
Abstract
The Medication Adherence Rating Scale (MARS) is one of the most widely used measurements of adherence in schizophrenia (SZ), but there is no available data regarding its psychometric properties in homeless SZ patients (HSZ). The aim of this study was therefore to assess the psychometric properties of the MARS in a large multicenter sample of HSZ subjects. This multi-centre prospective study was conducted in the following 4 French cities: Lille, Marseille, Paris and Toulouse. Three hundred and fifty-three patients were included. The 3-factor structure of the MARS was confirmed using confirmatory factor analysis: RMSEA = 0.045, CFI = 0.98, TLI = 0.97 and WRMR = 0.76. The unidimensionality of each factor was supported by the satisfactory INFIT statistics. Item internal consistencies were all higher than 0.20 and the Kuder–Richardson were higher than to 0.6, except for factor 2, which was closed to 0.5. Significant associations with symptoms, functioning and quality of life showed satisfactory external validity. The acceptability was satisfactory with missing data lower than 5% for each dimension. The MARS is a short self-administered instrument with acceptable psychometric properties in homeless SZ patients that yields interesting information about medication adherence.
Similar content being viewed by others

Introduction
Medication non-adherence has often been estimated at barely greater than 50% in patients with schizophrenia (SZ)1,2,3, leading to higher rates of relapse and hospitalization as well as to decreasing cognitive and functional prognosis4,5,6. Medication non-adherence is particularly pregnant in SZ marginalized populations, such as homeless individuals, who may face substantial barriers to medication adherence7. The definition of homelessness varies and may include individuals who lack a fixed, regular, and adequate nighttime residence8. Folsom and Jeste summarized studies about schizophrenia in the homeless from 1966 to 2001 and found a prevalence range of schizophrenia from 1% to 45%8. SZ has been shown to be the psychiatric disorder with the highest risk for homelessness9. The assessment of medication non-adherence in homeless SZ (HSZ) patients is thus an important challenge for clinicians, especially to propose targeted interventions to improve it. HSZ subjects may differ from SZ subjects as they have more comorbid substance use disorders that may impact adherence into treatment10. They also have different family support11. Family support has been shown to be crucial for adherence intro treatment in SZ subjects12. HSZ subjects have more emergency department use, which suggests more severe symptomatology in this population13. Additional research is needed on effective and practical approaches to improving health outcomes for homeless people with serious mental illness14. Evaluating adherence into treatment in HSZ is therefore a urgent need and has been rarely explored in the past15,16.
Three strategies have been suggested to reliably assess adherence in non-homeless SZ patients, of which none can be considered to date as a “gold standard”17,18. First, direct measure like electronic pillbox monitoring devices provides an objective measure of medication manipulation by the patient, but this strategy cannot confirm drug intake. Moreover it is expensive and therefore its use is limited in current practice. Second, plasma levels are more direct measures of medication absorption but assessing plasma levels remains costly and its interest in current practice is limited by pharmacokinetic discrepancies between subjects and by a phenomenon known as “white-coat adherence”, in which patients improve their medication-taking behavior in the 5 days before and after an appointment with the health care provider19. The last method based on self-report questionnaires are generally considered as the most cost-effective and time-efficient way to assess medication adherence, although it has also been reported to sometimes overestimate adherence17. This last option appears as the quickest and the most cost-effective mean to assess medication non-adherence in HSZ subjects.
The Medication Adherence Rating Scale (MARS) is one of the most widely used measurements of adherence in SZ patients20. This is a 10-item self-reported questionnaire resulting from the combination of the Medication Adherence Questionnaire21 and the Drug Attitude Inventory22, that were validated in patients with psychosis. Although initial results suggested that the scale had good reliability and validity, its psychometric properties were examined in a sample of moderate size (n = 66) and included patients with both bipolar disorder and SZ. More recently, Fialko et al.23, explored the MARS psychometric properties in a larger sample of 277 patients with SZ, schizoaffective disorder or delusional disorder. They replicated the three factors reported by previous research but also found the internal consistency of the MARS to be lower than original observations.
The aim of this study was therefore to investigate (i) construct validity and reliability, (ii) external validity and (iii) acceptability of the MARS in a large multicenter sample of HSZ subjects.
Methodology
Recruitment and population
The French Housing First program is a multi-centre prospective study was conducted in the following 4 French large cities: Lille, Marseille, Paris and Toulouse24. The inclusion criteria were as follows: age over 18 years; absolutely homeless (i.e., no fixed place to stay for at least the past 7 nights with little likelihood of finding a place in the upcoming month) or precariously housed (housed in single room occupancy, rooming house, or hotel/motel as a primary residence AND in the past year have a history of 2 or more episodes of being Absolutely Homeless OR one episode of being absolutely homeless of at least 4 weeks duration in the past year); diagnosis of SZ by a psychiatrist based on the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV-TR) criteria25; and the ability to speak French. The exclusion criterion was a reduced capacity to consent26. Mobile mental health outreach teams recruited patients over a 12-month period27. Evaluations were performed during face-to-face interviews by psychiatrists and research assistant in the offices of the mobile mental health outreach teams, which were located in the downtown area of each city. The patient completed the MARS questionnaire and other self-reported questionnaires independently or asked for assistance to complete all or part of the questionnaires. Only data at baseline (t0) were used in the MARS validation study.
Data collection
-
1
Medication adherence was assessed using the French translation of the MARS28. This translation followed an internationally accepted methodology into 3 steps: forward translation, backward translation, and patients’ cognitive debriefing29. The MARS contains 10 yes/no item and the sum of items yields a final score ranking from 0 (poor adherence to treatment) to 10 (good adherence to treatment).
-
2
Socio-demographic information: gender, age, marital status and academic level.
-
3
Clinical characteristics: Mental Health was assessed using the Modified Colorado Symptom Index (MCSI) which has been validated in homeless individuals30. The MCSI contains 14 items that ask about how often in the past month an individual has experienced a variety of mental health symptoms, including loneliness, depression, anxiety, and paranoid delusion. An index score for this scale is calculated by summing each response. Higher scores indicate a higher likelihood of mental health problems. Functioning was assessed using the Multnomah Community Ability Scale (MCAS) which scores 17 axes of functionality independently, rated on 5-point Likert scale31,32. In this study, we used 2 axes: 8 – Acceptance of Illness (How well does the client accept (as opposed to deny) his/her psychiatric disability?) and 14 – Medication Compliance (How frequently does the client comply with his/her prescribed medication regimen?).
-
4
QoL was assessed using the SQoL18 which is a self-administered questionnaire developed and validated for the specific assessment of quality of life in patients with SCZ33,34,35. The S-QoL has 18 items and has been validated in homeless individuals with SCZ36 and in several languages34,37,38. Scores range from 0, indicating the lowest QoL, to 100, indicating the highest QoL.
-
5
Drug information: antipsychotic medication (first generation antipsychotic - FGA vs. second generation antipsychotic – SGA) and the number of psychotic treatments were reported.
Statistical analyses
Statistical analyses were performed to explore construct validity, reliability and external validity of the MARS. Descriptive statistics of the sample included frequencies and percentages of categorical variables and the means and standard deviations of continuous variables.
The construct validity of the MARS was explored using confirmatory factor analysis. The following indicators were required: the Root Mean Square Error of Approximation (RMSEA) is acceptable if <0.08 and satisfactory if <0.05, the Comparative Fit Index (CFI) and Tucker‐Lewis Index (TLI) are higher than 0.9 and the Weighted Root Mean Square Residual (WRMR) is <1.0. The unidimensionality of each dimension was assessed using a Rasch analysis. The goodness-of-fit statistics (INFIT, ranging between 0.7 and 1.3) ensured that all items of the scale measured the same concept. Item-internal consistency (IIC) was assessed by correlating each item with its scale (corrected for overlap) using point biserial correlation (measure of association between a continuous variable and a binary variable) (correlation of 0.15 to 0.50 recommended for supporting item-internal consistency39,40,41. Item discriminant validity (IDV) was assessed by determining the extent to which items correlate more highly with the dimensions they are hypothesized to represent than with the other ones42. Floor and ceiling effects were reported assessing the homogeneous repartition of the response distribution.
For each dimension scale, reliability was assessed using Kuder–Richardson Formula-20 (an equivalent of Cronbach’s alpha coefficient for binary data) (a coefficient of at least 0.7 was expected for each scale39).
To explore external validity, Pearson’s correlation coefficients were used to investigate relationships between dimensions of the MARS and age, MCSI, MCAS, SQoL18 and number of treatments; dimension scores of the MARS were compared across patient groups (i.e., gender, marital status, academic level, SGA) using Mann-Whitney tests. Four hypotheses were formulated: (i) self-reported adherence (measured by the MARS score) has a weak to moderate correlation with adherence measured by the clinician (measured by the axes 14 of the MCAS) ; (ii) female gender is associated with lower medication adherence; (iii) High psychotic symptomatology (measured by the MCSI), low acceptance of illness (measured by the axe 8 of the MCAS), low QoL and high number of psychotropic treatments are associated with lower medication adherence and (iv) FGA are associated with lower adherence compared to SGA.
The acceptability of the MARS was tested using the percentage of missing values.
Data analyses were performed using the PASW 17.0.2 and MPLUS 7.2 software.
Ethical Approval
The study was carried out in accordance with the relevant guidelines and regulations including the principles of the Declaration of Helsinki, 6th revision43. Informed consent was obtained from all subjects. We received written consent from all the participants of our study. The Local Ethics Committee (Comité de Protection des Personnes Sud-Méditerranée V, France: trial number 11.050) and the French Drug and Device Regulation Agency (trial number 2011-A00668-33) approved this study.
Results
Sample characteristics
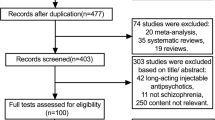
Three hundred and fifty-three homeless SZ patients completed the MARS. The mean age of the sample was 37.8 years (standard deviation = 9.8) and 14.7% of the sample was female (Table 1).
Construct validity and reliability
The three-factor structure of the MARS (factor 1: medication adherence behavior; factor 2: attitude to taking medication score; factor 3: negative side-effects and attitudes to psychotropic medication score) was confirmed by confirmatory factor analysis. All of the indices from the confirmatory model were satisfactory (RMSEA = 0.045, CFI = 0.98, TLI = 0.97 and WRMR = 0.76). The overall scalability was satisfactory. (Table 2) All of the items showed a good fit for the Rasch model in each factor, and none of the items had a statistical INFIT outside the range of acceptability. IIC were all higher than 0.20 and the correlation of each item with its contributive factor was higher than that with the other factors (IIC > IDV), except for factor 2. Floor effects were less than 20% for factors 1 and 2. Ceiling effects were higher than 20% for factors 1 and 3. The Kuder–Richardson coefficient were higher to 0.6, except for factor 2, which was closed to 0.5.
External validity
All of the details are provided in Table 3. External validity can be considered as satisfactory. The MARS total score and the first 2 factors (1 and 2) were moderately correlated with adherence measured by the clinician (axe 14 of the MCAS) (Pearson’s correlation: 0.18–0.25). Significant associations with respectively psychotic symptomatology (MCSI), acceptance of illness (axe 8 of the MCAS), QoL, and with the total number of psychotropic treatments showed satisfactory discriminant validity (all p < 0.05). A statistical trend (p = 0.052) was found in favor of a better adherence with SGA than with FGA (Table 3).
Acceptability
The acceptability was satisfactory with missing data lower than 5% for each dimension.
Discussion
Altogether, our results may be summarized as follows: in a sample of 353 HSZ subjects, the psychometric properties of the MARS were globally satisfactory, except for some indicators that suggest that minor changes could improve its performance. The external validity confirmed the clinical interest of the MARS.
Construct validity and reliability
The present work confirmed the 3-factor structure of the MARS and the unidimensionality of each factor supported by satisfactory INFIT statistics. This scale suggests that adherence to pharmacological treatment is complex and includes the effective behavior toward treatment intake (factor 1), believes toward medication (factor 2) and subjective negative effects of pharmacological treatments (factor 3). IIC values were satisfactory (i.e., higher than 0.2) but factor 2 had IDV values superior to the IIC values. This may be due to some items that are very close between the different factors. For example, the item 5, « I take my medication only when I am sick » included in factor 2, is closed to item 3 “When you feel better, do you sometimes stop taking your medication? » included in factor 1. Item 7 “My thoughts are clearer on medication » (also included in factor 2) is closed to items 9 and 10 « I feel weird, like a ‘zombie’ on medication » « Medication makes me feel tired and sluggish », both included in factor 3 (Table 2).
The Kuder–Richardson coefficient were higher than 0.6, similar to the values produced by Fialko et al.23 and lower to the values produced by Thompson et al. (2000) during the original development of the scale (global alpha = 0.75 and 0.72 in our study)20. However, this finding may not represent a weakness of the reliability of the scale23. Indeed, a low value of alpha could be due to a low number of questions and/or poor inter-relatedness between items44. It is thus likely that the brevity of the MARS is partly responsible for the low value of alpha. Nevertheless, coefficient of 0.6 could be acceptable45. The ceiling and floor effects were higher than 15% for some factors, suggesting that the MARS is probably not optimal to discriminate between subjects at either extreme of the scale. However, this finding is not surprising considering the small number of item and the binary response format.
The construct validity and reliability of the MARS could thus be improved by adding more response options (e.g., Likert scale format) or by adding more items more relevant for homeless individuals, which could also be beneficial for other important properties such as sensitivity to change46. However, these changes should not compromise the quick and simple format of the MARS. Future studies should explore the different options.
External validity
We made 4 hypotheses about external validity. External validity, which was explored by using socio-demographic characteristics and psychiatric and adherence measures, confirmed the majority of our assumptions. Some discrepancies were found, but can be explained by the characteristics of HSZ vs. SZ subjects (e.g., less family support, more substance abuse, lower insight into illness) (Table 3).
First, we hypothesized that self-reported adherence (measured by the MARS score) may have a weak to moderate correlation with key-worker-rated adherence (measured by the MCAS). This difference between key-worker and self-reported adherence is consistent with Fialko et al. findings23 and suggests the need for assessing specifically self-reported adherence in HSZ patients.
Secondly, we hypothesized that female gender would be associated with poor adherence. Indeed, female is a particularly vulnerable group, and initiation of treatment and monitoring are often difficult for them47,48,49. Female are in the minority of the homeless population and they often enter services at a much later stage than male, and when their problems have become more severe and enduring50. In our study, females have lower score for the factor 3, i.e., that females are more sensitive to negative side-effects and have more negative attitudes to psychotropic medication: “I feel weird, like a zombie, on medication”, “Medication makes me feel tired and sluggish”. This result suggests that interventions in female SZ patients should ensure that treatment is effective and that side effects are correctly managed with regular follow-up. Promoting a positive therapeutic alliance and good communication between clinician and patient is probably extremely important to improve individual perceptions or beliefs about the treatments. The side effects are probably not the only problem, and the lack of knowledge about each side effect and lack of skills or management strategies to cope with side effects are probably as much important2,51,52.
Thirdly, we hypothesized that high psychotic symptomatology (measured by the MCSI), low acceptance of disease (measured by the MCAS), low QoL and high number of psychotropic treatments would be associated with lower medication adherence. As expected, high psychotic symptomatology, low acceptance of disease and low QoL was associated with lower medication adherence consistently with previous studies53,54,55. Contrary to our hypothesis, we found that the number of psychotropic treatments was positively correlated with adherence scores. It may be advanced that homeless SZ patients identified by their doctors as more adherent are prescribed more medications23. They may receive a more intensive management because of their better acceptance.
Lastly, we hypothesized that SGA would be associated with a better adherence compared to FGA. Our results seemed confirm this hypothesis (statistical trend). This is consistent with the findings of Dassa et al.54. This result may be explained by a better tolerability of SGA compared to FGA, which may improve the adherence into treatment. However SGA remains a heterogeneous class and further studies should determine which antipsychotics are specifically associated with better adherence compared to others.
Acceptability
Another important finding is the excellent acceptability of the MARS. The rate of missing data was particularly low, especially for homeless patients. Several explanations may be proposed. The MARS is one of the shortest instruments among recent adherence measures for use in schizophrenia23. According to several authors, a short form of the scale is frequently associated with improved acceptability35,56. The average completion time is expected to be around five minutes, which will facilitate its use in research and clinical practice.
Limits and perspectives
An important methodological issue remains in the definition of adherence in schizophrenia, as mentioned in the rationale of the present study. Validity is considered present when the measurement predicts an external criterion based on a gold standard. In the case of adherence, there is no gold standard, so the instrument is considered valid if it consistently fits other construct. Although this choice might be debatable, we undertook comparisons with measurements of key-worker rated adherence and clinical variables well known to be associated with adherence, like acceptance of illness. The clinical significance of this study should be cautiously interpreted in accordance with this choice.
Even with the large overall sample size of this multi-centre study, the sample may not have been representative of the homeless population with schizophrenia. Because our study took place in large cities, our findings may not generalize to homeless people living in smaller cities in which life conditions and needs may be different. However, our study included southern and northern cities, thus taking into consideration socio-economic, cultural and climatic differences.
The present study is a cross-sectional study and longitudinal studies are needed to determine the predictive performance of this measure, reproducibility of these results and the sensibility to change. This last property is of major interest for the follow-up of patients in clinical practice and for psycho-educational program researches.
Conclusion
Altogether, these results suggest that the MARS is a relevant tool to quickly assess self-reported adherence, believes toward medication and subjective negative side effects of pharmacological treatment in HSZ patients in daily practice. This scale has been well accepted and opens to a discussion between the patient and the clinician about pharmacological treatment. However, future works are necessary to improve some characteristics of this scale.
Additional Information
How to cite this article: Zemmour, K. et al. Validation of the Medication Adherence Rating Scale in homeless patients with schizophrenia. Results from the French Housing First experience. Sci. Rep. 6, 31598; doi: 10.1038/srep31598 (2016).
References
Gilmer, T. P. et al. Adherence to treatment with antipsychotic medication and health care costs among Medicaid beneficiaries with schizophrenia. Am J Psychiatry 161, 692–699, doi: 10.1176/appi.ajp.161.4.692 (2004).
Lacro, J. P., Dunn, L. B., Dolder, C. R., Leckband, S. G. & Jeste, D. V. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry 63, 892–909 (2002).
Velligan, D. I. et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry 70 Suppl 4, 1–46; quiz 47–48 (2009).
Ascher-Svanum, H. et al. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry 67, 453–460 (2006).
Robinson, D. et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 56, 241–247 (1999).
Weiden, P. J., Kozma, C., Grogg, A. & Locklear, J. Partial compliance and risk of rehospitalization among California Medicaid patients with schizophrenia. Psychiatr Serv 55, 886–891, doi: 10.1176/appi.ps.55.8.886 (2004).
Hunter, C. E. et al. Barriers to Prescription Medication Adherence Among Homeless and Vulnerably Housed Adults in Three Canadian Cities. J Prim Care Community Health 6, 154–161, doi: 10.1177/2150131914560610 (2015).
Folsom, D. & Jeste, D. V. Schizophrenia in homeless persons: a systematic review of the literature. Acta Psychiatr Scand 105, 404–413 (2002).
Folsom, D. P. et al. Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. Am J Psychiatry 162, 370–376 (2005).
Maremmani, A. G. et al. Substance Use Among Homeless Individuals With Schizophrenia and Bipolar Disorder. J Nerv Ment Dis, doi: 10.1097/NMD.0000000000000462 (2016).
Chen, J. et al. Comparisons of family environment between homeless and non-homeless individuals with schizophrenia in Xiangtan, Hunan. Shanghai Arch Psychiatry 27, 175–182, doi: 10.11919/j.issn.1002-0829.214162 (2015).
Tarrier, N. Some aspects of family interventions in schizophrenia. I: Adherence to intervention programmes. Br J Psychiatry 159, 475–480, 483–474 (1991).
Cheung, A. et al. Emergency department use and hospitalizations among homeless adults with substance dependence and mental disorders. Addict Sci Clin Pract 10, 17, doi: 10.1186/s13722-015-0038-1 (2015).
Sajatovic, M. et al. Prospective trial of customized adherence enhancement plus long-acting injectable antipsychotic medication in homeless or recently homeless individuals with schizophrenia or schizoaffective disorder. J Clin Psychiatry 74, 1249–1255, doi: 10.4088/JCP.12m08331 (2013).
Coe, A. B. et al. Medication adherence challenges among patients experiencing homelessness in a behavioral health clinic. Res Social Adm Pharm 11, e110–120, doi: 10.1016/j.sapharm.2012.11.004 (2015).
Fazel, S., Geddes, J. R. & Kushel, M. The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 384, 1529–1540, doi: 10.1016/S0140-6736(14)61132-6 (2014).
Velligan, D. I. et al. Defining and assessing adherence to oral antipsychotics: a review of the literature. Schizophr Bull 32, 724–742, doi: 10.1093/schbul/sbj075 (2006).
Kane, J. M., Kishimoto, T. & Correll, C. U. Non-adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry 12, 216–226, doi: 10.1002/wps.20060 (2013).
Osterberg, L. & Blaschke, T. Adherence to medication. N Engl J Med 353, 487–497, doi: 10.1056/NEJMra050100 (2005).
Thompson, K., Kulkarni, J. & Sergejew, A. A. Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophr Res 42, 241–247 (2000).
Morisky, D. E., Green, L. W. & Levine, D. M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 24, 67–74 (1986).
Hogan, T. P., Awad, A. G. & Eastwood, R. A self-report scale predictive of drug compliance in schizophrenics: reliability and discriminative validity. Psychol Med 13, 177–183 (1983).
Fialko, L. et al. A large-scale validation study of the Medication Adherence Rating Scale (MARS). Schizophr Res 100, 53–59, doi: 10.1016/j.schres.2007.10.029 (2008).
Tinland, A. et al. Evaluation of the Housing First program in patients with severe mental disorders in France: study protocol for a randomized controlled trial. Trials 14, 309, doi: 10.1186/1745-6215-14-309 (2013).
A. P. A. DSM-IV. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Text revised. American Psychiatric Association, Washington, DC. (2000).
Jeste, D. V. & Saks, E. Decisional capacity in mental illness and substance use disorders: empirical database and policy implications. Behav Sci Law 24, 607–628, doi: 10.1002/bsl.707 (2006).
Girard, V. et al. The analysis of a mobile mental health outreach team activity: from psychiatric emergencies on the street to practice of hospitalization at home for homeless people. Presse Med 41, e226–237, doi: 10.1016/j.lpm.2011.09.032 (2012).
Misdrahi, D., Verdoux, H., Llorca, P. M. & Bayle, F. J. [Therapeutic adherence and schizophrenia: the interest of the validation of the French translation of Medication Adherence Rating Scale (MARS)]. Encephale 30, 409–410 (2004).
Acquadro, C. et al. Literature review of methods to translate health-related quality of life questionnaires for use in multinational clinical trials. Value Health 11, 509–521, doi: 10.1111/j.1524-4733.2007.00292.x (2008).
Conrad, K. J. et al. Reliability and validity of a modified Colorado Symptom Index in a national homeless sample. Ment Health Serv Res 3, 141–153 (2001).
Barker, S., Barron, N., McFarland, B. H. & Bigelow, D. A. A community ability scale for chronically mentally ill consumers: Part I. Reliability and validity. Community Ment Health J 30, 363–383 (1994).
Barker, S., Barron, N., McFarland, B. H., Bigelow, D. A. & Carnahan, T. A community ability scale for chronically mentally ill consumers: Part II. Applications. Community Ment Health J 30, 459–472 (1994).
Auquier, P. et al. Development and validation of a patient-based health-related quality of life questionnaire in schizophrenia: the S-QoL. Schizophr Res 63, 137–149 (2003).
Boyer, L. et al. The development of the S-QoL 18: a shortened quality of life questionnaire for patients with schizophrenia. Schizophr Res 121, 241–250 (2010).
Baumstarck, K. et al. Self-reported quality of life measure is reliable and valid in adult patients suffering from schizophrenia with executive impairment. Schizophr Res. 2013 Apr 5. doi: j.schres.2013.03.008. (2013).
Auquier, P. et al. Toward meeting the needs of homeless people with schizophrenia: the validity of quality of life measurement. PLos One 8, e79677, doi: 10.1371/journal.pone.0079677 (2013).
Caqueo-Urizar, A., Boyer, L., Boucekine, M. & Auquier, P. Spanish cross-cultural adaptation and psychometric properties of the Schizophrenia Quality of Life short-version questionnaire (SQoL18) in 3 middle-income countries: Bolivia, Chile and Peru. Schizophr Res 159, 136–143, doi: 10.1016/j.schres.2014.08.013 (2014).
Chou, C. Y., Ma, M. C., Yang, T. T. & Chen-Sea, M. J. Psychometric validation of the S-QoL Chinese (Taiwan) version for patients with schizophrenia. Qual Life Res 20, 763–767, doi: 10.1007/s11136-010-9809-z (2011).
Carey, R. G. & Seibert, J. H. A patient survey system to measure quality improvement: questionnaire reliability and validity. Med Care 31, 834–845 (1993).
Briggs, S. R. & Cheek, J. M. The role of factor analysis in the development and evaluation of personality scales. J Pers 54, 106–148 (1986).
Chiang, C. L. Statistical Methods of Analysis. World Scientific. (2003).
Campbell, D. T. & Fiske, D. W. Convergent and discriminant validation by the multitrait-multimethod matrix. Psychol Bull 56, 81–105 (1959).
WMA. World Medical Association: Declaration of Helsinki, 6th Revision. Edinburgh. ( 2008).
Sijtsma, K. On the use, the misuse, and the very limited usefulness of Cronbach’s alpha. Psychometrika 74, 107–120 (2009).
Nunnaly, J. C. & Bernstein, I. C. Psychometric theory. (Mc Graw-Hill, 1994).
Lietz, P. Research into questionnaire design. Int J Mark Res 52, 249–272 (2010).
Auerswald, C. L., Lin, J. S. & Parriott, A. Six-year mortality in a street-recruited cohort of homeless youth in San Francisco, California. PeerJ 4, e1909, doi: 10.7717/peerj.1909 (2016).
Baggett, T. P. et al. Mortality among homeless adults in Boston: shifts in causes of death over a 15-year period. JAMA Intern Med 173, 189–195, doi: 10.1001/jamainternmed.2013.1604 (2013).
Hamilton, A. B., Poza, I., Hines, V. & Washington, D. L. Barriers to Psychosocial Services among Homeless Women Veterans. J Soc Work Pract Addict 12, 52–68, doi: 10.1080/1533256X.2012.647584 (2012).
Lim, Y. W., Andersen, R., Leake, B., Cunningham, W. & Gelberg, L. How accessible is medical care for homeless women? Med Care 40, 510–520 (2002).
Lambert, M. et al. Impact of present and past antipsychotic side effects on attitude toward typical antipsychotic treatment and adherence. Eur Psychiatry 19, 415–422, doi: 10.1016/j.eurpsy.2004.06.031 (2004).
Wong, M. M., Chen, E. Y., Lui, S. S. & Tso, S. Medication adherence and subjective weight perception in patients with first-episode psychotic disorder. Clin Schizophr Relat Psychoses 5, 135–141, doi: 10.3371/CSRP.5.3.3 (2011).
Boyer, L. et al. Neurocognition, insight and medication nonadherence in schizophrenia: a structural equation modeling approach. PLos One 7, e47655, doi: 10.1371/journal.pone.0047655 (2012).
Dassa, D. et al. Factors associated with medication non-adherence in patients suffering from schizophrenia: a cross-sectional study in a universal coverage health-care system. Aust N Z J Psychiatry 44, 921–928, doi: 10.3109/00048674.2010.493503 (2010).
Hayhurst, K. P. et al. Improved quality of life over one year is associated with improved adherence in patients with schizophrenia. Eur Psychiatry 29, 191–196, doi: 10.1016/j.eurpsy.2013.03.002 (2014).
McKenna, S. Measuring quality of life in schizophrenia. Eur Psychiatry, 267s–274s (1997).
Acknowledgements
We would like to thank their help and advice in developing the French Housing First program: Paula Goering, Jean-Pierre Bonin, Cécile Leclerc, Eric Latimer and Sonia Coté. This work was supported by institutional grants from the 2011 Programme Hospitalier de Recherche Clinique National and the French Ministry of Health (Direction Générale de la Santé), as well as grants from Janssen Pharmaceutical Companies and the Fondation de France (PHRC-12-024-0278, Afssaps B110684-50, Comité de Protection des Personnes 2011-A00668-33). The sponsor was represented by Assistance Publique, Hôpitaux de Marseille, France; its role was to control the appropriateness of the ethical and legal considerations (Albisson A., Allenou P., Baumstarck K., Beetlestone E., Billard J., Bourlier E., Colucci J.M., Danel T., Debieve J., Djena A., Dupont J., Estecahandy P., Flahaut D., Fortanier C. Guetière G., Hérédia-Rodier P., Jouet E., Labeyrie E., Lefèbvre M., Legagneux J.M., Loundou A., Olive F., Psarra C., Requier E., Sauze D., Simonnet E., Suderie G., Troisoeufs A., Vandini P.P., Vincent B., and Wulfman R.).
Author information
Authors and Affiliations
Consortia
Contributions
Conception and design: A.T. and V.G. Collaborators French Housing First Study Group and P.A. Study coordination: A.T. and V.G. Collaborators French Housing First Study Group and P.A. Inclusion and clinical data collection: V.G. and A.T. Analysis of data: K.Z., A.T., M.B. and L.B. Interpretation of data: K.Z., A.T., S.L., C.L., G.F. and L.B. Drafting and writing of the manuscript: all the authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Additional information
A comprehensive list of consortium members appears at the end of the paper.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zemmour, K., Tinland, A., Boucekine, M. et al. Validation of the Medication Adherence Rating Scale in homeless patients with schizophrenia: Results from the French Housing First experience. Sci Rep 6, 31598 (2016). https://doi.org/10.1038/srep31598
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep31598
This article is cited by
-
The impact of parent history of severe mental illness on schizophrenia outcomes: results from the real-world FACE-SZ cohort
European Archives of Psychiatry and Clinical Neuroscience (2023)
-
Psychotropic medicine beliefs, side effects and adherence in schizophrenia: a patient–caregiver dyad perspective
International Journal of Clinical Pharmacy (2021)
-
Assertive Community Programs for Patients with Severe Mental Disorders: Are Benefits Sustained After Discharge?
Community Mental Health Journal (2020)
-
Homeless women with schizophrenia reported lower adherence to their medication than men: results from the French Housing First experience
Social Psychiatry and Psychiatric Epidemiology (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
