
Abstract
Epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKI) as gefitinib emerged as an accepted treatment in second- or third-line setting in NSCLC. However, clinical surrogate markers of EGFR-TKI activity in NSCLC patients remain to be identified and we studied the prognostic value of CYFRA 21-1 in this setting. Serum samples from 53 patients with NSCLC receiving gefitinib after failure of at least a platinum-containing regimen were prospectively collected from January 2002 to December 2003. Multivariate analysis demonstrated an independent negative impact on survival for a level of CYFRA 21-1 higher than 3.5 ng ml−1 (HR=2.45, 95% CI 1.13–5.29; P=0.02). In conclusion, CYFRA 21-1 is a tool available to predict the survival of NSCLC patients receiving gefitinib as third-line therapy in an independent manner. In case of a CYFRA 21-1 level higher than 3.5 ng ml−1, treatment with gefitinib needs further evaluation giving its relative poor effect on survival.
Similar content being viewed by others

Main
The prognostic value of CYFRA 21-1 for non-small-cell lung cancer (NSCLC) patients was recently definitively demonstrated in a meta-analysis in 2063 patients (Pujol et al, 2004). In the same time, epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKI) as gefitinib emerged as an accepted treatment in second- or third-line setting in NSCLC (Pfister et al, 2004). However, clinical surrogate markers of EGFR-TKI activity in NSCLC patients after failure of platinum-containing regimen remain to be identified. So, we conducted a study of the prognostic value of CYFRA 21-1 in NSCLC patients receiving gefitinib after failure of platinum-containing regimen in an expanded access program.
Patients and methods
Serum samples from patients with NSCLC receiving gefitinib after failure of at least a platinum-containing regimen were prospectively collected from January 2002 to December 2003. Histological subclassification was carried out according to the World Health Organization classification. Performance Status was estimated using the Eastern Cooperative Oncology Group (ECOG) scale. Clinical examination, chest, abdomen and brain-computed tomographic scan were carried out systematically.
Serum samples were obtained from each patient before gefitinib therapy. Fresh serum was collected and cooled after sampling, and then stored at −20°C until analysis. All assays were performed using commercial kit (ELSA CYFRA 21-1 CisBiointernational™) blind to clinical information. Serum level of CYFRA 21-1 was considered as elevated when it was superior or equal to 3.5 ng ml−1. Cutoff value of 3.5 ng ml−1 for CYFRA 21-1 was based on previously published results (Reinmuth et al, 2002). All patients consented to treatment with gefitinib.
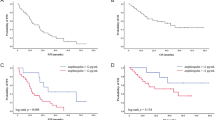
Survival data were updated in June 2004. One patient was lost. Probability of survival was estimated using the Kaplan–Meier method. Differences between survival were tested by means of log-rank test. A multivariate regression analysis was carried out with Cox's regression using the forward maximum-likelihood method. All variables with a P-value less than 0.20 at the time of univariate analysis were entered into the model. A P-value less than 0.05 was considered as significant.
Results
In all, 53 patients were included in the study (Table 1). Two patients did not received gefitinib due to disease progression and were excluded from analysis. The median age of the 51 patients was 60 years (38–78 years). All the patients were current or former smokers. All the patients received a two-drugs platinum-containing regimen as first line of treatment. A total of 47 (92.1%) received a third-generation drug regimen (gemcitabine, docetaxel or paclitaxel) in both first- and second-line therapy. A skin toxicity of grade 1 and 2 occurred for 11 (21.6%) and two (3.9%) patients, respectively. Diarrhoea occurred for eight patients (15.7%). The median duration of treatment was 3.3 months. The disease control rate was 70.6%, with 11.7% of partial response and 58.9% of stable disease. At the time of analysis, 33 patients were deceased. The median survival time was 4 months (1 to 20+ months).
The principal results of univariate analysis are shown in Table 2. Multivariate analysis demonstrated an independent favourable impact on survival for occurrence of a skin reaction (HR=0.28, 95% CI 0.12–0.66; P=0.004) and an independent negative impact on survival for a level of CYFRA 21-1 higher than 3.5 ng ml−1 (HR=2.45, 95% CI 1.13–5.29; P=0.02).
Discussion
This study highlights the role of CYFRA 21-1 level in assessing prognosis of NSCLC patients receiving gefitinib as third-line therapy (HR for death is 2.45 for patients with CYFRA 21-1 level higher than 3.5 ng ml−1, P=0.02). Giving this result, CYFRA 21-1 could be used as a help in determining patients who beneficiate from treatment with gefitinib. This could be of a paramount importance giving the lack of clinical factors in this setting.
Whereas genetic mutations on EGFR gene receptor were identified in tumours of patients responding to gefitinib (Lynch et al, 2004; Paez et al, 2004), we also need more easily assessable and clinically available predictive factors for response to gefitinib for daily practice. Using commercial kit, CYFRA 21-1 is easily assessable and its role as prognostic marker alone (Pujol et al, 2004) or in combination (Barlési et al, 2004) has been demonstrated. Furthermore, the prognostic value of CYFRA 21-1 in the present study was higher than that of clinical (performance status, weight loss) or biological (leucocytes, liver enzymes) traditional prognostic markers. In addition, previous studies interested in clinical (gender, Karnofsky index) or biological (EGFR expression, HER2 expression) factors predictive for response or survival for patients treated with gefitinib reported contradictive or negative results, except for those with adenocarcinoma histological subtype and nonsmoking history, which predict a better survival (Miller et al, 2004). Likewise, skin rash has been suggested to predict response to gefitinib as we have shown in our multivariate analysis; however, available data do not definitively support this hypothesis (van Zandwijk, 2003).
In conclusion, CYFRA 21-1 is a tool available to predict survival of NSCLC patients receiving gefitinib as third-line therapy in an independent manner. So, CYFRA 21-1 should be integrated in the biological assessment of NSCLC patients prior to receiving gefitinib. In case of a CYFRA 21-1 level higher than 3.5 ng ml−1, treatment with gefitinib needs further evaluation giving its relative poor effect on survival.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Barlési F, Gimenez C, Torre JP, Doddoli C, Mancini J, Greillier L, Roux F, Kleisbauer JP (2004) Prognostic value of combination of CYFRA 21-1, CEA and NSE in patients with advanced non-small cell lung cancer. Respir Med 98: 357–362
Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, Louis DN, Christiani DC, Settleman J, Haber DA (2004) Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med 350: 2129–2139
Miller VA, Kris MG, Shah N, Patel J, Azzoli C, Gomez J, Krug LM, Pao W, Rizvi N, Pizzo B, Tyson L, Venkatraman E, Ben-Porat L, Memoli N, Zakowski M, Rusch V, Heelan RT (2004) Bronchioloalveolar pathologic subtype and smoking history predict sensitivity to gefitinib in advanced non-small-cell lung cancer. J Clin Oncol 22: 1103–1109
Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, Naoki K, Sasaki H, Fujii Y, Eck MJ, Sellers WR, Johnson BE, Meyerson M (2004) EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science 304: 1497–1500
Pfister DG, Johnson DH, Azzoli CG, Sause W, Smith TJ, Baker Jr S, Olak J, Stover D, Strawn JR, Turrisi AT, Somerfield MR, American Society of Clinical Oncology (2004) American Society of Clinical Oncology treatment of unresectable non-small-cell lung cancer guideline: update 2003. J Clin Oncol 22: 330–353
Pujol JL, Molinier O, Ebert W, Daures JP, Barlesi F, Buccheri G, Paesmans M, Quoix E, Moro-Sibilot D, Szturmowicz M, Brechot JM, Muley T, Grenier J (2004) CYFRA 21-1 is a prognostic determinant in non-small-cell lung cancer: results of a meta-analysis in 2063 patients. Br J Cancer 90: 2097–2105
Reinmuth N, Brandt B, Semik M, Kunze WP, Achatzy R, Scheld HH, Broermann P, Berdel WE, Macha HN, Thomas M (2002) Prognostic impact of CYFRA 21-1 and other serum markers in completely resected non-small cell lung cancer. Lung Cancer 36: 265–270
van Zandwijk N (2003) Tolerability of gefitinib in patients receiving treatment in everyday clinical practice. Br J Cancer 89(Suppl 2): S9–S14
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Barlési, F., Tchouhadjian, C., Doddoli, C. et al. CYFRA 21-1 level predicts survival in non-small-cell lung cancer patients receiving gefitinib as third-line therapy. Br J Cancer 92, 13–14 (2005). https://doi.org/10.1038/sj.bjc.6602296
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6602296
Keywords
This article is cited by
-
The important role of circulating CYFRA21-1 in metastasis diagnosis and prognostic value compared with carcinoembryonic antigen and neuron-specific enolase in lung cancer patients
BMC Cancer (2017)
-
History, molecular features, and clinical importance of conventional serum biomarkers in lung cancer
Surgery Today (2017)
-
Correlation between EGFR gene mutation, cytologic tumor markers, 18F-FDG uptake in non-small cell lung cancer
BMC Cancer (2016)
-
Prognostic value of serum cytokeratin 19 fragments (Cyfra 21-1) in patients with non-small cell lung cancer
Scientific Reports (2015)
-
CEA serum level as early predictive marker of outcome during EGFR-TKI therapy in advanced NSCLC patients
Tumor Biology (2015)
