely to receive extractions than their more affluent peers with similar caries experience and restorative history.18 Unfortunately there is little information in the literature to show if parents' assessments of their children's anxiety influences their preferences for the dental care of their children. The relationship between parental preferences and these factors requires further examination.
The purpose of this study was to examine parental attitudes to dental care taking into account the family's socio-economic background, dentally-related behaviour including the reported levels of dental anxiety of the child's dental treatment history.
Methods
A whole population survey of 5-year-old children attending state registered schools in Chester and Ellesmere Port was undertaken. Three examiners collected data on caries prevalence and caries experience according to the national protocol for NHS surveys. All examiners were trained and calibrated according to British Association for the Study of Community Dentistry (BASCD) guidelines.19 The parents of all of the children examined were sent a questionnaire at the same time as the clinical survey. The questionnaire asked parents to report:
-
if their child attended the dentist on a regular asymptomatic basis or if they attended only when in pain,
-
whether or not their child was frightened or anxious about dental treatment. This variable was collected as a five point scale ranging from very relaxed to very frightened about dental treatment. This was subsequently dichotomised for the analyses by categorising children as frightened\anxious if their parents indicated that they were either fairly or very frightened about dental treatment,
-
their preferences for care if their child had a:
Scenario 1) carious but asymptomatic primary tooth;
Scenario 2) carious primary tooth which was causing toothache.
Parents were given the response choices of:
-
restore the tooth,
-
extract the tooth under general anaesthetic,
-
extract the tooth under local anaesthetic,
-
relieve the symptoms and monitor the tooth,
-
to leave the treatment decision to the dentist.
The extraction options were not provided for the asymptomatic carious tooth scenario.
Two reminders, at one and two months following the initial administration of the questionnaire, were sent out to improve response rate. Questionnaire data were merged with the clinical survey data file. Each subject's home postcode was recorded, added to the data file and used to attach the Townsend material deprivation score20 of the electoral ward of residence of each child. This area based index has been very commonly used in the UK as a proxy measure of socio-economic status of individuals.
Cross tabulations and Pearson chi-square tests were performed to test for associations between the parental preferences identified for each clinical scenario and:
-
reported attendance patterns,
-
parentally judged dental anxiety status of the child,
-
dental treatment (extraction or filling) history derived from the findings of the clinical survey.
Mean Townsend scores were calculated for each response category for each scenario and one way analysis of variance with the Bonferroni pairwise modification to the P value was used to test which of the mean values were significantly different from one another. Finally, a series of logistic regression analyses were performed. Each scenario was dichotomised. For the scenario in which the carious primary tooth was symptomless parents were categorised into wanting the tooth restored/not wanting the tooth restored. For the second scenario, in which the carious primary tooth was responsible for toothache, parents were categorised as expressing a choice for an intervention (filling or extraction) or preferring minimal intervention (relieve the symptoms and monitor the tooth) and leaving the treatment decision to the dentist. A second categorisation of this variable was also performed; parents were categorised as expressing a choice for an extraction (either using general or local anaesthetic) or all other choices. These three dichotomised variables were used as dependent variables to construct multiple logistic regression models with the independent variables:
-
gender
-
child dental fear\anxiety (parentally judged)
-
past attendance pattern
-
Townsend score
-
never had\had an extraction
-
never had\had a filling (children who had extractions were excluded)
Results
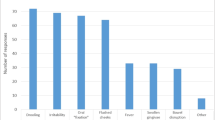
In all, 1,745 children received both clinical examinations and a questionnaire sent to their home address. Questionnaires were returned by 1,437 parents, an 82% response rate. The population had a dmft of 1.27 (SD 2.54) and dmft>0 33.8%. Item non-response varied slightly for the variables under consideration. Table 1 summarises the parental preferences for the scenario of their child having a carious but symptom-free primary tooth. The majority of parents would elect to leave any care decision in the hands of the dentist. About one third of parents did not want any treatment provided, but wanted the situation monitored. Only 6% expressed a desire to have their child's carious tooth restored. Table 2 presented the frequency distribution for the second scenario, a carious primary tooth causing toothache. The percentages in each category showed that slightly more parents would leave the decision up to the dentist (65.9%), approximately 12% would want the dentist to relieve the symptoms and monitor the tooth, the same percentage of parents wanted the tooth filled and around 9% of parents wanted the tooth to be extracted, either by general or local anaesthetic.
The bivariate relationships between parental choices and dental treatment history, socio-economic status, reported dental attendance and the anxiety of the child were considered prior to performing the logistic regression analyses. In the first scenario, for the asymptomatic tooth, none of the relationships between parental preferences and attendance, socio-economic status, and child anxiety were statistically significant. However, parents whose children had a filling in the past, were significantly (χ2 21.66, dof 2, P<0.001) more likely to express a preference for restorative treatment in this scenario than those children who had no previous history of restorative care. There was no significant relationship between preferences in this scenario and a history of extraction or for children with untreated caries.
A different set of bivariate relationships was found for the scenario of the child with a painful decayed tooth. A significant (χ2 18.75, dof 4, P<0.001) relationship was found between dental attendance and parental preferences, 37.3% of parents whose child was an irregular symptomatic attender wanted the tooth extracted under general anaesthesia, compared with values of between 15%–20% for asymptomatic regular attenders in the other categories. No association could be found between parentally reported anxiety of the child and parental preferences for treatment. Using the post hoc Bonferroni correction, significant differences were found between socio-economic status and the preferences in the painful carious tooth scenario. Parents who said they would want the tooth filled under these circumstances were significantly (P<0.05) more likely to live in a deprived area than those who wanted to leave the decision to the dentist. Whereas those parents who had a preference for an extraction under general anaesthesia were significantly more likely to live in a deprived area than those who would leave the decision to the dentist or would want the symptoms relieved and the tooth monitored. Therefore parents from more deprived backgrounds were more likely to want an intervention of some kind.
Parents whose children had had an extraction in the past and had a symptomatic tooth were significantly (χ2 66.17, dof 4, P<0.001) more likely to favour extraction under general anaesthesia. There was no statistically significant association for the choices for this scenario if the child had a history of previously having a filling.
Table 3 summarises the results of two logistic regression analysis for the dependent variable whether or not the parents preferred a filling for the asymptomatic carious tooth scenario. The independent variables Townsend score, gender, parentally judged dental anxiety of the child and reported attendance pattern did not have a significant effect on parental choices in each of the models. However the past dental treatment of the child had a significant effect on preferences after controlling for socio-economic status, gender, dental anxiety and attendance patterns. Parents of children who had previously had an extraction were over twice as likely (OR=2.24, 95% CI of OR 1.11, 4.53) to express a preference for a filling than parents of children who had never experienced an extraction. Parents whose children had a filling in the past were over four times more likely (OR=4.32, 95% CI of OR 2.21, 8.43) to want their child to have a filling in this scenario than parents whose children had never had a filling.
Table 4 summarises the results of two more logistic regression analyses for the responses to the painful carious primary tooth scenario. The answers were dichotomised according to whether or not the parents preferred an intervention of some sort (filling or extraction). In both analyses socio-economic status was a significant predictor, parents from more deprived backgrounds preferred to have some sort of intervention after controlling for other factors. Other independent variables were non-significant; these included gender, child dental anxiety (parentally judged) and past attendance pattern. Dental treatment history was a significant predictor of parental preferences. Parents whose children had an extraction in the past were over four times more likely (OR=4.35, 95% CI of OR 1.59, 11.88) to favour an intervention than those whose children had no history of extraction after controlling for socio-economic status, gender, anxiety and attendance. Parents of children who had a filling in the past were more than twice as likely to express a preference for some kind of treatment intervention (OR=2.39, 95% CI of OR 1.05, 5.45) than parents whose children had never had a filling. The final set of logistic regression analyses dichotomised parental responses to scenario two (carious and painful tooth) into wanting an extraction or one of the other categories and the results are presented in Table 5 Parents whose children had experienced an extraction were over three times more likely (OR=3.39, 95% CI of OR 1.97, 5.84) to express a choice for extraction than parents whose children had not experienced an extraction. Restorative treatment received in the past had no significant influence on parental preference for an extraction (OR=1.08, 95% CI of OR 0.51, 2.27).
Discussion
This study examines the preferences of parents regarding the dental care of their children. It provides some new information to add to the current debate in the UK concerning how best to manage the dental care of children with carious primary teeth. Although the questionnaire response rate of 82% was acceptable, there was a degree of non-response bias present in this study as non-responders to the survey were significantly more likely to live in deprived areas than responders. However, a methodological paper based on the data from this study21 describing aspects of measuring and correcting for non-response bias in this study demonstrated that it had a small effect on the key outcome measures and the magnitude of the differences between deprived and affluent groups. This methodological paper and a sister paper looking at predictors of dental fear and anxiety22 also demonstrated a very close positive association between the Townsend index and the dmft and a negative association between the index and dental attendance patterns of this population, demonstrating that the Townsend index is a robust proxy for the socio-economic status of individuals in this population.
One of the reassuring findings of the study is that in both scenarios, the majority (two-thirds) of parents had confidence in their dentist to make clinical treatment decisions in the best interests of their children. This reflects the imbalance in knowledge that always exists between patients (in this case parents) and healthcare professionals. So, although parents are guardians of their child's wellbeing they may not have a clear understanding of specific health problems, and the range of available treatments including their effectiveness. Given these circumstances the parent as a consumer of healthcare is not in a position to make informed decisions when selecting healthcare services. This places the responsibility on the dentist to provide adequate information (based on the best available evidence) to enable parents to provide truly informed consent for the dental care of their child.
It is of great interest that only 6% of parents would want the dentist to fill a carious, asymptomatic tooth, and nearly one third of parents would want no treatment, preferring the dentist to monitor the situation, rather than providing some form of restorative treatment. From the results it would seem that many parents accepted a non-interventionist approach to providing care for children with caries in the primary dentition, an approach to care which seems to have been adopted by some UK GDPs. The reasons for this finding are open to speculation. It may reflect a general reluctance of parents to have any dental or medical intervention performed on their children for minor symptomless ailments. Alternatively dentists may be explaining their conservative approach to care at the chairside and parents have accepted this philosophy. What is clear is that neither socio-economic status, reported attendance patterns nor the children's anxiety levels significantly affected parental preferences in scenario one. However, the logistic regression analyses showed that past treatment experience was the most important factor in predicting parental preferences. Parents of children who had had a filling in the past (and to a lesser extent an extraction) were more likely to express a preference for restorative care. This finding suggests that parents who have experience of their child receiving specific types of dental care are happy with the care provided and are more likely to prefer this type of treatment in the future.
When parents were asked to consider children who had a decayed tooth, which was causing toothache, a similar proportion of parents would leave the decision to the dentist. However, a greater proportion of parents (21.6%) would expect some kind of defined intervention to be provided, either a filling (12.5%) or an extraction (9.1%). The regression analyses demonstrated that there was a constant socio-economic influence associated with expectations generated by this scenario, which was missing in the first scenario. Parents from more deprived backgrounds were more likely to have a preference for a treatment intervention, either an extraction or filling, whereas parents from more affluent backgrounds had a greater preference for the professionals to make a decision on their behalf and were less keen on operative interventions. Bivariate analysis showed that parents who wanted an extraction under general anaesthesia were more likely to identify that their children were irregular, symptomatic attenders than parents who opted for a less traumatic approach to care. However, this type of attendance pattern is closely associated with deprivation17 and the multivariate analyses suggest that the significant association found between attendance patterns and parental preferences was confounded by this relationship, as attendance was not a significant factor in any of the logistic regression models.
Interestingly, the results demonstrate that parental assessment of their children's dental anxiety status had no significant influences on their preferences for care. This is puzzling, as one would expect parents of children, who they classify as being dentally anxious, to be less keen on intervention. One would therefore expect that this factor would have an independent effect on preferences. Several possible explanations may account for the limited effect of anxiety on parental preferences. First, there is some evidence that less than 40% of parents believe invasive dental experiences raise dental anxiety.23 Other factors reported by parents as possible causative triggers included medical problems, the child's temperament and the dentist's behaviour. Second, parents have been shown to perform flexibly in their decision-making according to their opinions about the treatment on offer and the likely outcome.24 Unfortunately, our knowledge-base is weak on parental beliefs about various dental interventions and the consequences for their child. Finally the dichotomous parental assessment of the child's dental anxiety used here may not be a sensitive enough measure to establish the full nature of the relationship. It is interesting that 15% of parents who preferred their child to receive an extraction under general anaesthesia for a painful and carious tooth rated their child as anxious. Parents making other treatment decisions which did not involve loss of consciousness rated their children less frequently as anxious. A more extensive measure of child dental anxiety25 from the parents' perspective may have confirmed this effect.
The factor which seems to have most influence on care preferences of parents is the past treatment that their child has received. The results of the logistic regression analyses suggest that parents were more likely to express an option for treatment that their child has received in the past. For example, in Table 3, the odds ratio was greater for children in receipt of a filling compared with an extraction. Likewise, in Table 5, looking at predictors for extraction as a treatment choice, an extraction history was a significant predictor but history of restoration alone was not. This indicates that when parents acquire experiential knowledge of a specific treatment option they gain a degree of confidence in that procedure. The results concerning preferences for extraction are particularly interesting, given that this study took place during a period of considerable public interest and concern over dental general anaesthetics in the UK. It perhaps again confirms parents' trust in the profession, but may also be due to the dramatic and traumatic nature of this type of treatment. A dental extraction is a notable life event for young children and their families and its successful completion may dispel any feeling of anxiety in parents about the procedure. Perhaps a satisfactory outcome prompts a feeling of trust in this form of treatment, even though morbidity following extractions under general anaesthesia is common and has distressing consequences for the young patients and their carers in the short term.26
This study encourages debate about how best to care for young children with carious primary teeth. It is important that both clinicians and healthcare managers are in tune with the wishes of patients. The results presented demonstrate the reliance of parents on the knowledge and skills of dentists. In addition, other questions are raised about the role of parents in the decisions about the dental care of their children, which requires a more complex study. However this study demonstrates that many parents do not see that restoration of asymptomatic carious primary teeth is imperative. Furthermore, parental expectations for the care of young children are closely associated with dental treatment experiences, and that there is a preference amongst parents living in deprived areas for extractions when their child has toothache. Child dental anxiety and attendance patterns had little effect on treatment preferences. To provide a more complete understanding of parental attitudes to the dental care of their children and determine some of the underlying reasons for the findings of this study a more in-depth qualitative investigation is required. Information from this type of research is needed to contribute to building an appropriate model of dental care for young children in the UK that is acceptable to both parents and dentists.
References
Tickle M, Milsom KM, Kennedy A . Is it better to leave or restore carious deciduous molar teeth? A preliminary study. Prim Dent Care 1999; 6: 127– 131.
Tickle M, Milsom KM, King D, Kearney-Mitchell P, Blinkhorn AS . The fate of the carious primary teeth of children who regularly attend the general dental service. Br Dent J 2002; 192: 219– 223.
Milsom KM, Tickle M, Blinkhorn AS . Dental pain and dental treatment of young children attending the general dental service. Br Dent J 2002; 192: 280– 284.
Levine RS, Pitts NB, Nugent ZJ . The fate of 1,587 unrestored carious deciduous teeth: a retrospective general practice based study from northern England Br Dent J 2002; 193: 94– 98.
Fayle SA, Welbury RR, Roberts JF . British Society of Paediatric Dentistry. A policy document on management of caries in the primary dentition. Int J Paed Dent 2001; 11: 153– 157.
Duggal MS, Nooh A . The relationship between extent of carious involvement of the marginal ridge and pulp inflammation of primary teeth. J Dent Res 1999; 78: 298.
Milsom KM, Tickle M, Blinkhorn AS . The prescription and relative outcomes of different materials used in general dental practice in the north west region of England to restore the primary dentition. J Dent 2002; 30: 77– 82.
Dental Practice Board electronic database of statistics http://www.dentanet.org.uk/dentanet/prof/dpb/index.html
Pitts NB, Evans DJ, Nugent ZJ . The dental caries experience of 5-year-old children in Great Britain. Surveys coordinated by the British Association for the Study of Community Dentistry in 1999/2000. Community Dent Health 2001; 18: 49– 55.
McCarty EC, Mencio GA, Green NE . Anesthesia and analgesia for the ambulatory management of fractures in children. J Am Acad Orthop Surg 1999; 7: 81– 91.
Levi RB, Marsick R, Drotar D, Kodish ED . Diagnosis, disclosure and informed consent: learning from parents of children with cancer. J Pediatr Hematol Oncol 2000; 22: 3– 12.
Oppenheim PI, Sotiropoulos G, Baraff LJ . Incorporating patient preferences into practice guidelines: management of children with fever without source. Am J Emerg Med 1995; 26: 240– 241.
Yamamoto LG, Young LL, Roberts JL . Informed consent and parental choice of anesthesia and sedation for the repair of small lacerations in children. Am J Emerg Med 1997; 15: 285– 289.
Zadik D, Pertez B . Management of the crying child during dental treatment. ASDC J Dent Child 2000; 67: 55– 58.
Sheller B, Williams BJ, Lombardi SM . Diagnosis and treatment of dental caries-related emergencies in a children's hospital. Pediatr Dent 1997;19: 470– 475.
Fuks AB, Kaufman E, Ram D, Hovav S, Shapira J . Assessment of two doses of intranasal midazolam for sedation of young pediatric dental patients. Pediatr Dent 1994; 16: 301– 305.
Tickle M, Williams MJ, Jenner AM, Blinkhorn A . The effects of dental attendance and socio-economic status on dental caries experience and treatment patterns in 5-year-old children. Br Dent J 1999; 186: 135– 137.
Tickle M, Milsom KM, Blinkhorn AS . Inequalities in the dental treatment provided to children: an example from the United Kingdom. Community Dent Oral Epidemiol 2002; 30: 335– 341.
Mitropoulos CM, Pitts NB, Deery C . British Association for the Study of Community Dentistry criteria for the standardised clinical assessment of dental health (1992/3) In: BASCD trainer's pack for caries prevalence studies 1992/3 Dundee, University of Dundee 1992.
Townsend P, Philimore P, Beattie A . Health and Deprivation: inequalities and the North. 1988: London, Croom Helm.
Tickle M, Milsom KM, Blinkhorn AS, Worthington HV . Comparing methods to detect and correct non-response bias in postal questionnaire studies. J Pub Health Dent 2003; 63: 112– 118.
Milsom KM, Tickle M, Humphris GM, Blinkhorn AS . The relationship between socio-economic status, caries and treatment status and reported anxiety in a population of 5-year-old children Br Dent J 2003; 195: 301– 303.
ten Berg M, Veerkamp JS, Hoogstraten J, Prins PJ . Parental beliefs on the origins of child dental fear in The Netherlands. ASDC J Dent Child 2001; 68: 51– 54.
Ogan K, Pohl HG, Carlson D, Belman AB, Rushton HG . Parental preferences in the management of vesicoureteral reflux. J Urol 2001; 166: 240– 243.
Aartman IH, van Everdingen T, Hoogstraten J, Shuurs AH . Self-report measurements of dental anxiety and fear in children: a critical assessment. ASDC J Dent Child 1998; 65: 252– 258.
Bridgman CM, Ashby D, Holloway PJ . An investigation of the effects on children of tooth extraction under general anaesthesia in general dental practice. Br Dent J 1999; 186: 245– 247.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Tickle, M., Milsom, K., Humphris, G. et al. Parental attitudes to the care of the carious primary dentition. Br Dent J 195, 451–455 (2003). https://doi.org/10.1038/sj.bdj.4810600
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4810600
This article is cited by
-
Improvement of parents’ oral health knowledge by a school-based oral health promotion for parents of preschool children: a prospective observational study
BMC Oral Health (2023)
-
Guidelines relevant to paediatric dentistry – do foundation dentists and general dental practitioners follow them? Part 2: Treatment and recall
British Dental Journal (2018)
-
Head Start Oral Health Assessment
Maternal and Child Health Journal (2016)
-
An assessment of dental caries among young Aboriginal children in New South Wales, Australia: a cross-sectional study
BMC Public Health (2015)
-
A pilot of a school-based dental treatment programme for vulnerable children with possible dental neglect: the Back2School programme
British Dental Journal (2013)
