
Abstract
Study Design:
A cross-sectional descriptive study was performed with structured questionnaires and interviews conducted with 60 primary caregivers of persons with paraplegia (T1 to S2) owing to traumatic spinal cord injury (SCI).
Objectives:
The purpose of this study was the assessment of the health-related quality of life (HRQoL) of primary caregivers of persons with paraplegia owing to traumatic SCI.
Setting:
São Paulo, SP, Brazil.
Methods:
The HRQoL was assessed by the Short Form-36 (SF-36) health survey questionnaire and caregiver burden was evaluated by the Caregiver Burden Scale (CBS).
Results:
Among 60 caregivers evaluated, 49 (81.7%) were female, with mean age of 35.8 (SD=12.91) years, 16 (26.6%) being wives and 14 (23.4%) sisters of persons with paraplegia. It was found that the caregivers spend an average of 11.3 h/day caring for individuals with paraplegia. Twenty-three caregivers (38.3%) had a chronic disease and 32 (53.3%) were sole caregivers taking upon themselves the full responsibility of caring for the persons with paraplegia. The subjects reported lower scores on bodily pain and vitality than the other dimensions of the SF-36. The mean global CBS score was 1.71 (SD=0.50) and mean scores for each dimension ranged from 1.39 (SD=0.64) for emotional involvement to 2.44 (SD=0.79) for environment dimension.
Conclusion:
The primary caregivers of spinal cord-injured persons reported low scores on all of the SF-36 and CBS dimensions, bodily pain and vitality being the SF-36 dimensions that received the lowest scores.
Sponsorship:
Funding was provided by the Brazilian research agency CAPES.
Similar content being viewed by others

Introduction
For almost three decades, more attention has been given in the literature to family caregivers of elderly persons with physical or mental disability, especially in the study of the impact the disease has on their lives. The diagnosis of a severe disease, as well as an accident that results in disability, such as spinal cord injury (SCI), not only affect the patient but also the whole family. In this way, the person with the disability as well as the family group goes through a process of loss and grief.1, 2
The measurement of health-related quality of life (HRQoL) of caregivers of patients with traumatic SCI provides relevant information on social, psychological, emotional and physical aspects.
Health problems faced by caregivers and their consequences may have impact on the patients' HRQoL. As the caregiver is the key to maintaining the patient in the community, both prevention and treatment of health problems among caregivers may help to reduce the need for hospitalization of patients or, at least, increase the time between admissions.3
The purpose of this study was to contribute additional information concerning HRQoL of caregivers of patients with traumatic SCI. This information could help to establish interventions to improve the HRQoL of caregivers and, consequently, to influence positively the care provided to patients.
Materials and methods
This is a cross-sectional descriptive study. The data were collected among 60 primary caregivers of persons with traumatic SCI who live in São Paulo, a city of approximately 10 million inhabitants. Unfortunately, the statistics on the number of persons with paraplegia and respective caregivers living in this area are not known. The data were collected between January and May 2005.
Caregivers, who accompanied outpatients with paraplegia to routine office visits in clinical settings, such as the Clinic of Urology and Plastic Surgery at the São Paulo Hospital and two rehabilitation centers, were interviewed at these locations and also at their residences.
The following inclusion criteria were to be met: age over 18 years; be an unpaid caregiver and a primary caregiver for more than 1 year of a person with traumatic SCI. The person with traumatic SCI must currently be an outpatient aged between 18 and 60 years.
To obtain relevant information, the patient with paraplegia was initially contacted and informed about the purpose of the study; it was verified if the cause of the injury was traumatic and whether the patient and his caregiver met the inclusion criteria.
The primary caregiver was identified by the patient based on the following definition: ‘The person who is primarily involved in the care of the patient and provides the most support and/or assistance.’
A letter containing information about the study, written in simple and clear language, was read to the participants and the informed consent form was signed by the subjects. Confidentiality was assured. All caregivers confirmed they were the primary person involved in the care of the patient.
Interviews were conducted with all subjects in which the Short Form-36 (SF-36) health survey questionnaire for HRQoL4 and the Caregiver Burden Scale (CBS)5 were completed.
The SF-36 questionnaire contains 35 items grouped into eight dimensions as follows: physical function (10 items), role physical (four items), bodily pain (two items), general health (five items), vitality (four items), social function (two items), emotional role (three items) and mental health (five items).4 Scores on each dimension range from 0 to 100, where 0 corresponds to the worst health status and 100 to the best health status. SF-36 also includes an additional item, which asks subjects about the change in their health status over the past year. This 36th item is not scored.6
The CBS was used to measure subjectively the effect of the patients' illness on the caregivers' life. It has 22 items grouped into five dimensions: general strain, isolation, disappointment, emotional involvement and environment.5 Each question offers alternative answers consisting of never, seldom, sometimes and frequently, with values ranging from 1 to 4, respectively. The individual score is obtained by the arithmetic mean of the values that correspond to the specific answers of each dimension, ranging from 1 to 4; the higher the value of the individual score, the higher will be the impact felt by the caregiver in the specific dimension. The mean global score is obtained by the arithmetic mean of the values that correspond to the 22 items.
Student's t-test for independent samples was used to compare the means between two groups and the variance analysis was applied to compare data from more than two groups. The correlation among numeric variables was assessed using Pearson's linear coefficient. A P⩽0.05 or 5% was considered significant.
This study was analyzed and approved by the Research Ethics Committee of the Federal University of São Paulo, Brazil.
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Results
The sample was constituted by 60 primary caregivers of persons with traumatic SCI. The subjects were predominantly female (81.7%), aged from 18 to 60 years, with a mean of 35.8 (SD=12.91) years. Most of the caregivers (51.7%) were married and had low level of education (53.3%) (Table 1). All caregivers were relatives of the patients and, among them, 16 (26.6%) were wives, 14 (23.4%) sisters and 11 (18.4%) mothers. Other characteristics of the caregivers are shown in Table 2.
Most of the 60 outpatients with paraplegia involved in this study were male (86.7%), single (61.7%), with a mean age of 32.9 (SD=9.47) years and had low level of education (63.3%). Although 41.7% were born in different states, all patients were current residents of São Paulo. The most frequent causes of paraplegia were firearm injury (63.3%) followed by motor vehicle accident (20%). The levels of SCI, according to the American Spinal Injury Association (ASIA) classification, varied from T1 to T10 (80%), T11 to L2 (16.7%) and L3 to S2 (3.3%). The most frequent complications observed in the patients were urinary (88.3%) and anal (45%) incontinence, muscle spasm (65%) and pressure ulcers (26.7%).
Table 3 shows caregivers' scores on the SF-36 dimensions. The dimensions that received the lowest scores were bodily pain and vitality.
Statistical differences were found for caregivers with chronic diseases within the following dimensions: physical function (P=0.001), bodily pain (P=0.003), general health (P=0.004), vitality (P=0.007) and mental health (P=0.024), according to the Student's t-test.
The mean global score and the mean scores of five CBS dimensions are presented in Table 4.
On a scale ranging from 1 to 4, the mean global score was 1.71 (SD=0.50), and among the assessed dimensions, the mean scores ranged from 1.39 (SD=0.64) for emotional involvement to 2.44 (SD=0.79) for environment. Among single caregivers, a statistically significant difference was observed in the isolation dimension (P=0.017), using variance analysis.
No significant difference was found in the mean scores of any other social–demographic or clinical characteristics.
No statistical association was found when the Pearson's linear correlation was applied.
Discussion
About 90% of the caregivers of persons with chronic diseases are their relatives.7, 8 Most of the time the caregiver is a woman, usually the wife or daughter, aged between 29 and 68 years, from different social groups, who has been providing care for periods ranging from months to decades and, generally, lives with the patient.9, 10
In this study, differently from studies evaluating the care of elderly people,9, 11 it was found that, besides the spouses (26.6%), there is also the presence of sisters (23.4%) and mothers (18.3%) acting as caregivers, probably because the person with paraplegia is usually young (mean=32.9 years).
These results are similar to the ones found by De Vivo and Fine12 in a study of persons with SCI, in which wives are highlighted as the primary caregivers and, less frequently, the other relatives. Generally, it is the wife who carries the burden of care. Chan13 evaluated wives of individuals with SCI and detected a high frequency of stress and depressive feelings. According to De Vivo and Fine,12 the divorce rate after injury is high, ranging from 8 to 48%. De Vivo et al14 evaluated 622 persons enrolled in the National Spinal Cord Injury Statistical Center (USA) data set since 1973, finding a total of 126 divorces, which compares to the 74 expected, based on the age-sex-specific annual divorce rates for the United States population.
In this study, it was found that the caregiver spends an average of 11.3 h per day caring for the person with SCI, which reflects an almost complete dedication, and is also responsible for housekeeping tasks and the care of other dependent family members. In Brazil, it is part of the culture to provide total support to relatives with disabilities or with special needs. Belasco and Sesso15 reported an average of 8 h/day spent by caregivers in the care of patients who need hemodialysis. Even if most of the primary caregivers (73.3%) work outside their homes, some of them (26.7%) were retired or housewives, with no job-related activity outside their residences. In Brazil, there is a high level of unemployment, especially among the population with low level of education, and usually these individuals are self-employed, engaged in informal activities such as manicure and laundress, among others. In this way, a person may work sporadically to maintain a minimum income and, at the same time, have a flexible schedule that allows her to care for the disabled person.
The answers given in the interviews indicated that 38.3% of the caregivers of persons with paraplegia suffer from chronic diseases. Previous studies suggest that physical complaints of caregivers are frequently of psychosomatic origins.16, 17, 18
Caregivers tend to develop more psychopathology than physical illness, make more visits to physicians and report worse health than the general population.15
Over half of the subjects (53.3%) in this study were sole caregivers, taking upon themselves the full responsibility not only of caring for the individuals with paraplegia but also of housekeeping tasks without any help from a secondary caregiver.
Nowadays, the quality of life has become a major topic of research in the area of health and the findings contribute to the definition and approval of treatments and evaluation of cost benefits of the care given.
The HRQoL of caregivers of patients with SCI was measured by the SF-36 and results showed a greater impact on the physical component than the mental component. The most influenced individual dimensions were bodily pain (mean=65.05) and vitality (mean=65.58), which showed the lowest values in a scale ranging from 0 to 100.
Statistical differences were found for caregivers with chronic diseases within the following dimensions: physical function (P=0.001), bodily pain (P=0.003), general health (P=0.004), vitality (P=0.007) and mental health (P=0.024), according to the Student's t-test.
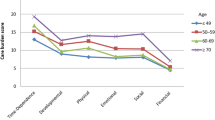
Table 4 shows that the CBS dimensions with the highest mean scores were environment (2.44), disappointment (1.74) and general strain (1.59).
In this study, the questions that most influenced the increase of the environment dimension scores were question 22: ‘Is there any problem in the neighborhood in which your relative lives (eg, lack of accessible transportation, difficult access to drug stores and/or medical services, problems with neighbors) that makes it difficult for you to care for that person?’ and question 20: ‘Does your home environment make it difficult for you to care for your relative?’, in agreement with Medeiros et al.1
Considering that individuals with SCI need wheelchairs or bath chairs, special adaptations are required at home and in public facilities. Some environmental changes have been done to accommodate people with disabilities, but reduced public transportation access and buildings and sidewalks without ramps for wheelchairs appear to be some of the problems that mostly affect the caregiver and, consequently, the person with SCI.
Relative caregivers who were receiving help reported greater degree of satisfaction with their lives than those who were not receiving help.19 Therefore, one could expect that caregivers who live in places where there is a lack of appropriate support, accessible public transportation and difficult access to medical and social assistance, would show greater influence on items related to the environment.
In Sweden, Elmsthal et al5 evaluated caregivers of elderly dependent persons with stroke who needed a convenient environment adapted to their particular needs. The study was performed in a developed country with higher socio-economic indicators than Brazil, which probably provides better access to health services and a more convenient environment for disabled people. Environment scores reported in Brazilian studies1, 15 were higher than Swedish ones,5 indicating a higher level of burden for Brazilian caregivers related to environmental factors.
The subjective impact of the disease on the caregiver is an extremely complex issue where several factors are inter-related, including the cultural context of the studied population.
As only few studies2, 20 have investigated the HRQoL of caregivers of persons with paraplegia in Brazil, and the dynamics of caregiver burden was not evaluated here, as this was a cross-sectional study, we consider this research as a preliminary study, indispensable and that can yield valuable information that may clarify many important questions related to caregivers of persons with paraplegia. The results obtained may lead to the elaboration of strategies to reduce the impact caused by the disease in the life and health of caregivers of persons with paraplegia and, consequently, improve their HRQoL.
Among these strategies, the types of assistance that are receiving increased attention in the area of health are rehabilitation centers for people with physical disabilities or chronic diseases, home care assistance and health education to enable lay people to coordinate some techniques, which were formerly performed only by hospital professionals.
Conclusion
The primary caregivers of spinal cord-injured persons reported low scores on all of the SF-36 and CBS dimensions, with bodily pain and vitality being the SF-36 dimensions that received the lowest scores. These findings indicate that community services should not only be oriented toward the needs of the person with disability but also to the needs of the caregivers.
References
Medeiros MMC, Ferraz MB, Quaresma MR . The effect of rheumatoid arthritis on the quality of life of primary caregivers. J Rheumatol 2000; 27: 76–83.
Azevedo GR, Santos VLCG (Handicapped). Caregiver: the social representations of family members about the caregiving process. Rev Latino-am Enfermagem 2006; 14: 770–780.
Baumgarten M . The health of persons giving care to the demented elderly: a critical review of the literature. J Clin Epidemiol 1989; 42: 1137–1148.
Stewart AL, Hays RD, Ware JE . The MOS Short Form General Health Survey: reliability and validity in a patient population. Med Care 1988; 26: 724–735.
Elmstahl S, Malmberg B, Annerstedt L . Caregiver's burden of patients 3 years after stroke assessed by a novel caregiver burden scale. Arch Phys Med Rehabil 1996; 77: 177–182.
Ciconelli RM, Ferraz MB, Santos W, Meinão I, Quaresma MR . Brazilian-Portuguese version of the SF-36, A reliable and valid quality of life outcome measure. Rev Bras Reumatol 1999; 39: 143–150.
Ehrlich F, Bowring G, Draper B, Poulos C, Salgado R . Caring for carers – a national problem. Med J Aust 1992; 156: 590–592.
Corcoran MA . Management decisions made by caregiver spouses of persons with Alzheimer's disease. Am J Ocup Ther 1994; 48: 38–45.
Zarit SH, Todd P, Zarit J . Subjective burden of husbands and wives as caregivers: a longitudinal study. Gerontologist 1986; 26: 260–266.
Fink SV . The influence of family resources and family demands on the strains and well-being of caregiving families. Nurs Res 1995; 44: 139–146.
Russo J, Vitalino PP, Brewer DD, Katon W, Becker J . Psychiatric disorders in spouse caregivers of care recipients with Alzheimer's disease and matched controls: a diathesis-stress model of psychopathology. J Abnorm Psychol 1995; 104: 197–204.
De Vivo MJ, Fine PR . Spinal Cord Injury: its short-term impact on marital status. Arch Phys Med Rehabil 1985; 66: 501–504.
Chan RC . Stress and coping in spouses of persons with spinal cord injuries. Clin Rehabil 2000; 14: 137–144.
De Vivo MJ, Hawkins LN, Richards JS, Go BK . Outcomes of post-spinal cord injury marriages. Arch Phys Med Rehabil 1995; 76: 130–138.
Belasco AG, Sesso R . Burden and quality of life of caregivers for hemodialysis patients. Am J Kidney Dis 2002; 39: 805–812.
Karlin NJ, Retzlaff PD . Psychopathology in caregivers of the chronically ill: personality and clinical syndromes. Hosp J 1995; 10: 55–61.
Schulz R, O'Brien AT, Bookwala J, Fleissner K . Psychiatric and physical morbidity effects of dementia caregivers: prevalence, correlates and causes. Gerontologist 1995; 35: 771–791.
Ünalan H et al. Quality of life of primary caregivers of spinal cord injury survivors living in the community: controlled study with short form-36 questionnaire. Spinal cord 2001; 39: 318–322.
Potaszniz H, Nelson G . Stress and social support: the burden experienced by the family of a mentally ill person. Am J Community Psychol 1984; 12: 589–607.
Faro ACM . Atividades realizadas no domicílio pelo cuidador familiar da pessoa com lesão medular. Rev Paul Enf 2001; 20: 33–42.
Acknowledgements
We thank the Brazilian Foundation for the Coordination of the Improvement of Higher Education Personnel (CAPES) for the financial support for this work.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Blanes, L., Carmagnani, M. & Ferreira, L. Health-related quality of life of primary caregivers of persons with paraplegia. Spinal Cord 45, 399–403 (2007). https://doi.org/10.1038/sj.sc.3102038
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3102038
Keywords
This article is cited by
-
Labor market costs for long-term family caregivers: the situation of caregivers of persons with spinal cord injury in Switzerland
BMC Health Services Research (2023)
-
Caregiver burden according to ageing and type of care activity in caregivers of individuals with spinal cord injury
Spinal Cord Series and Cases (2023)
-
Burden in caregivers of spinal cord injury patients: a systematic review and meta-analysis
Acta Neurologica Belgica (2022)
-
Family reported outcomes, an unmet need in the management of a patient's disease: appraisal of the literature
Health and Quality of Life Outcomes (2021)
-
Is caregiver quality of life predicted by their perceived burden? A cross-sectional study of family caregivers of people with spinal cord injuries
Spinal Cord (2021)
