
Abstract
Background:
Diabetics have been found to have a greater risk of colorectal cancer than non-diabetics.
Methods:
We examined whether this relationship differed by ethnic group, cancer site or tumour stage in a population-based prospective cohort, including 3549 incident colorectal cancer cases identified over a 13-year period (1993–2006) among 199 143 European American, African American, Native Hawaiian, Japanese American and Latino men and women in the Multiethnic Cohort.
Results:
Diabetics overall had a significantly greater risk of colorectal cancer than did non-diabetics (relative risk (RR)=1.19, 95% confidence interval (CI)=1.09–1.29, P-value (P)<0.001). Positive associations were observed for colon cancer, cancers of both the right and left colon, and cancers diagnosed at a localised and regional/distant stage. The association with colorectal cancer risk was significantly modified by smoking status (PInteraction=0.0044), with the RR being higher in never smokers (RR=1.32, 95% CI=1.15–1.53, P<0.001) than past (RR=1.19, 95% CI=1.05–1.34, P=0.007) and current smokers (RR=0.90, 95% CI=0.70–1.15, P=0.40).
Conclusion:
These findings provide strong support for the hypothesis that diabetes is a risk factor for colorectal cancer.
Similar content being viewed by others

Main
Colorectal cancer and type 2 diabetes share several risk factors including western diet, obesity and physical inactivity, and epidemiological studies have provided evidence to support a positive relationship between these two common diseases (Will et al, 1998; Nilsen and Vatten, 2001; Levi et al, 2002; Yang et al, 2005). One hypothesis purported to explain the association is the ‘hyperinsulinemia-hypothesis’ (McKeown-Eyssen, 1994; Giovannucci, 1995), whereby insulin resistance in type 2 diabetics leads to higher insulin levels, as well as an increased level of bioavailable IGF-I. The proliferative effects of insulin and IGF-I on the colon epithelium are believed to increase the potential for spontaneous mutations and have an important function in both the initiation and progression phases of carcinogenesis in colorectal cancer. This hypothesis is further supported by the findings that elevated circulating levels of C-peptide and IGF-I are associated with an increased risk of colorectal cancer (Kaaks et al, 2000; Sandhu et al, 2002; Ma et al, 2004; Renehan et al, 2004; Schoen et al, 2005; Jenab et al, 2007; Otani et al, 2007). Studies of the relationship between type 2 diabetes and colorectal cancer risk in racial/ethnic populations other than Whites have been limited; however, in general, they also support the positive association between these conditions (Jee et al, 2005; Seow et al, 2006; Vinikoor et al, 2009). We conducted a prospective analysis of the relationship between diabetes and colorectal cancer risk in the Multiethnic Cohort. This large prospective cohort includes five racial/ethnic populations (European Americans, African Americans, Native Hawaiians, Japanese Americans and Latinos) that represent a wide variation in the incidence of these diseases, as well as in the prevalence of known risk factors. Here, we report on the association between these end points by race, sex, cancer site (colon vs rectum and left colon vs right colon), stage (localised vs regional/distant) and in strata of established risk factors for colorectal cancer.
Materials and methods
The Multiethnic Cohort includes 215 251 men and women in Hawaii and California (largely from Los Angeles County). The participants are primarily individuals of Native Hawaiian, Japanese, White, African American and Latino race/ethnicity, who entered the cohort between 1993 and 1996 by completing a detailed, self-administered questionnaire that obtained information on basic demographic variables, as well as several lifestyle factors (e.g. diet) and medical conditions (e.g. diabetes). Potential cohort members were identified primarily through the Department of Motor Vehicles drivers’ license files and additionally for African Americans, Health Care Financing Administration (Medicare) data files. Participants were between the ages of 45 and 75 years at the time of recruitment. In the cohort, incident colorectal cancer cases are identified through cohort linkage to population-based cancer Surveillance, Epidemiology and End Results registries, which cover Hawaii and Los Angeles County, as well as the rest of the state of California. For this analysis, linkage with these registries was complete through 31 December 2004, in Hawaii and 31 December 2006 in California. Over this period, 1921 male and 1628 female cases of colorectal cancer were identified. Deaths within the cohort are determined from linkages to the death certificate files in Hawaii and California, supplemented with linkages to the National Death Index. Diabetes status is defined based on self-report to a question on the baseline questionnaire asking whether a doctor had ever told the respondent that he/she had diabetes (high blood sugar). The question did not differentiate between type 1 and type 2 diabetes mellitus and thus we expect a small fraction (<10%) of the self-reported diabetes cases to have type 1 diabetes and be potentially misclassified. Year of diabetes diagnosis (before 1994, 1994, 1995, 1996, 1997 or 1998) was defined using a second questionnaire in 2001, and 90.3% (79 178 men and 100 663 women) of the subjects who returned the first questionnaire also returned the second questionnaire.
In the analysis, we excluded one male subject missing information for diabetes status on the baseline questionnaire. The prospective analysis of the association between diabetes status and colorectal cancer incidence in this study includes 89 478 men and 109 664 women in the Multiethnic Cohort from the five main ethnic groups.
The study protocol was approved by the institutional review boards at the University of Southern California and the University of Hawaii.
Statistical analysis
Cox regression was used to estimate hazard ratios (reported as relative risks (RRs)) for the effect of diabetes on colorectal cancer incidence. Models were stratified by age at entry of the cohort, and were minimally adjusted for ethnicity and sex, or further adjusted for the following risk factors as potential confounders: body mass index (BMI) (<23, ⩾23–25, ⩾25–30, ⩾30–35, ⩾35 kg m−2 and missing), smoking status (never, past, current and missing), educational level (⩽12 years, some college or vocational, college graduate and missing), alcohol intake (never, <12, 12–24 and ⩾24 g per day and missing), non-steroidal anti-inflammatory drugs (NSAIDs) use (yes, no and missing), saturated fat intake (categorised by quartiles of the distribution of percent of calories from saturated fat; ⩽7.0%, >7.0–8.8%, >8.8–10.6%, >10.6% and missing), non-saturated fat intake (categorised by quartiles of the distribution of percent of calories from non-saturated fat; ⩽17.8%, >17.8–21.2%, >21.2–24.5%, >24.5% and missing), dietary fibre intake (categorised by quartiles of the distribution of dietary fibre intake; ⩽8.7, >8.7–11.3, >11.3–14.5, >14.5 g kcal−1 and missing), total calories (categorised by quartiles of the distribution of calories intake per day; ⩽1417.8, >1417.8–1918.9, >1918.9–2608.9, >2608.9 kcal per day and missing), vigorous activity (never, ⩽0.21, >0.21–0.71, >0.71 hours per day and missing), family history of colorectal cancer (yes and no), menopausal status and hormone replacement therapy (HRT) use (premenopausal, postmenopausal never HRT users, postmenopausal past HRT users, postmenopausal current HRT users, and those missing information on menopause status or HRT use) among women only. For each covariate, an indicator variable was used for those missing data.
RRs were estimated separately for colon and rectal cancer, by location in the colon (left vs right; 31 men and 42 women were missing information for this variable and were excluded from this analysis) and by stage (localised vs regional/distant; 190 men and 213 women were missing information for this variable and were excluded from this analysis). We also examined whether the association may be modified by known risk factors (at baseline): age (<60, 60–69 and ⩾70 years), BMI (<25 and ⩾25 kg m−2; 881 men and 2704 women were missing information for BMI and were further excluded from this analysis), smoking status (never, past and current; 1034 men and 2145 women were missing information for smoking status and were further excluded from this analysis) and NSAIDs use (yes and no; 2984 men and 5701 women were missing information for NSAIDs use and were further excluded from this analysis).
The risk of colorectal cancer in diabetics has been reported to be highest 10–15 years after diabetes diagnosis, with risk declining in later years perhaps as a result of hypoinsulinemia (La Vecchia et al, 1997; Le Marchand et al, 1997; Hu et al, 1999). In an attempt to assess the association between time since diabetes diagnosis and colorectal cancer risk, we performed analysis comparing colorectal cancer risk in long-term and short-term diabetics. Subjects who reported a diabetes diagnosis before 1994 were considered to have a long duration of diabetes, and those who reported a diabetes diagnosis in or after 1994 were considered to have a short duration of diabetes. In this analysis, we began the follow-up at the time the second questionnaire was returned (2001). In all, 5344 diabetic men and 5842 diabetic women were missing information for diagnosis year of diabetes or did not return the second questionnaire, or had colorectal cancer before the return date of the second questionnaire and thus were excluded from this analysis. After exclusion, 9716 diabetic men and 10 429 diabetic women were included in this analysis.
Results
The mean age of the men (n=89 478) at baseline of the cohort was 60.2 years (s.d., 8.9), which ranged from 57.2 years for Native Hawaiians to 62.5 years for African Americans. The prevalence of diabetes varied widely across populations, from 9.5% in European Americans to 21.6% in Latinos. Diabetic men were slightly older than non-diabetic men for each racial/ethnic group, ranging from 62.7 years (vs 59.2 in non-diabetics) in European Americans to 61.9 years (vs 60.3 in non-diabetics) in Latinos. Among men, the age-standardised incidence rate of colorectal cancer was higher in diabetics than non-diabetics among European Americans, African Americans, Japanese Americans and Latinos, but lower in Native Hawaiians. In each population, diabetic men were more likely to be overweight and less physically active than men without diabetes (Table 1).
The mean age of the women (n=109 664) was 59.7 years (s.d., 8.9), with Native Hawaiians being the youngest (mean, 56.7 years) and Japanese and African Americans being the oldest (mean, 61.4 years; Table 1). Among women, the prevalence rate of diabetes was lowest in European Americans (7.8%) and highest in African Americans (20.0%). Likewise, the mean age of diabetic women at baseline was greater than non-diabetic women. Age-standardised rates of colorectal cancer in women were greater in diabetics than non-diabetics for all populations except Native Hawaiians. Among women, obesity and physical inactivity were consistently associated with diabetes across populations (Table 1).
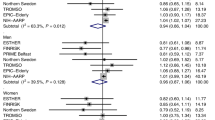
The associations noted by race and sex were not materially modified after adjustment for potential risk factors for colorectal cancer; none of the risk factors served as strong independent confounders of the association between colorectal cancer risk and diabetes (Table 2). In multivariate analyses, the RR of colorectal cancer in diabetics was 19% higher compared with non-diabetics (RR=1.19, 95% confidence interval (CI)=1.09–1.29, P<0.001; Table 2). The RR was greater and more significant in women (RR=1.28, 95% CI=1.12–1.46, P<0.001) than in men (RR=1.12, 95% CI=0.99–1.26, P=0.063; PInteraction=0.071). A positive association between diabetes and colorectal cancer risk was noted in all ethnic groups except among Native Hawaiians, with the RR estimates ranging from 1.16 in European Americans (95% CI=0.91–1.48, P=0.24) and African Americans (95% CI=0.97–1.38, P=0.097) to 1.27 in Japanese Americans (95% CI=1.09–1.47, P=0.002). Risk was non-significantly lower in Native Hawaiians (RR=0.89, 95% CI=0.62–1.27, P=0.52); however, a test of heterogeneity suggested no significant difference in the risk estimates across ethnic groups (PInteraction=0.43) (Table 2).
In analyses stratified by cancer site (colon vs rectum) (Table 2), risk of colon cancer was elevated in diabetics (RR=1.20, 95% CI=1.09–1.32, P<0.0001) as was rectal cancer risk (RR=1.15, 95% CI=0.96–1.36, P=0.12). Test of heterogeneity by ethnicity was not significant for colon cancer (PInteraction=0.30) or for rectal cancer (PInteraction=0.18). However, for rectal cancer, a particularly strong association between cancer risk and diabetes was observed only in Latinos (RR=1.55, 95% CI=1.13–2.14, P=0.007) (Table 2), with the association noted in Latino men (RR=1.51, 95% CI=1.00–2.27, P=0.050) and women (RR=1.61, 95% CI=0.97–2.69, P=0.067) (Supplementary Tables 1 and 2). The risk of cancer associated with diabetes was elevated and similar in magnitude for cancer in the right colon (RR=1.23, 95% CI=1.08–1.41, P=0.002) and in the left colon (RR=1.18, 95% CI=1.01–1.38, P=0.040). For both locations, tests of heterogeneity suggested no difference across ethnic groups (Table 2).
In analyses by stage (Table 2), there were significant increases in risk for both regional/distant cancer and localised cancer (RR=1.21, 95% CI=1.06–1.39, P=0.005 for localised cancer; RR=1.14, 95% CI=1.01–1.30, P=0.036 for regional/distant cancer). No significant heterogeneity across ethnic groups was observed by stage. For regional/distant colorectal cancer, the RR was similar in men (RR=1.15, 95% CI=0.97–1.36, P=0.10) and women (RR=1.14, 95% CI=0.94–1.37, P=0.19); whereas for localised cancer, there was no significant increase in risk observed in diabetic men (RR=1.06, 95% CI=0.88–1.27, P=0.55), but the risk was significantly increased in diabetic women (RR=1.44, 95% CI=1.18–1.76, P<0.001; PInteraction=0.0098) (Supplementary Tables 1 and 2).
We observed no significant difference in the association between diabetes status and colorectal cancer risk by BMI (⩾25 kg m−2: RR=1.21, 95% CI=1.09–1.34; <25 kg m−2: RR=1.23, 95% CI=1.05–1.45, PInteraction=0.14; Table 3). Nor were significant differences noted in the association when stratified by age, NSAIDs use, or HRT use (among women). However, we found that the association between diabetes status and colorectal cancer risk differed significantly by smoking status (PInteraction=0.0044). The association was strongest in never smokers, with a RR of 1.32 (95% CI=1.15–1.53, P<0.001); in past smokers, the RR was 1.19 (95% CI=1.05–1.34, P=0.007); no positive association was observed in current smokers (RR=0.90, 95% CI=0.70–1.15, P=0.40). This pattern was generally consistent in both sexes and in all colorectal cancer subgroups (Supplementary Table 3), and a significant interaction between tobacco use and diabetes status was observed in men, and for regional/distant colorectal cancer and rectal cancer. We observed no heterogeneity by ethnicity within a defined strata for any risk factor (e.g. current smokers; Table 3).
We also investigated the relationship between time since diagnosis with diabetes and colorectal cancer risk. Compared with diabetics diagnosed in 1994 or later, those with an earlier diagnosis were at non-significantly lower risk of colorectal cancer risk (RRlong-duration vs short-duration=0.89, 95% CI=0.69–1.14, P=0.35).
Discussion
In the prospective analysis of five racial/ethnic populations in the Multiethnic Cohort, we found a highly statistically significant association between diabetes status and colorectal cancer incidence, with diabetics having 19% greater risk of developing colorectal cancer than non-diabetics after adjusting for known risk factors. The risk associated with diabetes was slightly greater in women (RR=1.28) than in men (RR=1.12) (PInteraction=0.071), and the positive association was observed in all populations except Native Hawaiians, which was the smallest group.
Only a small number of studies have investigated the relationship between diabetes and colorectal cancer risk in non-European populations and even fewer have closely examined the association by colorectal cancer site, stage and other known risk factors for colorectal cancer across multiple ethnic groups. Our findings in Japanese Americans suggested that risk of colorectal cancer was elevated in diabetics in both men and women (RR=1.15, 95% CI=0.95–1.39 in men and RR=1.49, 95% CI=1.18–1.91 in women), which is consistent with earlier reports in Koreans and Singapore Chinese (Jee et al, 2005; Seow et al, 2006). In contrast to earlier report of no association with colon or rectal cancer among African Americans (Vinikoor et al, 2009), we found that diabetes was significantly associated with colon cancer risk in African Americans (RR=1.24, 95% CI=1.02–1.49), but not with rectal cancer risk (RR=0.85, 95% CI=0.54–1.32). We also found no evidence of an association of diabetes and colorectal cancer risk in Native Hawaiians, which has not been reported before.
In analyses by cancer site, risk was significantly increased for colon cancer, cancer of the right colon and left colon. Non-significant overall positive associations were observed for rectal cancer. For cancer of the rectum, although the test for interaction suggested no heterogeneity in the association across ethnic groups, we did notice that the risk or colorectal cancer association with diabetes was significantly elevated in Latinos (RR=1.51 in men and RR=1.61 in women), but not in any of the other ethnic groups. In analyses by stage, significant increases in risks were noted for both regional/distant and localised disease. Risks within tumour subgroups were generally consistent across ethnic groups. The relationship between diabetes status and colorectal cancer was significantly modified by smoking status. In contrast to an earlier report of greater colorectal cancer risk in current and former smokers than never smokers among diabetics (Limburg et al, 2006; Gibbs et al, 2007), the association in our study was stronger in never smokers (RR=1.32) than in past smokers (RR=1.19), whereas no positive association was observed in current smokers (RR=0.90). With smoking being a risk factor for colorectal cancer, it is possible that the association between diabetes and colorectal cancer risk may be more apparent in those at lower risk. Additional studies will be needed to better understand this observation.
In this study, diabetes status was based on self-report, which may have led to some misclassification of diabetics as non-diabetics. This underreporting may have resulted in an underestimate of the magnitude of the association between diabetes and colorectal cancer risk. However, earlier studies have shown that self-reported responses for many common chronic diseases such as diabetes are reliable when compared with medical records (Midthjell et al, 1992; Okura et al, 2004; Walitt et al, 2008). We could not differentiate between cases with type 1 and type 2 diabetes; however, we expect this misclassification to be minimal as type 1 diabetes is uncommon. Another limitation of our study is that the analysis did not account for incident cases of diabetes over the follow-up period. Incident cases of diabetes in the non-diabetic group during the follow-up would make the two groups more similar and therefore attenuate the true association between diabetes and colorectal cancer risk.
With ⩽13 years of follow-up, we were unable to address the effects of long-standing diabetes on colorectal cancer risk. However, we observed that diabetics diagnosed before 1994 were at lower risk of having colorectal cancer compared with those who were diagnosed with diabetes in 1994 or later (RR=0.89). These findings support the results from earlier studies (La Vecchia et al, 1997; Le Marchand et al, 1997; Hu et al, 1999) and the hyperinsulinemia-hypothesis, according to which risk of colorectal cancer should be lower in later years of diabetes as a result of hypoinsulinemia.
In this large, multiethnic prospective study, we observed consistent positive associations between diabetes and colorectal cancer risk in African Americans, Latinos, Japanese and European Americans. The lack of positive association between diabetes and colorectal cancer risk in Native Hawaiians is consistent with the relatively low rate of colorectal cancer in this group despite a high rate of diabetes (Grandinetti et al, 2007). Additional follow-up and larger studies will be needed to confirm the apparent inverse association in Native Hawaiians. These findings provide strong support for the hypothesis that diabetes is a risk factor for colorectal cancer.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Gibbs P, Steel S, McLaughlin S, Jones I, Faragher I, Skinner I, Croxford M, Johns J, Chapman M, Lipton L (2007) Type 2 diabetes mellitus, smoking, and colorectal cancer. Am J Gastroenterol 102: 909–910
Giovannucci E (1995) Insulin and colon cancer. Cancer Causes Control 6: 164–179
Grandinetti A, Kaholokula JK, Theriault AG, Mor JM, Chang HK, Waslien C (2007) Prevalence of diabetes and glucose intolerance in an ethnically diverse rural community of Hawaii. Ethn Dis 17: 250–255
Hu FB, Manson JE, Liu S, Hunter D, Colditz GA, Michels KB, Speizer FE, Giovannucci E (1999) Prospective study of adult onset diabetes mellitus (type 2) and risk of colorectal cancer in women. J Natl Cancer Inst 91: 542–547
Jee SH, Ohrr H, Sull JW, Yun JE, Ji M, Samet JM (2005) Fasting serum glucose level and cancer risk in Korean men and women. JAMA 293: 194–202
Jenab M, Riboli E, Cleveland RJ, Norat T, Rinaldi S, Nieters A, Biessy C, Tjonneland A, Olsen A, Overvad K, Gronbaek H, Clavel-Chapelon F, Boutron-Ruault MC, Linseisen J, Boeing H, Pischon T, Trichopoulos D, Oikonomou E, Trichopoulou A, Panico S, Vineis P, Berrino F, Tumino R, Masala G, Peters PH, van Gils CH, Bueno-de-Mesquita HB, Ocke MC, Lund E, Mendez MA, Tormo MJ, Barricarte A, Martinez-Garcia C, Dorronsoro M, Quiros JR, Hallmans G, Palmqvist R, Berglund G, Manjer J, Key T, Allen NE, Bingham S, Khaw KT, Cust A, Kaaks R (2007) Serum C-peptide, IGFBP-1 and IGFBP-2 and risk of colon and rectal cancers in the European Prospective Investigation into Cancer and Nutrition. Int J Cancer 121: 368–376
Kaaks R, Toniolo P, Akhmedkhanov A, Lukanova A, Biessy C, Dechaud H, Rinaldi S, Zeleniuch-Jacquotte A, Shore RE, Riboli E (2000) Serum C-peptide, insulin-like growth factor (IGF)-I, IGF-binding proteins, and colorectal cancer risk in women. J Natl Cancer Inst 92: 1592–1600
La Vecchia C, Negri E, Decarli A, Franceschi S (1997) Diabetes mellitus and colorectal cancer risk. Cancer Epidemiol Biomarkers Prev 6: 1007–1010
Le Marchand L, Wilkens LR, Kolonel LN, Hankin JH, Lyu LC (1997) Associations of sedentary lifestyle, obesity, smoking, alcohol use, and diabetes with the risk of colorectal cancer. Cancer Res 57: 4787–4794
Levi F, Pasche C, Lucchini F, La Vecchia C (2002) Diabetes mellitus, family history, and colorectal cancer. J Epidemiol Community Health 56: 479–480; author reply 480
Limburg PJ, Vierkant RA, Fredericksen ZS, Leibson CL, Rizza RA, Gupta AK, Ahlquist DA, Melton III LJ, Sellers TA, Cerhan JR (2006) Clinically confirmed type 2 diabetes mellitus and colorectal cancer risk: a population-based, retrospective cohort study. Am J Gastroenterol 101: 1872–1879
Ma J, Giovannucci E, Pollak M, Leavitt A, Tao Y, Gaziano JM, Stampfer MJ (2004) A prospective study of plasma C-peptide and colorectal cancer risk in men. J Natl Cancer Inst 96: 546–553
McKeown-Eyssen G (1994) Epidemiology of colorectal cancer revisited: are serum triglycerides and/or plasma glucose associated with risk? Cancer Epidemiol Biomarkers Prev 3: 687–695
Midthjell K, Holmen J, Bjorndal A, Lund-Larsen G (1992) Is questionnaire information valid in the study of a chronic disease such as diabetes? The Nord-Trondelag diabetes study. J Epidemiol Community Health 46: 537–542
Nilsen TI, Vatten LJ (2001) Prospective study of colorectal cancer risk and physical activity, diabetes, blood glucose and BMI: exploring the hyperinsulinaemia hypothesis. Br J Cancer 84: 417–422
Okura Y, Urban LH, Mahoney DW, Jacobsen SJ, Rodeheffer RJ (2004) Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J Clin Epidemiol 57: 1096–1103
Otani T, Iwasaki M, Sasazuki S, Inoue M, Tsugane S (2007) Plasma C-peptide, insulin-like growth factor-I, insulin-like growth factor binding proteins and risk of colorectal cancer in a nested case-control study: the Japan public health center-based prospective study. Int J Cancer 120: 2007–2012
Renehan AG, Zwahlen M, Minder C, O’Dwyer ST, Shalet SM, Egger M (2004) Insulin-like growth factor (IGF)-I, IGF binding protein-3, and cancer risk: systematic review and meta-regression analysis. Lancet 363: 1346–1353
Sandhu MS, Dunger DB, Giovannucci EL (2002) Insulin, insulin-like growth factor-I (IGF-I), IGF binding proteins, their biologic interactions, and colorectal cancer. J Natl Cancer Inst 94: 972–980
Schoen RE, Weissfeld JL, Kuller LH, Thaete FL, Evans RW, Hayes RB, Rosen CJ (2005) Insulin-like growth factor-I and insulin are associated with the presence and advancement of adenomatous polyps. Gastroenterology 129: 464–475
Seow A, Yuan JM, Koh WP, Lee HP, Yu MC (2006) Diabetes mellitus and risk of colorectal cancer in the Singapore Chinese Health Study. J Natl Cancer Inst 98: 135–138
Vinikoor LC, Long MD, Keku TO, Martin CF, Galanko JA, Sandler RS (2009) The association between diabetes, insulin use, and colorectal cancer among Whites and African Americans. Cancer Epidemiol Biomarkers Prev 18: 1239–1242
Walitt BT, Constantinescu F, Katz JD, Weinstein A, Wang H, Hernandez RK, Hsia J, Howard BV (2008) Validation of self-report of rheumatoid arthritis and systemic lupus erythematosus: the Women's Health Initiative. J Rheumatol 35: 811–818
Will JC, Galuska DA, Vinicor F, Calle EE (1998) Colorectal cancer: another complication of diabetes mellitus? Am J Epidemiol 147: 816–825
Yang YX, Hennessy S, Lewis JD (2005) Type 2 diabetes mellitus and the risk of colorectal cancer. Clin Gastroenterol Hepatol 3: 587–594
Acknowledgements
This work was supported by the National Cancer Institute (grant number CA54281). We are indebted to the participants of the Multiethnic Cohort for their ongoing commitment to the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on British Journal of Cancer website
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
He, J., Stram, D., Kolonel, L. et al. The association of diabetes with colorectal cancer risk: the Multiethnic Cohort. Br J Cancer 103, 120–126 (2010). https://doi.org/10.1038/sj.bjc.6605721
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6605721
Keywords
This article is cited by
-
Factors affecting participation in the colorectal cancer screening program: a cross-sectional population study
Journal of Cancer Research and Clinical Oncology (2023)
-
Associations of Albumin and BMI with Colorectal Cancer Risk in the Southern Community Cohort Study: a Prospective Cohort Study
Journal of Racial and Ethnic Health Disparities (2023)
-
Geographic Distribution and Time Trends of Colorectal Cancer in Brazil from 2005 to 2018
Digestive Diseases and Sciences (2022)
-
Circulating soluble receptor for advanced glycation end products and other factors in type 2 diabetes patients with colorectal cancer
BMC Endocrine Disorders (2020)
-
Diabetes mellitus and colorectal carcinoma outcomes: a meta-analysis
International Journal of Colorectal Disease (2020)
