
Abstract
Accumulation of protein-bound uraemic toxins (PBUTs) is one of the reasons for the development of uraemia-related complications including cardiovascular disease; however, conventional haemodialysis is limited in its ability to remove PBUTs. We aimed to examine whether the oral charcoal adsorbent AST-120 has an additive effect on PBUT removal in haemodialysis patients. During the 4-week study, anuric patients undergoing haemodialysis received AST-120 (6 g/day) in the last 2 weeks (n = 10) or the first 2 weeks (n = 10). Serum levels of total and free PBUTs such as indoxyl sulfate, p-cresyl sulfate and phenyl sulfate at the pre- and postdialysis sessions were measured before and after AST-120 use and after discontinuation. Levels of the oxidative stress markers oxidized albumin and 8-isoprostane were also measured. AST-120 use induced dramatic reduction of indoxyl sulfate (total, 45.7% [33.2–50.5%]; free, 70.4% [44.8–79.8%]), p-cresyl sulfate (total, 31.1% [25.0–48.0%]; free, 63.5% [49.3–70.9%]) and phenyl sulfate (free, 50.6% [32.3–71.2%]) levels; however, this effect disappeared after the discontinuation of AST-120. AST-120 use also induced substantial reduction of the oxidized albumin and 8-isoprostane levels. In conclusion, oral administration of AST-120 had additive effects on the continuous reduction of some PBUTs in anuric patients undergoing haemodialysis.
Similar content being viewed by others
Introduction
An accumulation of uraemic toxins is associated with chronic kidney disease (CKD)-related complications including cardiovascular disease, especially in patients undergoing dialysis treatment1,2,3. With the development in dialysis therapies, removal of low- and middle molecular-weight water-soluble molecules has been improving; however, conventional haemodialysis treatment is limited in its ability to remove protein-bound uraemic toxins (PBUTs) owing to binding to large molecular proteins4. For example, the protein-binding rate of indoxyl sulfate (IS), a representative PBUT, is 97.7% and the reduction rate with regular haemodialysis treatment is 31.8%5. Several clinical studies suggested that IS and p-cresyl sulfate (PCS) were related to cardiovascular mortality in CKD and dialysis patients1,2 and the accumulation of IS or PCS is related to the increase in oxidative stress3,6,7. Thus, additional therapeutic strategies will be needed to reduce PBUT levels for preventing CKD-related complications.
The oral charcoal adsorbent AST-120 is known to reduce the serum levels of IS through the adsorption of indole converted from dietary tryptophan in the gastrointestinal tract. AST-120 use was reported to decrease the IS levels in a dose-dependent manner in nondialysis CKD patients8. This report suggests that AST-120 use may have a greater beneficial effect on the decrease in PBUTs in anuric patients undergoing maintenance dialysis treatment because they have higher levels of PBUTs1,5.
In this study, we investigated whether oral administration of AST-120 induced the reduction of several PBUTs in anuric patients undergoing maintenance haemodialysis. We also assessed the subsequent effects of AST-120 use on some oxidative stress markers.
Results
Baseline characteristics
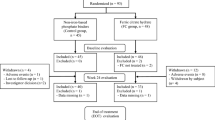
The median age of the patients was 63.0 (58.3–65.0) years. Women accounted for 40.0% of the study population. The median duration of dialysis was 15.5 (8.0–20.8) years and the patients had no residual kidney function. The patients were divided into 2 groups, i.e. Group I (n = 10) and Group II (n = 10), which were similar in terms of demographic, dialysis and laboratory characteristics (Table 1).
Uraemic toxins in haemodialysis patients treated with AST-120
During the 4-week study, haemodialysis patients received AST-120 (6 g/day) in the last 2 weeks (Group I) or the first 2 weeks (Group II) of the study. No adverse effects of AST-120, such as constipation, loss of appetite and nausea, were reported in the participants by using a questionnaire. In Group I, the serum levels of total and free IS before the dialysis session were 3.09 mg/dL (2.80–4.62 mg/dL) and 0.106 mg/dL (0.055–0.136 mg/dL), respectively and the protein-binding rate was 97.1% (96.6–97.9%), which is similar to that reported by a previous study5. A haemodialysis session decreased the total and free IS levels to 2.16 mg/dL (1.59–2.61 mg/dL) and 0.026 mg/dL (0.018–0.036 mg/dL), respectively, whereas regular haemodialysis treatment maintained a high serum level of IS in the predialysis session. However, use of AST-120 (6 g/day) for 2 weeks dramatically decreased the total and free IS levels in the predialysis session (total IS: 1.62 mg/dL [1.31–2.48 mg/dL]; free IS: 0.027 mg/dL [0.017–0.040 mg/dL]) and the low levels were maintained between dialysis sessions (Fig. 1A,D). In Group II, use of AST-120 (6 g/day) for 2 weeks decreased the total and free IS levels in the predialysis session (total IS: 2.55 mg/dL [1.34–3.27 mg/dL] before treatment and 1.49 mg/dL [0.90–1.91 mg/dL] after treatment; free IS: 0.067 mg/dL [0.018–0.130 mg/dL] before treatment and 0.020 mg/dL [0.009–0.043 mg/dL] after treatment). However, the total and free IS levels increased after the discontinuation of AST-120 (Fig. 1B,E). The total and free IS levels in Groups I and II in the predialysis session decreased significantly with AST-120 treatment (total IS: 1.63 mg/dL [1.19–1.98 mg/dL] vs. 3.06 mg/dL [2.08–3.74 mg/dL] before treatment, P < 0.001; free IS: 0.023 mg/dL [0.013–0.038 mg/dL] vs. 0.098 mg/dL [0.038–0.131 mg/dL] before treatment, P < 0.001) and the reduction rates of total and free IS were 45.7% (33.2–50.5%) and 70.4% (44.8–79.8%), respectively (Fig. 1C,F). When the association between the initial serum levels of IS and the reduction ratio with AST-120 treatment was evaluated, free IS, but not total IS, showed a statistically significant correlation with the reduction ratio (free IS: Rho = 0.713, P < 0.001; total IS: Rho = −0.011, P = 0.965).

Serum levels of total and free indoxyl sulfate (IS) in maintenance haemodialysis patients receiving AST-120 treatment.
Serial changes in the serum levels of total IS ((A) Group I, (B) Group II, n = 10 per group) and free IS ((D) Group I, (E) Group II, n = 10 per group) and a comparison between the serum levels before and those after AST-120 use in the predialysis session ((C) total IS, (F) free IS, n = 20). P values were calculated using the Wilcoxon signed-rank test.
The effects of AST-120 on the serum levels of PCS showed the same trend as those of AST-120 on the serum levels of IS in Group I (Fig. 2A,D) and Group II (Fig. 2B,E). The serum levels of PCS also decreased with AST-120 use (total PCS: 1.66 mg/dL [0.96–2.77 mg/dL] vs. 2.90 mg/dL [1.59–4.34 mg/dL] before treatment, P = 0.019; free PCS: 0.061 mg/dL [0.028–0.100 mg/dL] vs. 0.250 mg/dL [0.082–0.384 mg/dL] before treatment, P = 0.002) (Fig. 2C,F) and the reduction rates of total and free PCS with AST-120 treatment were 31.1% (25.0–48.0%) and 63.5% (49.3–70.9%), respectively. When the association between the initial serum levels of PCS and the reduction ratio with AST-120 treatment was evaluated, free PCS, but not total PCS, showed a statistically significant correlation with the reduction ratio (free PCS: Rho = 0.584, P = 0.007; total PCS: Rho = 0.438, P = 0.054).

Serum levels of total and free p-cresyl sulfate (PCS) in maintenance haemodialysis patients receiving AST-120 treatment.
Serial changes in the serum levels of total PCS ((A) Group I, (B) Group II, n = 10 per group) and free PCS ((D) Group I, (E) Group II, n = 10 per group) and a comparison between the serum levels before and those after AST-120 use in the predialysis session ((C) total IS, (F) free IS, n = 20). P values were calculated using the Wilcoxon signed-rank test.
Free phenyl sulfate (PS) levels decreased significantly with AST-120 treatment (0.11 mg/dL [0.05–0.20 mg/dL] vs. 0.22 mg/dL [0.11–0.44 mg/dL] before treatment, P = 0.019), whereas total PS levels did not change (0.63 mg/dL [0.29–1.26 mg/dL] vs. 0.69 mg/dL [0.40–1.82 mg/dL] before treatment, P = 0.456) (Fig. 3A,B, Supplementary Fig. 1). On the other hand, both total and free indoleacetic acid (IAA) and hippuric acid (HA) levels did not change with AST-120 treatment (Fig. 3C–F, Supplementary Figs 2 and 3).

Serum levels of total and free phenyl sulfate (PS), indoleacetic acid (IAA) and hippuric acid (HA) in maintenance haemodialysis patients receiving AST-120 treatment.
A comparison between the total and free PS, IAA and HA serum levels before and those after AST-120 use in the predialysis session ((A) total PS, (B) free PS, (C) total IAA, (D) free IAA, (E) total HA, (F) free HA, n = 20). P values were calculated using the Wilcoxon signed-rank test.
To understand the effects of AST-120 on the changes in low- and intermediate-molecular-weight water-soluble molecules, urea nitrogen and β2-microglobulin levels were measured during the study and AST-120 treatment did not decrease the levels of both urea nitrogen (62.5 mg/dL [55.2–70.8 mg/dL] vs. 65.2 mg/dL [57.4–72.4 mg/dL] before treatment, P = 0.525) and β2-microglobulin (24.2 mg/L [21.0–26.8 mg/L] vs. 24.5 mg/dL [21.4–26.8 mg/L] before treatment, P = 0.978] (Supplemental Fig. 4).
These results indicate that the use of AST-120 induced a dramatic reduction of some PBUTs, such as IS (total and free), PCS (total and free) and PS (free) in patients on maintenance haemodialysis treatment.
Oxidative stress in patients undergoing haemodialysis treated with AST-120
We also evaluated the changes in the oxidative stress markers with AST-120 treatment in patients undergoing maintenance haemodialysis. Use of AST-120 induced significant reduction in oxidized albumin content [63.4% (60.3–69.0%) vs. 68.5% (63.0–74.3%) before AST-120 treatment, P = 0.041, Fig. 4A) as well as 8-isoprostane [458.1 pg/mL (380.7–615.6 pg/mL) vs. 642.4 pg/mL (450.7–880.6 pg/mL) before AST-120 treatment, P = 0.035, Fig. 4B]. These results indicate that the use of AST-120 was related to improvement of oxidative stress in patients undergoing maintenance haemodialysis treatment.

Changes in the levels of oxidative stress markers in maintenance haemodialysis patients receiving AST-120 treatment.
A comparison between the oxidized albumin (A) and 8-isoprostane (B) levels before and those after AST-120 use in the predialysis session. P values were calculated using the Wilcoxon signed-rank test.
Discussion
In this study, anuric patients undergoing maintenance haemodialysis treatment were orally administered the charcoal adsorbent AST-120 which induced a dramatic the levels of some PBUTs. Furthermore, AST-120 use was associated with the improvement in some oxidative stress markers.
PBUTs are accumulated in CKD patients, especially in those undergoing dialysis treatment1,5. High serum levels of PBUTs, such as IS, PCS and IAA, are associated with higher rates of cardiovascular and all-cause mortality in dialysis patients1,2,9. The mechanisms through which PBUTs induce various CKD-related complications including cardiovascular disease are still incompletely understood; basic research suggests a direct interaction between those uraemic toxins and cardiovascular tissues10,11 with aggravation of oxidative stress3,6,7. However, conventional haemodialysis is limited in its ability to remove PBUTs, such as IS, IAA and HA, even with convective therapies including high-flux haemodialysis, haemofiltration and haemodiafiltration4,12, although recent preliminary data suggested that change in pH during haemodialysis may increase the removal of IS (Chun J, et al. Kidney Week 2014, 861A [2014]). Thus, an additional blood purification strategy is needed to decrease PBUT levels, which will lead to better survival in dialysis patients.
The oral charcoal adsorbent AST-120 prevents IS synthesis by inhibiting the gastrointestinal uptake of indole in nondialysis CKD patients8. Although the randomised placebo-controlled EPPIC-1 and EPPIC-2 trials did not show the beneficial effects of the use of AST-120 (9 g/day) on the endpoints including dialysis initiation, kidney transplantation and serum creatinine doubling in patients with stage 4 CKD13, we believe that these effects will be much more obvious in maintenance dialysis patients with a high level of accumulated PBUTs. Thus, we examined whether oral administration of AST-120 had an additive effect of PBUT reduction in anuric patients undergoing maintenance haemodialysis. As a result, AST-120 use with conventional haemodialysis induced a dramatic decrease in the IS (total and free), PCS (total and free) and PS (free) levels (Figs 1, 2, 3, Supplementary Fig. 1). These beneficial effects may improve survival in maintenance haemodialysis patients because high serum levels of total IS are reported to be associated with higher mortality in CKD patients1. The decrease in the free IS and PCS levels was more obvious than that in the total IS and PCS levels because AST-120 inhibits the absorption of indole or p-cresol, derived from dietary tryptophan and tyrosine respectively across the intestinal tract14,15,16, which leads to the inhibition of free IS and PCS production. Another possible mechanism is that the remaining IS and PCS contents after AST-120 treatment tend to bind to proteins, leading to an increase in the protein-binding rate. The binding saturation of free vs. total solute concentrations and competitive binding of different solutes at the same protein-binding sites should be discussed in future studies. The levels of free PS, but not total PS, decreased with AST-120 treatment (Fig. 3A,B, Supplementary Fig. 1). Similar to PCS14, PS is produced from tyrosine in the intestinal tract and the effects of AST-120 use may be partial for total PS because compared with the amounts of IS (reduction rate 34.3% [27.0–42.8%], Fig. 1A,B) and PCS (reduction rate: 32.3% [21.9–36.5%], Fig. 2A,B), large amounts of PS were removed using haemodialysis (reduction rate: 71.3% [63.5–75.7%], Supplementary Fig. 1a,b). On the other hand, AST-120 use did not change the serum levels of IAA and HA (Fig. 3C–F, Supplementary Figs 2 and 3). The mechanism of gastrointestinal production and uptake of those molecules may not be as crucial for those molecules. A recent study showed that an increase in the levels of dietary fibre led to a decrease in the plasma levels of IS (total and free) and PCS (free) in haemodialysis patients17. A previous study showed that colectomy decreased the plasma levels of IS and PCS, but not those of HA, in patients undergoing dialysis treatment18. Thus, oral administration of AST-120 showed effects mainly on uraemic toxins of colonic origin, such as IS, PCS and PS. Lee et al. also reported the effects of AST-120 on the reduction of IS and PCS levels in patients undergoing peritoneal dialysis or haemodialysis19. They analysed the data obtained from haemodialysis and peritoneal dialysis patients with residual kidney function; however, the additional effects of AST-120 on the decrease in PBUT levels in dialysis patients are unclear. In contrast, we examined the effects of AST-120 on various types of PBUTs in maintenance haemodialysis patients with no residual kidney function both before and after the dialysis session. Moreover, we observed that the PBUT levels increased again after discontinuation of the treatment. Thus, we found that AST-120 use with conventional dialysis treatment in haemodialysis patients induced a strong and continuous reduction in the levels of PBUTs of colonic origin.
AST-120 was also associated with the improvement of some oxidative stress markers (Fig. 4). This was probably because of the subsequent effects after the decrease in the PBUT levels. In an animal model, AST-120 administration modulated kidney injury-induced cardiac fibrosis through oxidative stress20. In another animal model, AST-120 administration inhibited kidney injury-induced acceleration of atherosclerosis with a decrease in IS deposition as well as inflammatory cytokine expressions in lesions21. A clinical study reported that AST-120 use improved flow-mediated endothelium-dependent vasodilatation and the oxidized glutathione/glutathione ratio in nondialysis CKD patients22. Taken together, a decrease in the PBUT levels with the use of AST-120 and conventional haemodialysis may lead to improvement of oxidative stress in maintenance haemodialysis patients.
This study has some limitations. This was a crossover trial, not a randomised placebo-controlled study. The sample size was small and the treatment duration was short, which limited our understanding of the subsequent effects of AST-120, such as oxidative stress and inflammatory reactions. Moreover, serum samples were collected only at 0, 2 and 4 weeks during the study, which limited our understanding of the time taken for the serum concentrations to be affected. Long-term observation of maintenance haemodialysis patients will be needed to understand the effects of AST-120 on uraemia-related complications including cardiovascular outcomes. However, despite the small sample size and short treatment duration, our data suggest that oral charcoal adsorbents may be used as an additional blood purification therapy to reduce PBUTs in maintenance dialysis patients.
In conclusion, oral administration of AST-120 was effective in the continuous reduction of some PBUTs and was associated with the improvement of oxidative stress in maintenance haemodialysis treatment. This adsorption treatment may be an additional blood purification therapy to prevent uraemia-related complications.
Methods
Study design and patients
We recruited 20 patients undergoing maintenance haemodialysis treatment who had no residual kidney function, from a single dialysis unit. All eligible patients received 4–5 h of haemodialysis thrice weekly with standard bicarbonate dialysate (Na+: 140 mEq/L, K+: 2.0 mEq/L, Ca2+: 2.75 mEq/L, Mg2+: 1.0 mEq/L, Cl−: 112.25 mEq/L, HCO3- 27.5 mEq/L) and 1.6–2.1 m2 dialyzers with synthetic membranes, polysulfone or polyethersulfone. The blood flow was 180–250 ml/min and dialysate flow was 500 mL/min. Dialysis adequacy was estimated by Kt/Vurea. Patients who had acute inflammatory disease, underwent haemodialysis for <1 year, and/or were <20 years old were excluded. To observe differences in patient characteristics before and after the intervention, the patients were divided into 2 groups, i.e. Group I and Group II, which did not differ in terms of age, sex and dialysis duration. In Group I patients, AST-120 was not administered for the first 2 weeks and then was administered at 6 g/day for the last 2 weeks. In Group II patients, AST-120 was administered for the first 2 weeks and then was not administered for the last 2 weeks. In this study, AST-120 was administered at 6 g/day in haemodialysis patients because in Japan, the regular dose of AST-120 in predialysis CKD patients is 6 g/day23. Serum samples were obtained from patients before and after the dialysis sessions at 0, 2 and 4 weeks. Baseline data such as age, sex, body mass index, cause of end-stage kidney disease, systolic blood pressure, duration of dialysis treatment, single pool Kt/Vurea and serum levels of urea nitrogen, creatinine, albumin, blood haemoglobin, calcium, phosphorus, intact parathyroid hormone and C-reactive protein at the predialysis session were also measured. This study adhered to the Declaration of Helsinki and was approved by the Central Ethics Committee at Niigata University. It was registered at the University Hospital Medical Information Network Center (UMIN000009618). All participants provided written informed consent.
Measurement of uraemic toxins
Serum samples were frozen at −30 °C immediately after collection from patients and thawed just before the measurement of uraemic toxins, including low- and intermediate-molecular-weight water-soluble molecules and protein-bound solutions. In the case of PBUTs, levels of both the total and free forms of 5 endogenous metabolites such as IS, PCS, PS, IAA and HA were measured by mass spectrometry as described previously5. Urea nitrogen and β2-microglobulin levels were also measured during the study.
Measurement of oxidative stress
Chromatographic analysis of serum albumin in haemodialysis patients was performed as described previously24. High-performance liquid chromatography (HPLC) analysis of 5 μL aliquots of each serum sample was performed using a Shodex Asahipak ES-502N column (Showa Denko Co., Ltd., Tokyo, Japan; column temperature, 35 ± 0.5 °C). The HPLC system was composed of an intelligent pump (L-6200) equipped with a gradient programmer and an F-1050 fluorescence detector (Hitachi Co., Ltd., Tokyo, Japan). Elution was performed using a linear gradient with increasing ethanol concentrations from 0% to 5% for serum in 0.05 mol/L of sodium acetate and 0.40 mol/L of sodium sulfate mixture (pH 4.85) at a flow rate of 1.0 mL/min. From the HPLC profiles of serum albumin, the value of oxidized albumin content was estimated by dividing the area of oxidized albumin by the total area corresponding to albumin. The serum level of 8-isoprostane was measured using an enzyme-linked immunosorbent assay kit (Detroit R&D Inc. Detroit, MI, USA).
Statistical analyses
The sample size was calculated using published results showing 2.11 ± 0.93 mg/dL as the mean value and standard deviation for CKD patients with a high risk of mortality1. To detect an 80% difference, we estimated 15 participants to achieve 90% statistical power with a 2-sided significance level of 5%. Regarding patient characteristics, continuous variables were expressed as medians (interquartile range: IQR). Regarding the uraemic toxin levels, data were expressed as medians (IQR) and the Wilcoxon signed-rank test was used for comparisons between the levels before and those after AST-120 use. The Spearman rank correlation test was used to assess the correlation between the initial serum levels of PBUTs and the reduction ratio. All statistical analyses were performed using JMP7 (SAS Institute; Cary; NC, USA). A two-sided significance level of 5% was considered statistically significant.
Additional Information
How to cite this article: Yamamoto, S. et al. Continuous Reduction of Protein-Bound Uraemic Toxins with Improved Oxidative Stress by Using the Oral Charcoal Adsorbent AST-120 in Haemodialysis Patients. Sci. Rep. 5, 14381; doi: 10.1038/srep14381 (2015).
References
Barreto, F. C. et al. Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin J Am Soc Nephrol 4, 1551–8 (2009).
Bammens, B., Evenepoel, P., Keuleers, H., Verbeke, K. & Vanrenterghem, Y. Free serum concentrations of the protein-bound retention solute p-cresol predict mortality in hemodialysis patients. Kidney Int 69, 1081–7 (2006).
Lekawanvijit, S., Kompa, A. R., Wang, B. H., Kelly, D. J. & Krum, H. Cardiorenal syndrome: the emerging role of protein-bound uremic toxins. Circ Res 111, 1470–83 (2012).
Susantitaphong, P., Siribamrungwong, M. & Jaber, B. L. Convective therapies versus low-flux hemodialysis for chronic kidney failure: a meta-analysis of randomized controlled trials. Nephrol Dial Transplant 28, 2859–74 (2013).
Itoh, Y., Ezawa, A., Kikuchi, K., Tsuruta, Y. & Niwa, T. Protein-bound uremic toxins in hemodialysis patients measured by liquid chromatography/tandem mass spectrometry and their effects on endothelial ROS production. Anal Bioanal Chem 403, 1841–50 (2012).
Watanabe, H. et al. p-Cresyl sulfate causes renal tubular cell damage by inducing oxidative stress by activation of NADPH oxidase. Kidney Int 83, 582–92 (2013).
Muteliefu, G. et al. Indoxyl sulfate promotes vascular smooth muscle cell senescence with upregulation of p53, p21 and prelamin A through oxidative stress. Am J Physiol Cell Physiol 303, C126–34 (2012).
Schulman, G. et al. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am J Kidney Dis 47, 565–77 (2006).
Dou, L. et al. The cardiovascular effect of the uremic solute indole-3 acetic acid. J Am Soc Nephrol 26, 876–87 (2015).
Tumur, Z., Shimizu, H., Enomoto, A., Miyazaki, H. & Niwa, T. Indoxyl sulfate upregulates expression of ICAM-1 and MCP-1 by oxidative stress-induced NF-kappaB activation. Am J Nephrol 31, 435–41 (2010).
Lekawanvijit, S. et al. Does indoxyl sulfate, a uraemic toxin, have direct effects on cardiac fibroblasts and myocytes? Eur Heart J 31, 1771–9 (2010).
Eknoyan, G. et al. Effect of dialysis dose and membrane flux in maintenance hemodialysis. N Engl J Med 347, 2010–9 (2002).
Schulman, G. et al. Randomized Placebo-Controlled EPPIC Trials of AST-120 in CKD. J Am Soc Nephrol 26, 1732–46 (2015).
Niwa, T. Phenol and p-cresol accumulated in uremic serum measured by HPLC with fluorescence detection. Clin Chem 39, 108–11 (1993).
Schepers, E., Glorieux, G. & Vanholder, R. The gut: the forgotten organ in uremia? Blood Purif 29, 130–6 (2010).
Niwa, T., Ise, M. & Miyazaki, T. Progression of glomerular sclerosis in experimental uremic rats by administration of indole, a precursor of indoxyl sulfate. Am J Nephrol 14, 207–12 (1994).
Sirich, T. L., Plummer, N. S., Gardner, C. D., Hostetter, T. H. & Meyer, T. W. Effect of increasing dietary fiber on plasma levels of colon-derived solutes in hemodialysis patients. Clin J Am Soc Nephrol 9, 1603–10 (2014).
Aronov, P. A. et al. Colonic contribution to uremic solutes. J Am Soc Nephrol 22, 1769–76 (2011).
Lee, C. T. et al. Effects of AST-120 on blood concentrations of protein-bound uremic toxins and biomarkers of cardiovascular risk in chronic dialysis patients. Blood Purif 37, 76–83 (2014).
Fujii, H. et al. Oral charcoal adsorbent (AST-120) prevents progression of cardiac damage in chronic kidney disease through suppression of oxidative stress. Nephrol Dial Transplant 24, 2089–95 (2009).
Yamamoto, S. et al. Oral activated charcoal adsorbent (AST-120) ameliorates extent and instability of atherosclerosis accelerated by kidney disease in apolipoprotein E-deficient mice. Nephrol Dial Transplant 26, 2491–7 (2011).
Yu, M., Kim, Y. J. & Kang, D. H. Indoxyl sulfate-induced endothelial dysfunction in patients with chronic kidney disease via an induction of oxidative stress. Clin J Am Soc Nephrol 6, 30–9 (2011).
Akizawa, T. et al. Effect of a carbonaceous oral adsorbent on the progression of CKD: a multicenter, randomized, controlled trial. Am J Kidney Dis 54, 459–67 (2009).
Anraku, M. et al. Intravenous iron administration induces oxidation of serum albumin in hemodialysis patients. Kidney Int 66, 841–8 (2004).
Acknowledgements
This study was supported in part by a grant-in-aid (no. 24790837) (to S.Y.) from the Japan Society for the Promotion of Science, a grant (to S.Y.) from the Takeda Science Foundation and a grant (to S.Y.) from the SENSHIN Medical Research Foundation.
Author information
Authors and Affiliations
Contributions
Conception, study design, analysis and data interpretation: S.Y., Y.T., K.K., J.K. and I.N. Sample collection and measurement of protein-bound uraemic toxins and other markers: S.Y., K.O., K.M., T.M., H.M. and T.M. Manuscript drafting: S.Y., J.K. and I.N.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Yamamoto, S., Kazama, J., Omori, K. et al. Continuous Reduction of Protein-Bound Uraemic Toxins with Improved Oxidative Stress by Using the Oral Charcoal Adsorbent AST-120 in Haemodialysis Patients. Sci Rep 5, 14381 (2015). https://doi.org/10.1038/srep14381
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep14381
This article is cited by
-
Research on the relationship between serum indoxyl sulfate concentration and iron dynamics index in patients with end-stage kidney disease: a cross-sectional study
Renal Replacement Therapy (2022)
-
In Vitro Detoxification Studies of p-Cresol by Intestinal Bacteria Isolated from Human Feces
Current Microbiology (2020)
-
The uremic toxin p-cresyl sulfate induces proliferation and migration of clear cell renal cell carcinoma via microRNA-21/ HIF-1α axis signals
Scientific Reports (2019)
-
Molecular mechanisms underlying uremic toxin-related systemic disorders in chronic kidney disease: focused on β2-microglobulin-related amyloidosis and indoxyl sulfate-induced atherosclerosis—Oshima Award Address 2016
Clinical and Experimental Nephrology (2019)
-
Gut microbiome-derived phenyl sulfate contributes to albuminuria in diabetic kidney disease
Nature Communications (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
