





Abstract
Aims This prospective multicentre observational study assessed the efficacy of specific therapy based on implantable loop recorder (ILR) diagnostic observations in patients with recurrent suspected neurally mediated syncope (NMS).
Methods and results Patients with three or more clinically severe syncopal episodes in the last 2 years without significant electrocardiographic and cardiac abnormalities were included. Orthostatic hypotension and carotid sinus syncope were excluded. After ILR implantation, patients were followed until the first documented syncope (Phase I). The ILR documentation of this episode determined the subsequent therapy and commenced Phase II follow-up. Among 392 patients, the 1-year recurrence rate of syncope during Phase I was 33%. One hundred and three patients had a documented episode and entered Phase II: 53 patients received specific therapy [47 a pacemaker because of asystole of a median 11.5 s duration and six anti-tachyarrhythmia therapy (catheter ablation: four, implantable defibrillator: one, anti-arrhythmic drug: one)] and the remaining 50 patients did not receive specific therapy. The 1-year recurrence rate in 53 patients assigned to a specific therapy was 10% (burden 0.07±0.2 episodes per patient/year) compared with 41% (burden 0.83±1.57 episodes per patient/year) in the patients without specific therapy (80% relative risk reduction for patients, P=0.002, and 92% for burden, P=0.002). The 1-year recurrence rate in patients with pacemakers was 5% (burden 0.05±0.15 episodes per patient/year). Severe trauma secondary to syncope relapse occurred in 2% and mild trauma in 4% of the patients.
Conclusion A strategy based on early diagnostic ILR application, with therapy delayed until documentation of syncope allows a safe, specific, and effective therapy in patients with NMS.
Introduction
It is generally agreed, in accordance with the current guidelines,1,2 that by relatively straightforward initial evaluation (patient history, physical examination, standard electrocardiogram, and measurement of supine/upright blood pressure), it is possible to risk-stratify patients with syncope. Specifically, this approach can effectively identify patients who are likely to have cardiac syncope and who would benefit from further cardiovascular investigations. Furthermore, based on the initial evaluation, a neurally mediated mechanism can be suspected, irrespective of the results of tilt testing.3–5
Therefore, based only on this initial evaluation, a group of patients with suspected neurally mediated syncope (NMS) can be identified with a high level of certainty and followed both through the implantation of a loop recorder (ILR) and after eventual specific ILR-guided treatment. However, there is no existing evidence of the effectiveness of such an approach.
The present study assessed the effectiveness of a diagnostic and treatment strategy, based on the initial evaluation described above, early ILR implantation, and ILR-based specific therapy after syncope recurrence, in patients with recurrent suspected NMS.
Methods
The International Study on Syncope of Uncertain Etiology 2 (ISSUE 2) was a multicentre, prospective, observational study enrolling consecutive patients who underwent an ILR implantation for suspected NMS. Patients were enrolled at 63 European and American centres; enrolment began in June 2002 and ended in July 2004. The Steering Committee designed the trial. Medtronic Inc. funded the trial and provided a study manager to supervise its conduct. Data were sent by investigators via dedicated internet website to an independent clinical-research organization (RDES SL, Barcelona, Spain) that maintained the database, issued data-clarification forms, and assisted by Medtronic clinical monitors, verified source documents. The sponsor had no access to the database and did not participate in the analysis of the results or subsequent publications. All analysis were performed by a pre-determined End-points Committee with the assistance of a statistician. The study was approved by the institutional review boards and signed informed consent was obtained from each patient at the time of enrolment.
Patients
Eligible patients were at least 30 years of age and had suffered, in the prior 2 years, three or more syncope episodes of suspected NMS which was considered by the attending physician to be a severe clinical presentation (because of high number of episodes that affect patient's quality of life or high risk for physical injury due to unpredictable occurrence) requiring treatment initiation. Patients with induced carotid sinus syncope were excluded.
In accordance with the current guidelines,1,2 a NMS was considered likely when, on the initial evaluation, the following observations were excluded: (i) suspected or definite structural heart disease suggesting a high likelihood of cardiac syncope, i.e. syncope during exercise, overt heart failure, ejection fraction ≤40%, myocardial infarction, hypertrophic cardiomyopathy, dilated cardiomyopathy, significant valvular disease, sinus bradycardia <50 bpm or sino-atrial block, Mobitz I second degree atrioventricular block, Mobitz II second or third degree atrioventricular block, bundle branch block, rapid paroxysmal supraventricular tachycardia or ventricular tachycardia, pre-excited QRS complexes, prolonged QT interval, right bundle branch block pattern with ST-elevation in leads V1–V3 (Brugada syndrome), negative T-waves in right precordial leads, epsilon waves, and ventricular late potentials suggestive of arrhythmogenic right ventricular dysplasia; (ii) symptomatic orthostatic hypotension diagnosed by standing blood pressure measurement; (iii) non-syncopal loss of consciousness (e.g. epilepsy, psychiatric, metabolic, drop-attack, cerebral transient ischaemic attack, intoxication, cataplexy); and (iv) subclavian steal syndrome.
Carotid sinus massage of 10 s duration was performed in all patients, supine and upright, and those with suspected carotid sinus syncope were excluded. Tilt testing and adenosine triphosphate (ATP) test were recommended during the screening phase but were not mandatory for inclusion of the patients in the study group. A positive response to tilt testing was defined as the induction of syncope in the presence of bradycardia, hypotension, or both. A positive response to ATP test was defined as the induction of a complete AV block (or sinus pause) with a ventricular pause ≥6.0 s.1,2
Study protocol
Eligible patients were enrolled in the study if they underwent ILR implantation (Reveal Plus, Medtronic Inc., Minneapolis, MN, USA). The recommended programmed mode was one manual event and 13 automatic events for a total duration of 42 min of storage. Patients were instructed to activate the device after every episode of syncope. A screening log of eligible not-implanted patients was also collected. After ILR implantation, Phase I comprised quarterly follow-up visits until the first electrocardiographically (ECG) documented syncope or for a maximum of 24 months (Phase I). The ILR documentation of this episode determined the subsequent therapy and commenced Phase II follow-up. The mechanism of syncope was assigned according to the ISSUE classification by the End-points Committee members, each of whom analysed the records of all episodes.6 The recommended therapies were dual-chamber cardiac pacing in asystolic (type 1) and bradycardic (type 2) patients, anti-arrhythmic therapy in tachyarrhythmic patients (type 4B–D), and counselling and non-specific therapy in patients with normal or slight rhythm variations (type 3) or progressive sinus tachycardia (type 4A). Phase II consisted of quarterly follow-up visits for a maximum of 24 months or until the date of study end (June 2005). A second ILR was implanted in the case of battery depletion before the end of the study; ILR was not explanted during Phase II in patients who did not receive therapy. The study protocol has been previously published.7
Outcome measures
During Phase I, the time of the first ECG documented syncopal recurrence after ILR implantation and the time of the first documented or undocumented syncopal event were collected. During Phase II, the time of the first syncopal recurrence and the total burden of syncopes after application of ILR-guided therapy were collected. Only ECG-documented syncopal episodes were used to determine the treatment strategy and hereby move patients into Phase II. ECG-documented pre-syncope and asymptomatic recordings and syncope events that were undocumented were not considered as endpoints. The patients who received a treatment for these latter episodes were not included in Phase II.
Statistical methods
In the ISSUE-1 study,3 syncope was documented in 29% of patients and half of these received an ILR-based specific therapy. We estimated that the overall effect of any therapy as a consequence of ILR-documented diagnosis would reduce 50% of the recurrences of syncope (from absolute 30% rate during Phase I to 15% rate during Phase II). We therefore estimated that about 400 patients were needed in Phase I to obtain 120 patients with syncope events to be assigned in Phase II of which 60 would be assigned to ILR-based specific therapy and 60 to no specific therapy. The sample size of 120 patients was calculated using a survival estimate for one sample, considering the survival rate of 85% at 1 year, with 95% confidence interval (CI) and 5% precision.
A comparison of the baseline clinical characteristics between the patients who reached the primary endpoint during Phase I and the remaining who did not, as well a comparison between the patients who, during Phase II, received specific therapy and those who did not, was performed in order to evaluate whether there were clinical characteristics able to explain the different outcomes of the patients. Such comparisons between groups were performed with Student's t-test or the non-parametric Mann–Whitney U test for continuous variables and with χ2 or Fisher's exact test for proportions, as appropriate. The time to the first syncope relapse was analysed by means of Kaplan–Meier survival curves, which were compared using the log-rank test.
During Phase II, the time to the first syncope relapse of the patients who were assigned to the different therapies was analysed by means of Kaplan–Meier survival curves and was compared using the log-rank test. The burden of syncope episodes defined as the mean number of episodes per patient/year was also compared in each group. Finally, univariate predictors of syncopal recurrence were evaluated among baseline characteristics. A multivariable Cox regression analysis, which included in the model the block of those variables which showed a P<0.2 at univariate analysis, was used for the evaluation of independent predictors of syncopal recurrence. The assumptions underlying the Cox proportional-hazards model were tested by Shoenfeld residual analysis.
All reported P-values are two-tailed and the value <0.05 was considered significant. SPSS (SPSS Inc., Chicago, IL, USA) software version 12.0.2 statistical package was used for the statistical analyses.
Results
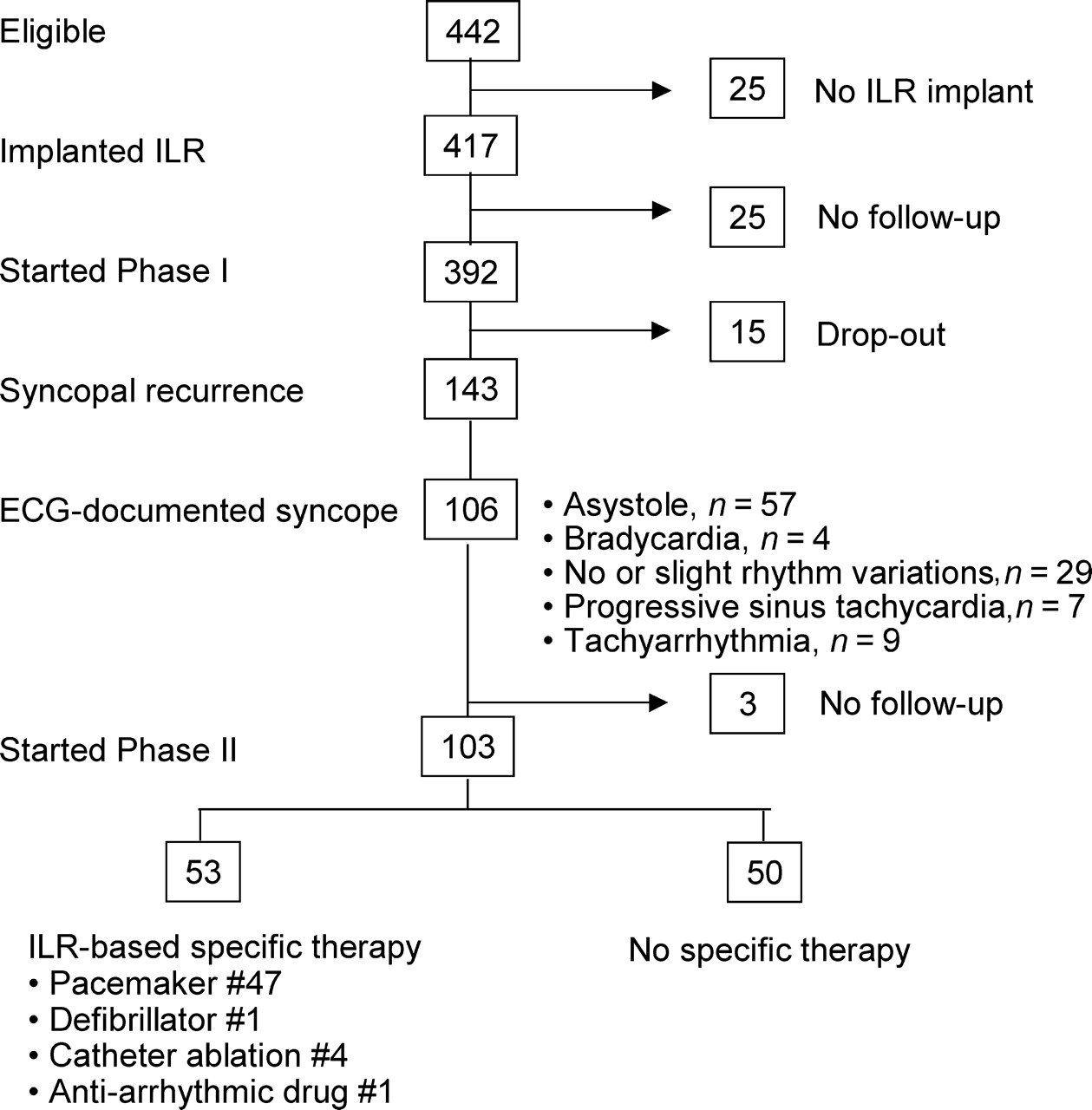
Of 442 eligible patients, 25 (6%) patients did not receive an ILR implant due to patient's refusal or physician's decision to start immediate empirical treatment, and an additional 25 (6%) patients were implanted with an ILR but did not comply with follow-up; thus, 392 received an ILR and started Phase I of the study. The study flow is shown in Figure 1.
Diagram of study design and results.
Phase I: diagnosis
The clinical characteristics of Phase I patients are listed in Table 1.
Characteristics of the patients at enrolment
| Phase I | Phase II | ||||||
|---|---|---|---|---|---|---|---|
| Total population (n=392) | ILR not-documented syncope (n=289) | ILR-documented syncope (n=103) | Pa-value | Specific therapy (n=53) | Non-specific therapy (n=50) | P-value | |
| Mean age, years | 66±14 | 65±14 | 67±14 | 0.379 | 69±13 | 64±15 | 0.068 |
| Male gender, n (%) | 177 (45) | 133 (46) | 44 (43) | 0.563 | 20 (38) | 25 (50) | 0.210 |
| Syncope events | |||||||
| Syncopes, median (interquartile range) | 6 (4–10) | 6 (4–10) | 6 (4–10) | 0.822 | 5 (4–8) | 6 (4–14) | 0.143 |
| Syncopes, last 2 years, median (interquartile range) | 4 (3–5) | 4 (3–5) | 4 (3–6) | 0.084 | 4 (3–5) | 4 (3–7) | 0.206 |
| Interval between first and last episode, median, year (interquartile range) | 7 (4–14) | 7 (4–16) | 6 (4–13) | 0.156 | 6 (4–14) | 6 (4–12) | 0.895 |
| Age at first syncope | 54±20 | 53±20 | 57±19 | 0.062 | 59±18 | 54±19 | 0.237 |
| History of presyncope, n (%) | 212 (54) | 169 (59) | 43 (42) | 0.003 | 20 (38) | 23 (46) | 0.395 |
| Presyncope, median (interquartile range) | 5 (3–10) | 5 (3–10) | 5 (3–11) | 0.963 | 4 (3–10) | 5 (3–27) | 0.275 |
| Hospitalization for syncope, n (%) | 219 (56) | 165 (57) | 54 (52) | 0.393 | 32 (60) | 23 (46) | 0.144 |
| Injuries related to fainting, n (%) | 230 (59) | 164 (57) | 66 (64) | 0.195 | 37 (70) | 30 (60) | 0.297 |
| Major injuries (fractures, brain concussion) | 82 (21) | 61 (21) | 21 (20) | 0.841 | 13 (25) | 8 (16) | 0.283 |
| Minor injuries (bruises, etc.) | 185 (48) | 133 (47) | 52 (51) | 0.488 | 27 (51) | 26 (52) | 0.915 |
| No warning at the onset of the attack (last and/or previous episode), n (%) | 194 (50) | 49 (48) | 145 (51) | 0.608 | 24 (45) | 24 (48) | 0.782 |
| Typical vasovagal/situational presentation (last and/or previous episode), n (%) | 161 (41) | 125 (43) | 36 (35) | 0.135 | 14 (26) | 21 (42) | 0.095 |
| Atypical presentation (uncertain), n (%) | 230 (59) | 163 (57) | 67 (65) | 0.135 | 39 (74) | 29 (58) | 0.095 |
| Tilt testing: performed, n (%) | 343 (88) | 252 (87) | 91 (88) | 0.761 | 41 (77) | 49 (98) | 0.002 |
| Positive of performed | 164 (48) | 126 (50) | 38 (42) | 0.177 | 15 (37) | 22 (45) | 0.425 |
| Cardioinhibitory or mixed of performed | 111 (32) | 87 (35) | 24 (36) | 0.456 | 10 (24) | 11 (29) | 0.607 |
| ATP test: performed, n (%) | 180 (46) | 129 (45) | 51 (50) | 0.394 | 22 (42) | 29 (58) | 0.094 |
| Positive of performed | 55 (29) | 39 (45) | 16 (27) | 0.881 | 8 (36) | 8 (28) | 0.503 |
| Normal electrocardiogram, n (%) | 338 (87) | 249 (87) | 89 (87) | 0.839 | 46 (87) | 45 (90) | 0.638 |
| No structural heart disease, n (%) | 336 (86) | 246 (86) | 90 (88) | 0.524 | 48 (91) | 43 (86) | 0.447 |
| Medical history, n (%) | |||||||
| Cardiac disease | 55 (14) | 41 (14) | 12 (12) | 0.524 | 5 (9) | 7 (14) | 0.447 |
| Hypertension | 178 (46) | 130 (45) | 48 (47) | 0.798 | 24 (45) | 24 (48) | 0.782 |
| Any neurological disease | 35 (9) | 10 (10) | 25 (9) | 0.748 | 4 (8) | 6 (12) | 0.425 |
| Diabetes | 30 (8) | 20 (7) | 10 (10) | 0.366 | 7 (13) | 2 (4) | 0.098 |
| Any therapy at the time of enrolment, n (%) | 152 (39) | 105 (36) | 47 (46) | 0.096 | 20 (38) | 26 (52) | 0.146 |
| Anti-hypertensive | 111 (28) | 78 (27) | 33 (32) | 0.329 | 15 (28) | 17 (34) | 0.532 |
| Psychiatric | 34 (9) | 22 (8) | 12 (12) | 0.211 | 3 (6) | 9 (18) | 0.051 |
| Anti-arrhythmic | 19 (5) | 13 (5) | 6 (6) | 0.590 | 4 (8) | 2 (4) | 0.442 |
| Others | 28 (7) | 19 (7) | 9 (9) | 0.464 | 4 (8) | 4 (8) | 1.000 |
| Phase I | Phase II | ||||||
|---|---|---|---|---|---|---|---|
| Total population (n=392) | ILR not-documented syncope (n=289) | ILR-documented syncope (n=103) | Pa-value | Specific therapy (n=53) | Non-specific therapy (n=50) | P-value | |
| Mean age, years | 66±14 | 65±14 | 67±14 | 0.379 | 69±13 | 64±15 | 0.068 |
| Male gender, n (%) | 177 (45) | 133 (46) | 44 (43) | 0.563 | 20 (38) | 25 (50) | 0.210 |
| Syncope events | |||||||
| Syncopes, median (interquartile range) | 6 (4–10) | 6 (4–10) | 6 (4–10) | 0.822 | 5 (4–8) | 6 (4–14) | 0.143 |
| Syncopes, last 2 years, median (interquartile range) | 4 (3–5) | 4 (3–5) | 4 (3–6) | 0.084 | 4 (3–5) | 4 (3–7) | 0.206 |
| Interval between first and last episode, median, year (interquartile range) | 7 (4–14) | 7 (4–16) | 6 (4–13) | 0.156 | 6 (4–14) | 6 (4–12) | 0.895 |
| Age at first syncope | 54±20 | 53±20 | 57±19 | 0.062 | 59±18 | 54±19 | 0.237 |
| History of presyncope, n (%) | 212 (54) | 169 (59) | 43 (42) | 0.003 | 20 (38) | 23 (46) | 0.395 |
| Presyncope, median (interquartile range) | 5 (3–10) | 5 (3–10) | 5 (3–11) | 0.963 | 4 (3–10) | 5 (3–27) | 0.275 |
| Hospitalization for syncope, n (%) | 219 (56) | 165 (57) | 54 (52) | 0.393 | 32 (60) | 23 (46) | 0.144 |
| Injuries related to fainting, n (%) | 230 (59) | 164 (57) | 66 (64) | 0.195 | 37 (70) | 30 (60) | 0.297 |
| Major injuries (fractures, brain concussion) | 82 (21) | 61 (21) | 21 (20) | 0.841 | 13 (25) | 8 (16) | 0.283 |
| Minor injuries (bruises, etc.) | 185 (48) | 133 (47) | 52 (51) | 0.488 | 27 (51) | 26 (52) | 0.915 |
| No warning at the onset of the attack (last and/or previous episode), n (%) | 194 (50) | 49 (48) | 145 (51) | 0.608 | 24 (45) | 24 (48) | 0.782 |
| Typical vasovagal/situational presentation (last and/or previous episode), n (%) | 161 (41) | 125 (43) | 36 (35) | 0.135 | 14 (26) | 21 (42) | 0.095 |
| Atypical presentation (uncertain), n (%) | 230 (59) | 163 (57) | 67 (65) | 0.135 | 39 (74) | 29 (58) | 0.095 |
| Tilt testing: performed, n (%) | 343 (88) | 252 (87) | 91 (88) | 0.761 | 41 (77) | 49 (98) | 0.002 |
| Positive of performed | 164 (48) | 126 (50) | 38 (42) | 0.177 | 15 (37) | 22 (45) | 0.425 |
| Cardioinhibitory or mixed of performed | 111 (32) | 87 (35) | 24 (36) | 0.456 | 10 (24) | 11 (29) | 0.607 |
| ATP test: performed, n (%) | 180 (46) | 129 (45) | 51 (50) | 0.394 | 22 (42) | 29 (58) | 0.094 |
| Positive of performed | 55 (29) | 39 (45) | 16 (27) | 0.881 | 8 (36) | 8 (28) | 0.503 |
| Normal electrocardiogram, n (%) | 338 (87) | 249 (87) | 89 (87) | 0.839 | 46 (87) | 45 (90) | 0.638 |
| No structural heart disease, n (%) | 336 (86) | 246 (86) | 90 (88) | 0.524 | 48 (91) | 43 (86) | 0.447 |
| Medical history, n (%) | |||||||
| Cardiac disease | 55 (14) | 41 (14) | 12 (12) | 0.524 | 5 (9) | 7 (14) | 0.447 |
| Hypertension | 178 (46) | 130 (45) | 48 (47) | 0.798 | 24 (45) | 24 (48) | 0.782 |
| Any neurological disease | 35 (9) | 10 (10) | 25 (9) | 0.748 | 4 (8) | 6 (12) | 0.425 |
| Diabetes | 30 (8) | 20 (7) | 10 (10) | 0.366 | 7 (13) | 2 (4) | 0.098 |
| Any therapy at the time of enrolment, n (%) | 152 (39) | 105 (36) | 47 (46) | 0.096 | 20 (38) | 26 (52) | 0.146 |
| Anti-hypertensive | 111 (28) | 78 (27) | 33 (32) | 0.329 | 15 (28) | 17 (34) | 0.532 |
| Psychiatric | 34 (9) | 22 (8) | 12 (12) | 0.211 | 3 (6) | 9 (18) | 0.051 |
| Anti-arrhythmic | 19 (5) | 13 (5) | 6 (6) | 0.590 | 4 (8) | 2 (4) | 0.442 |
| Others | 28 (7) | 19 (7) | 9 (9) | 0.464 | 4 (8) | 4 (8) | 1.000 |
Plus–minus values are means±SD.
aP-value was calculated between the 103 Phase II patients and the 289 patients of Phase I who did not undergo Phase II.
Characteristics of the patients at enrolment
| Phase I | Phase II | ||||||
|---|---|---|---|---|---|---|---|
| Total population (n=392) | ILR not-documented syncope (n=289) | ILR-documented syncope (n=103) | Pa-value | Specific therapy (n=53) | Non-specific therapy (n=50) | P-value | |
| Mean age, years | 66±14 | 65±14 | 67±14 | 0.379 | 69±13 | 64±15 | 0.068 |
| Male gender, n (%) | 177 (45) | 133 (46) | 44 (43) | 0.563 | 20 (38) | 25 (50) | 0.210 |
| Syncope events | |||||||
| Syncopes, median (interquartile range) | 6 (4–10) | 6 (4–10) | 6 (4–10) | 0.822 | 5 (4–8) | 6 (4–14) | 0.143 |
| Syncopes, last 2 years, median (interquartile range) | 4 (3–5) | 4 (3–5) | 4 (3–6) | 0.084 | 4 (3–5) | 4 (3–7) | 0.206 |
| Interval between first and last episode, median, year (interquartile range) | 7 (4–14) | 7 (4–16) | 6 (4–13) | 0.156 | 6 (4–14) | 6 (4–12) | 0.895 |
| Age at first syncope | 54±20 | 53±20 | 57±19 | 0.062 | 59±18 | 54±19 | 0.237 |
| History of presyncope, n (%) | 212 (54) | 169 (59) | 43 (42) | 0.003 | 20 (38) | 23 (46) | 0.395 |
| Presyncope, median (interquartile range) | 5 (3–10) | 5 (3–10) | 5 (3–11) | 0.963 | 4 (3–10) | 5 (3–27) | 0.275 |
| Hospitalization for syncope, n (%) | 219 (56) | 165 (57) | 54 (52) | 0.393 | 32 (60) | 23 (46) | 0.144 |
| Injuries related to fainting, n (%) | 230 (59) | 164 (57) | 66 (64) | 0.195 | 37 (70) | 30 (60) | 0.297 |
| Major injuries (fractures, brain concussion) | 82 (21) | 61 (21) | 21 (20) | 0.841 | 13 (25) | 8 (16) | 0.283 |
| Minor injuries (bruises, etc.) | 185 (48) | 133 (47) | 52 (51) | 0.488 | 27 (51) | 26 (52) | 0.915 |
| No warning at the onset of the attack (last and/or previous episode), n (%) | 194 (50) | 49 (48) | 145 (51) | 0.608 | 24 (45) | 24 (48) | 0.782 |
| Typical vasovagal/situational presentation (last and/or previous episode), n (%) | 161 (41) | 125 (43) | 36 (35) | 0.135 | 14 (26) | 21 (42) | 0.095 |
| Atypical presentation (uncertain), n (%) | 230 (59) | 163 (57) | 67 (65) | 0.135 | 39 (74) | 29 (58) | 0.095 |
| Tilt testing: performed, n (%) | 343 (88) | 252 (87) | 91 (88) | 0.761 | 41 (77) | 49 (98) | 0.002 |
| Positive of performed | 164 (48) | 126 (50) | 38 (42) | 0.177 | 15 (37) | 22 (45) | 0.425 |
| Cardioinhibitory or mixed of performed | 111 (32) | 87 (35) | 24 (36) | 0.456 | 10 (24) | 11 (29) | 0.607 |
| ATP test: performed, n (%) | 180 (46) | 129 (45) | 51 (50) | 0.394 | 22 (42) | 29 (58) | 0.094 |
| Positive of performed | 55 (29) | 39 (45) | 16 (27) | 0.881 | 8 (36) | 8 (28) | 0.503 |
| Normal electrocardiogram, n (%) | 338 (87) | 249 (87) | 89 (87) | 0.839 | 46 (87) | 45 (90) | 0.638 |
| No structural heart disease, n (%) | 336 (86) | 246 (86) | 90 (88) | 0.524 | 48 (91) | 43 (86) | 0.447 |
| Medical history, n (%) | |||||||
| Cardiac disease | 55 (14) | 41 (14) | 12 (12) | 0.524 | 5 (9) | 7 (14) | 0.447 |
| Hypertension | 178 (46) | 130 (45) | 48 (47) | 0.798 | 24 (45) | 24 (48) | 0.782 |
| Any neurological disease | 35 (9) | 10 (10) | 25 (9) | 0.748 | 4 (8) | 6 (12) | 0.425 |
| Diabetes | 30 (8) | 20 (7) | 10 (10) | 0.366 | 7 (13) | 2 (4) | 0.098 |
| Any therapy at the time of enrolment, n (%) | 152 (39) | 105 (36) | 47 (46) | 0.096 | 20 (38) | 26 (52) | 0.146 |
| Anti-hypertensive | 111 (28) | 78 (27) | 33 (32) | 0.329 | 15 (28) | 17 (34) | 0.532 |
| Psychiatric | 34 (9) | 22 (8) | 12 (12) | 0.211 | 3 (6) | 9 (18) | 0.051 |
| Anti-arrhythmic | 19 (5) | 13 (5) | 6 (6) | 0.590 | 4 (8) | 2 (4) | 0.442 |
| Others | 28 (7) | 19 (7) | 9 (9) | 0.464 | 4 (8) | 4 (8) | 1.000 |
| Phase I | Phase II | ||||||
|---|---|---|---|---|---|---|---|
| Total population (n=392) | ILR not-documented syncope (n=289) | ILR-documented syncope (n=103) | Pa-value | Specific therapy (n=53) | Non-specific therapy (n=50) | P-value | |
| Mean age, years | 66±14 | 65±14 | 67±14 | 0.379 | 69±13 | 64±15 | 0.068 |
| Male gender, n (%) | 177 (45) | 133 (46) | 44 (43) | 0.563 | 20 (38) | 25 (50) | 0.210 |
| Syncope events | |||||||
| Syncopes, median (interquartile range) | 6 (4–10) | 6 (4–10) | 6 (4–10) | 0.822 | 5 (4–8) | 6 (4–14) | 0.143 |
| Syncopes, last 2 years, median (interquartile range) | 4 (3–5) | 4 (3–5) | 4 (3–6) | 0.084 | 4 (3–5) | 4 (3–7) | 0.206 |
| Interval between first and last episode, median, year (interquartile range) | 7 (4–14) | 7 (4–16) | 6 (4–13) | 0.156 | 6 (4–14) | 6 (4–12) | 0.895 |
| Age at first syncope | 54±20 | 53±20 | 57±19 | 0.062 | 59±18 | 54±19 | 0.237 |
| History of presyncope, n (%) | 212 (54) | 169 (59) | 43 (42) | 0.003 | 20 (38) | 23 (46) | 0.395 |
| Presyncope, median (interquartile range) | 5 (3–10) | 5 (3–10) | 5 (3–11) | 0.963 | 4 (3–10) | 5 (3–27) | 0.275 |
| Hospitalization for syncope, n (%) | 219 (56) | 165 (57) | 54 (52) | 0.393 | 32 (60) | 23 (46) | 0.144 |
| Injuries related to fainting, n (%) | 230 (59) | 164 (57) | 66 (64) | 0.195 | 37 (70) | 30 (60) | 0.297 |
| Major injuries (fractures, brain concussion) | 82 (21) | 61 (21) | 21 (20) | 0.841 | 13 (25) | 8 (16) | 0.283 |
| Minor injuries (bruises, etc.) | 185 (48) | 133 (47) | 52 (51) | 0.488 | 27 (51) | 26 (52) | 0.915 |
| No warning at the onset of the attack (last and/or previous episode), n (%) | 194 (50) | 49 (48) | 145 (51) | 0.608 | 24 (45) | 24 (48) | 0.782 |
| Typical vasovagal/situational presentation (last and/or previous episode), n (%) | 161 (41) | 125 (43) | 36 (35) | 0.135 | 14 (26) | 21 (42) | 0.095 |
| Atypical presentation (uncertain), n (%) | 230 (59) | 163 (57) | 67 (65) | 0.135 | 39 (74) | 29 (58) | 0.095 |
| Tilt testing: performed, n (%) | 343 (88) | 252 (87) | 91 (88) | 0.761 | 41 (77) | 49 (98) | 0.002 |
| Positive of performed | 164 (48) | 126 (50) | 38 (42) | 0.177 | 15 (37) | 22 (45) | 0.425 |
| Cardioinhibitory or mixed of performed | 111 (32) | 87 (35) | 24 (36) | 0.456 | 10 (24) | 11 (29) | 0.607 |
| ATP test: performed, n (%) | 180 (46) | 129 (45) | 51 (50) | 0.394 | 22 (42) | 29 (58) | 0.094 |
| Positive of performed | 55 (29) | 39 (45) | 16 (27) | 0.881 | 8 (36) | 8 (28) | 0.503 |
| Normal electrocardiogram, n (%) | 338 (87) | 249 (87) | 89 (87) | 0.839 | 46 (87) | 45 (90) | 0.638 |
| No structural heart disease, n (%) | 336 (86) | 246 (86) | 90 (88) | 0.524 | 48 (91) | 43 (86) | 0.447 |
| Medical history, n (%) | |||||||
| Cardiac disease | 55 (14) | 41 (14) | 12 (12) | 0.524 | 5 (9) | 7 (14) | 0.447 |
| Hypertension | 178 (46) | 130 (45) | 48 (47) | 0.798 | 24 (45) | 24 (48) | 0.782 |
| Any neurological disease | 35 (9) | 10 (10) | 25 (9) | 0.748 | 4 (8) | 6 (12) | 0.425 |
| Diabetes | 30 (8) | 20 (7) | 10 (10) | 0.366 | 7 (13) | 2 (4) | 0.098 |
| Any therapy at the time of enrolment, n (%) | 152 (39) | 105 (36) | 47 (46) | 0.096 | 20 (38) | 26 (52) | 0.146 |
| Anti-hypertensive | 111 (28) | 78 (27) | 33 (32) | 0.329 | 15 (28) | 17 (34) | 0.532 |
| Psychiatric | 34 (9) | 22 (8) | 12 (12) | 0.211 | 3 (6) | 9 (18) | 0.051 |
| Anti-arrhythmic | 19 (5) | 13 (5) | 6 (6) | 0.590 | 4 (8) | 2 (4) | 0.442 |
| Others | 28 (7) | 19 (7) | 9 (9) | 0.464 | 4 (8) | 4 (8) | 1.000 |
Plus–minus values are means±SD.
aP-value was calculated between the 103 Phase II patients and the 289 patients of Phase I who did not undergo Phase II.
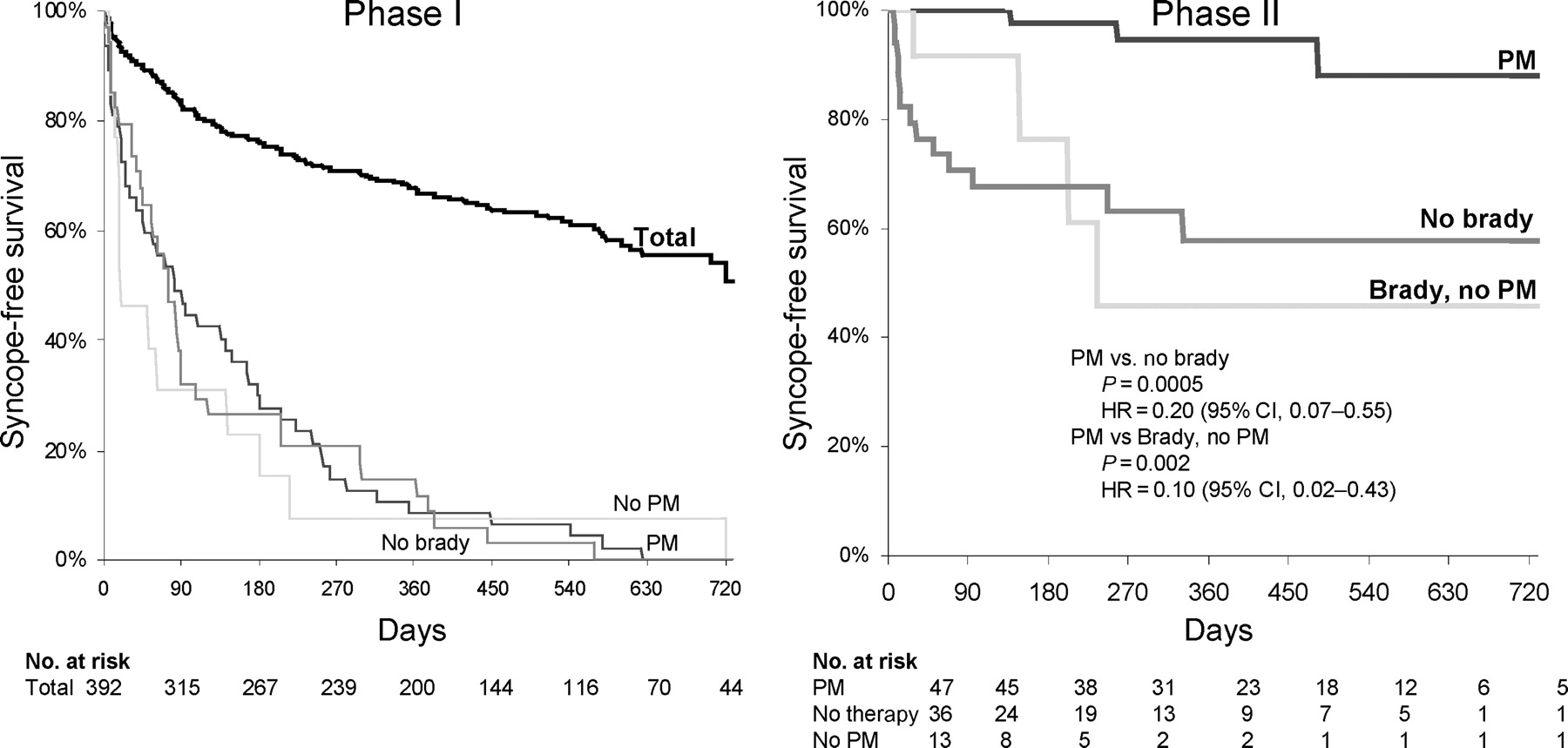
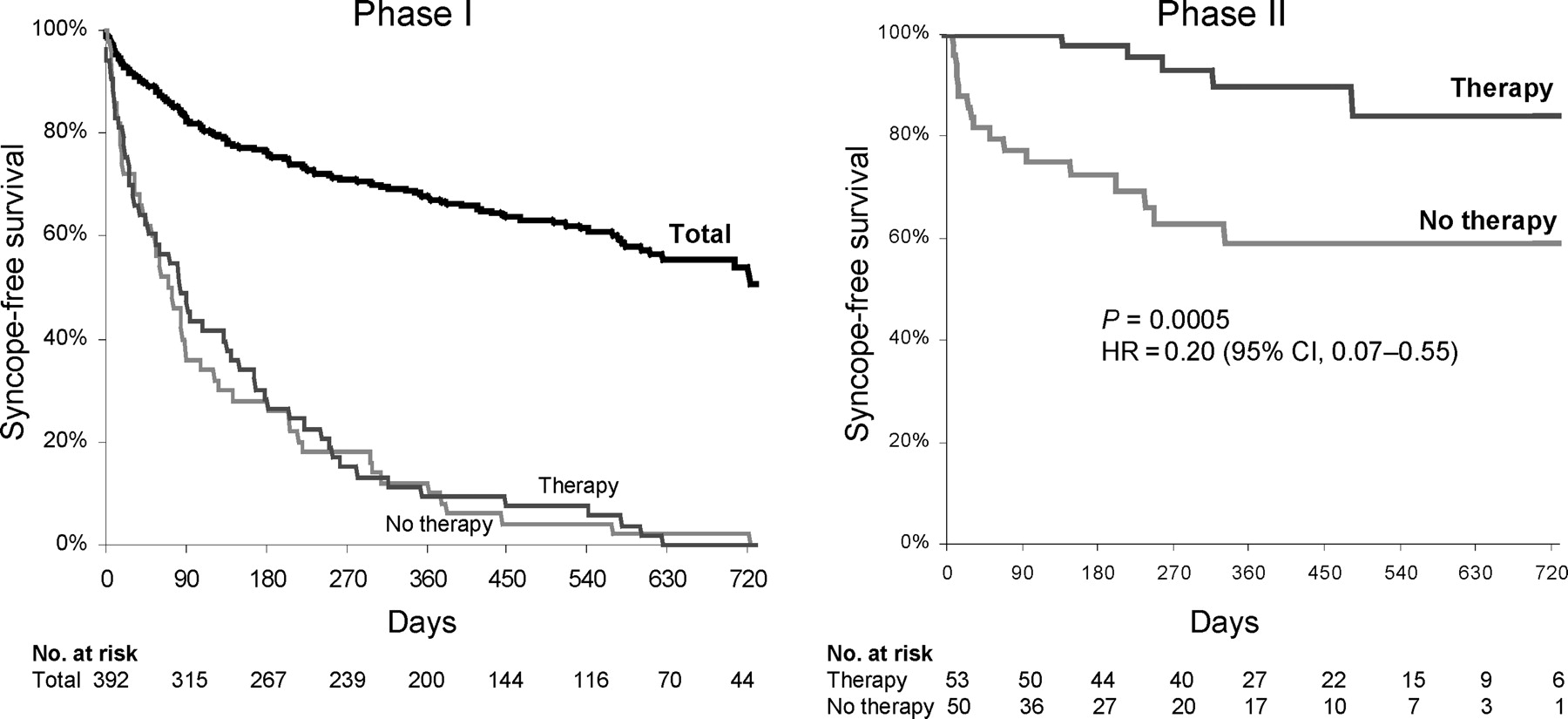
During a median follow-up of 9 months (interquartile range 3–17), 143 patients (36%) had a syncope recurrence with an actuarial recurrence rate of 17, 24, 33, and 49% after 3, 6, 12, and 24 months, respectively (Figure 2) and 88 (22%) patients had pre-syncope(s).
Kaplan–Meier estimates of syncopal recurrence of the total population undergoing ILR implantation (Phase I) and of the two subgroups of patients who received ILR-based specific therapy (therapy) and no specific therapy (no therapy) during Phase II study period after ECG documentation of syncope. These two subgroups had similar actuarial occurrence of syncope during Phase I (P=0.74), which suggests a similar recurrence rate in Phase II if left untreated. The recurrence rate of ILR-based specific therapy group was lower than that of the Phase I population, whereas the recurrence rate of non-specific therapy group was similar or even higher.
Syncope was documented by ILR in 106 (26%) patients after a median of 3 months (interquartile range 1–7). The most frequent finding, which was observed in 57 patients (54%), was one or more prolonged asystolic pauses >3 s, the maximum pause being a median of 11.5 s (interquartile range 6.3–18.5 s) (type 1 of the ISSUE classification5): in 41 of these patients, the asystole was due to sinus arrest and in 16 patients the asystole was due to AV block. Bradycardia was documented in four patients (4%) (type 2). Normal or slight rhythm variations (type 3) and progressive sinus tachycardia (type 4A) were documented in 29 (27%) and seven (7%) patients, respectively. Finally, nine patients (8%) had primary tachyarrhythmias: three paroxysmal atrial fibrillation, five paroxysmal supraventricular tachycardia, and one ventricular tachycardia (type 4B–D).
Fifteen (4%) patients started treatment before syncope relapse after a median of 11 months (interquartile range 3–17 months) due to ILR documentation of asymptomatic or pre-syncopal arrhythmias: cardiac pacing in 11 patients with bradycardia/asystole, catheter ablation in one patient with paroxysmal AV nodal reentrant tachycardia, prophylactic ICD implant in two patients with non-sustained ventricular tachycardia, and empirical drug therapy in one patient. These patients dropped out and were not included in Phase II.
Phase II: therapy
Of the 103 patients who started Phase II follow-up, 53 (51%) patients received ILR-based specific therapy [47 a pacemaker because of asystole of a median 11.5 s duration and six anti-tachyarrhythmia therapy (catheter ablation: four, implantable defibrillator: one, anti-arrhythmic drug; one)] and the remaining 50 (49%) patients did not receive any specific therapy (empirical drugs in seven of these) (Figure 1). This latter group included 13 patients who did not receive pacemaker therapy despite documentation of asystole or bradycardia and one patient who did not receive anti-arrhythmic therapy despite documentation of a primary tachyarrhythmia. The clinical characteristics of the two groups and of the overall population were similar (Table 1).
During a median follow-up of 9 months (interquartile range 4–16), six (11%) patients assigned to ILR-based specific therapy had a total of seven syncope relapses; in comparison, 17 (35%) patients of the non-specific therapy group had a total of 46 syncope relapses. There was a 92% (95% CI 91–98) reduction of total burden in the ILR-based specific therapy group [0.07 (95% CI 0.01–0.12) vs. 0.83 (95% CI 0.38–1.28) episodes per patient/year, P=0.002]. There was also a 80% (95% CI 45–93) relative risk reduction of syncope recurrence with an actuarial recurrence rate of syncope of 0, 2, 10, and 16 vs. 23, 28, 41, and 41% after 3, 6, 12, and 24 months, respectively (P=0.0005) (Figure 2). The recurrence rate of ILR-based specific therapy group was lower than that of the Phase I population (10 vs. 33% at 12 months). On the contrary, the recurrence rate of non-specific therapy group was similar or even higher than that of the Phase I population (41 vs. 33% at 12 months) (Figure 2).
Pre-syncopes occurred in four (8%) patients with ILR-based specific therapy and in eight (16%) patients with non-specific therapy (P=0.227).
Syncope recurred in 4/47 (9%) patients who received a pacemaker (burden 0.05±0.15 episodes per patient/year) with an actuarial 3, 6, 12, and 24 months recurrence rate of 0, 2, 5, and 12%. This rate was significantly lower than that observed in patients without asystole or bradycardia, i.e. type 3 or 4A [87% relative risk reduction (95% CI 55–96), P=0.001 and P=0.001 for burden], and that observed in patients with asystole or bradycardia, i.e. type 1 or 2, who did not receive a pacemaker [recurrence in 4/13 (31%), 90% relative risk reduction (95% CI 57–98), P=0.002] (Figure 3).
The Kaplan–Meier estimates of syncopal recurrence of 47 patients who had documented asystole or bradycardia during Phase I, i.e. type 1 and 2 forms, and were treated with a pacemaker (PM) are compared with that of 36 patients without asystole or bradycardia, i.e. type 3 or 4A, (no brady) and that of 13 patients who had a documented asystole or bradycardia but were not treated with a pacemaker (brady, no PM). These three subgroups had similar actuarial occurrence of syncope during Phase I (PM vs. no brady, P=0.72; PM vs. brady, no PM, P=60), which suggests a similar recurrence rate in Phase II if left untreated. The recurrence rate of PM subgroup was lower than that of the Phase I population, whereas the recurrence rates of the no brady and brady no PM subgroups was similar. HR means Hazard ratio.
At multivariable Cox regression analysis, among eight variables listed in Table 2, pacemaker therapy was the strongest independent predictor of the absence of syncope relapse during Phase II (Table 2).
Univariable and multivariable predictors of syncope recurrence in 103 patients during Phase II
| Univariate | Multivariable | |||
|---|---|---|---|---|
| Hazard ratio (95% CI) | P-value | Hazard ratio (95% CI) | P-value | |
| Mean age, continuous | 0.97 (0.94–0.99) | 0.024 | 0.92 (0.86–1.00) | 0.049 |
| Male gender | 0.96 (0.42–2.20) | 0.928 | ||
| Syncope events | ||||
| Syncopes total, continuous | 1.01 (0.99–1.03) | 0.102 | 1.01 (0.98–1.04) | 0.579 |
| Syncopes last 2 years, continuous | 1.04 (1.01–1.06) | 0.007 | 1.01 (0.97–1.05) | 0.651 |
| Interval between first and last episode, continuous | 0.98 (0.93–1.03) | 0.466 | ||
| Age at first syncope, continuous | 0.99 (0.96–1.01) | 0.174 | 1.06 (0.99–1.14) | 0.098 |
| History of pre-syncope | 0.67 (0.27–1.62) | 0.373 | ||
| Pre-syncope number, continuous | 1.01 (0.98–1.04) | 0.493 | ||
| Hospitalization for syncope | 0.73 (0.32–1.69) | 0.461 | ||
| Injuries related to fainting | 1.12 (0.47–2.66) | 0.798 | ||
| Major injuries (fractures, brain concussion) | 1.36 (0.53–3.48) | 0.519 | ||
| Minor injuries (bruises, etc.) | 1.00 (0.44–2.27) | 0.999 | ||
| No warning at the onset of the attack (last and/or previous episode) | 1.86 (0.79–4.39) | 0.159 | 1.47 (0.58–3.72) | 0.417 |
| Typical vasovagal/situational presentation (last and/or previous episode) | 1.07 (0.45–2.56) | 0.876 | ||
| Atypical presentation (uncertain) | 0.93 (0.39–2.23) | 0.876 | ||
| Tilt testing: performed | 25.1 (0.12–5285) | 0.238 | ||
| Positive | 1.27 (0.55–2.94) | 0.580 | ||
| Cardioinhibitory or mixed | 2.42 (0.51–11.4) | 0.264 | ||
| ATP test: performed | 1.03 (0.45–2.38) | 0.944 | ||
| Positive | 0.74 (0.20–2.81) | 0.662 | ||
| Normal electrocardiogram | 1.26 (0.29–5.43) | 0.754 | ||
| No structural heart disease | 0.73 (0.22–2.49) | 0.617 | ||
| Medical history | ||||
| Cardiac disease | 1.37 (0.40–4.65) | 0.617 | ||
| Hypertension | 0.37 (0.14–0.93) | 0.035 | 0.21 (0.06–0.67) | 0.009 |
| Any neurological disease | 0.04 (0.00–25.4) | 0.334 | ||
| Diabetes | 0.81 (0.19–3.46) | 0.773 | ||
| Any therapy at the time of enrolment | 1.42 (0.63–3.22) | 0.402 | ||
| No ILR-based specific therapya | 4.97 (1.83–13.52) | 0.002 | 3.03 (0.51–17.92) | 0.221 |
| No pacemaker therapy | 7.16 (2.11–24.23) | 0.002 | 26.1 (3.14–217.1) | 0.003 |
| Univariate | Multivariable | |||
|---|---|---|---|---|
| Hazard ratio (95% CI) | P-value | Hazard ratio (95% CI) | P-value | |
| Mean age, continuous | 0.97 (0.94–0.99) | 0.024 | 0.92 (0.86–1.00) | 0.049 |
| Male gender | 0.96 (0.42–2.20) | 0.928 | ||
| Syncope events | ||||
| Syncopes total, continuous | 1.01 (0.99–1.03) | 0.102 | 1.01 (0.98–1.04) | 0.579 |
| Syncopes last 2 years, continuous | 1.04 (1.01–1.06) | 0.007 | 1.01 (0.97–1.05) | 0.651 |
| Interval between first and last episode, continuous | 0.98 (0.93–1.03) | 0.466 | ||
| Age at first syncope, continuous | 0.99 (0.96–1.01) | 0.174 | 1.06 (0.99–1.14) | 0.098 |
| History of pre-syncope | 0.67 (0.27–1.62) | 0.373 | ||
| Pre-syncope number, continuous | 1.01 (0.98–1.04) | 0.493 | ||
| Hospitalization for syncope | 0.73 (0.32–1.69) | 0.461 | ||
| Injuries related to fainting | 1.12 (0.47–2.66) | 0.798 | ||
| Major injuries (fractures, brain concussion) | 1.36 (0.53–3.48) | 0.519 | ||
| Minor injuries (bruises, etc.) | 1.00 (0.44–2.27) | 0.999 | ||
| No warning at the onset of the attack (last and/or previous episode) | 1.86 (0.79–4.39) | 0.159 | 1.47 (0.58–3.72) | 0.417 |
| Typical vasovagal/situational presentation (last and/or previous episode) | 1.07 (0.45–2.56) | 0.876 | ||
| Atypical presentation (uncertain) | 0.93 (0.39–2.23) | 0.876 | ||
| Tilt testing: performed | 25.1 (0.12–5285) | 0.238 | ||
| Positive | 1.27 (0.55–2.94) | 0.580 | ||
| Cardioinhibitory or mixed | 2.42 (0.51–11.4) | 0.264 | ||
| ATP test: performed | 1.03 (0.45–2.38) | 0.944 | ||
| Positive | 0.74 (0.20–2.81) | 0.662 | ||
| Normal electrocardiogram | 1.26 (0.29–5.43) | 0.754 | ||
| No structural heart disease | 0.73 (0.22–2.49) | 0.617 | ||
| Medical history | ||||
| Cardiac disease | 1.37 (0.40–4.65) | 0.617 | ||
| Hypertension | 0.37 (0.14–0.93) | 0.035 | 0.21 (0.06–0.67) | 0.009 |
| Any neurological disease | 0.04 (0.00–25.4) | 0.334 | ||
| Diabetes | 0.81 (0.19–3.46) | 0.773 | ||
| Any therapy at the time of enrolment | 1.42 (0.63–3.22) | 0.402 | ||
| No ILR-based specific therapya | 4.97 (1.83–13.52) | 0.002 | 3.03 (0.51–17.92) | 0.221 |
| No pacemaker therapy | 7.16 (2.11–24.23) | 0.002 | 26.1 (3.14–217.1) | 0.003 |
When not specified, variables are categorized yes vs. no.
aPacemaker therapy was the most frequent therapy in specific therapy group. When no pacemaker therapy was excluded from the model, no ILR-based specific therapy became significant: 5.01 (1.78–14.10), 0.002.
Univariable and multivariable predictors of syncope recurrence in 103 patients during Phase II
| Univariate | Multivariable | |||
|---|---|---|---|---|
| Hazard ratio (95% CI) | P-value | Hazard ratio (95% CI) | P-value | |
| Mean age, continuous | 0.97 (0.94–0.99) | 0.024 | 0.92 (0.86–1.00) | 0.049 |
| Male gender | 0.96 (0.42–2.20) | 0.928 | ||
| Syncope events | ||||
| Syncopes total, continuous | 1.01 (0.99–1.03) | 0.102 | 1.01 (0.98–1.04) | 0.579 |
| Syncopes last 2 years, continuous | 1.04 (1.01–1.06) | 0.007 | 1.01 (0.97–1.05) | 0.651 |
| Interval between first and last episode, continuous | 0.98 (0.93–1.03) | 0.466 | ||
| Age at first syncope, continuous | 0.99 (0.96–1.01) | 0.174 | 1.06 (0.99–1.14) | 0.098 |
| History of pre-syncope | 0.67 (0.27–1.62) | 0.373 | ||
| Pre-syncope number, continuous | 1.01 (0.98–1.04) | 0.493 | ||
| Hospitalization for syncope | 0.73 (0.32–1.69) | 0.461 | ||
| Injuries related to fainting | 1.12 (0.47–2.66) | 0.798 | ||
| Major injuries (fractures, brain concussion) | 1.36 (0.53–3.48) | 0.519 | ||
| Minor injuries (bruises, etc.) | 1.00 (0.44–2.27) | 0.999 | ||
| No warning at the onset of the attack (last and/or previous episode) | 1.86 (0.79–4.39) | 0.159 | 1.47 (0.58–3.72) | 0.417 |
| Typical vasovagal/situational presentation (last and/or previous episode) | 1.07 (0.45–2.56) | 0.876 | ||
| Atypical presentation (uncertain) | 0.93 (0.39–2.23) | 0.876 | ||
| Tilt testing: performed | 25.1 (0.12–5285) | 0.238 | ||
| Positive | 1.27 (0.55–2.94) | 0.580 | ||
| Cardioinhibitory or mixed | 2.42 (0.51–11.4) | 0.264 | ||
| ATP test: performed | 1.03 (0.45–2.38) | 0.944 | ||
| Positive | 0.74 (0.20–2.81) | 0.662 | ||
| Normal electrocardiogram | 1.26 (0.29–5.43) | 0.754 | ||
| No structural heart disease | 0.73 (0.22–2.49) | 0.617 | ||
| Medical history | ||||
| Cardiac disease | 1.37 (0.40–4.65) | 0.617 | ||
| Hypertension | 0.37 (0.14–0.93) | 0.035 | 0.21 (0.06–0.67) | 0.009 |
| Any neurological disease | 0.04 (0.00–25.4) | 0.334 | ||
| Diabetes | 0.81 (0.19–3.46) | 0.773 | ||
| Any therapy at the time of enrolment | 1.42 (0.63–3.22) | 0.402 | ||
| No ILR-based specific therapya | 4.97 (1.83–13.52) | 0.002 | 3.03 (0.51–17.92) | 0.221 |
| No pacemaker therapy | 7.16 (2.11–24.23) | 0.002 | 26.1 (3.14–217.1) | 0.003 |
| Univariate | Multivariable | |||
|---|---|---|---|---|
| Hazard ratio (95% CI) | P-value | Hazard ratio (95% CI) | P-value | |
| Mean age, continuous | 0.97 (0.94–0.99) | 0.024 | 0.92 (0.86–1.00) | 0.049 |
| Male gender | 0.96 (0.42–2.20) | 0.928 | ||
| Syncope events | ||||
| Syncopes total, continuous | 1.01 (0.99–1.03) | 0.102 | 1.01 (0.98–1.04) | 0.579 |
| Syncopes last 2 years, continuous | 1.04 (1.01–1.06) | 0.007 | 1.01 (0.97–1.05) | 0.651 |
| Interval between first and last episode, continuous | 0.98 (0.93–1.03) | 0.466 | ||
| Age at first syncope, continuous | 0.99 (0.96–1.01) | 0.174 | 1.06 (0.99–1.14) | 0.098 |
| History of pre-syncope | 0.67 (0.27–1.62) | 0.373 | ||
| Pre-syncope number, continuous | 1.01 (0.98–1.04) | 0.493 | ||
| Hospitalization for syncope | 0.73 (0.32–1.69) | 0.461 | ||
| Injuries related to fainting | 1.12 (0.47–2.66) | 0.798 | ||
| Major injuries (fractures, brain concussion) | 1.36 (0.53–3.48) | 0.519 | ||
| Minor injuries (bruises, etc.) | 1.00 (0.44–2.27) | 0.999 | ||
| No warning at the onset of the attack (last and/or previous episode) | 1.86 (0.79–4.39) | 0.159 | 1.47 (0.58–3.72) | 0.417 |
| Typical vasovagal/situational presentation (last and/or previous episode) | 1.07 (0.45–2.56) | 0.876 | ||
| Atypical presentation (uncertain) | 0.93 (0.39–2.23) | 0.876 | ||
| Tilt testing: performed | 25.1 (0.12–5285) | 0.238 | ||
| Positive | 1.27 (0.55–2.94) | 0.580 | ||
| Cardioinhibitory or mixed | 2.42 (0.51–11.4) | 0.264 | ||
| ATP test: performed | 1.03 (0.45–2.38) | 0.944 | ||
| Positive | 0.74 (0.20–2.81) | 0.662 | ||
| Normal electrocardiogram | 1.26 (0.29–5.43) | 0.754 | ||
| No structural heart disease | 0.73 (0.22–2.49) | 0.617 | ||
| Medical history | ||||
| Cardiac disease | 1.37 (0.40–4.65) | 0.617 | ||
| Hypertension | 0.37 (0.14–0.93) | 0.035 | 0.21 (0.06–0.67) | 0.009 |
| Any neurological disease | 0.04 (0.00–25.4) | 0.334 | ||
| Diabetes | 0.81 (0.19–3.46) | 0.773 | ||
| Any therapy at the time of enrolment | 1.42 (0.63–3.22) | 0.402 | ||
| No ILR-based specific therapya | 4.97 (1.83–13.52) | 0.002 | 3.03 (0.51–17.92) | 0.221 |
| No pacemaker therapy | 7.16 (2.11–24.23) | 0.002 | 26.1 (3.14–217.1) | 0.003 |
When not specified, variables are categorized yes vs. no.
aPacemaker therapy was the most frequent therapy in specific therapy group. When no pacemaker therapy was excluded from the model, no ILR-based specific therapy became significant: 5.01 (1.78–14.10), 0.002.
Clinical events
During Phase I, seven patients died: two deaths were due to stroke and five were due to non-cardiovascular causes. One patient assigned to non-specific therapy died during sleep in Phase II. Three other patients survived cardiovascular events (stroke, acute myocardial infarction).
Severe trauma secondary to syncope relapse occurred in seven (2%) patients and mild trauma in 16 (4%) patients during Phase I. During Phase II, no patient had trauma. Finally, four patients had ILR pocket infections.
Discussion
This study shows that a strategy based on a relatively straightforward initial clinical evaluation, early application of an ILR, and therapy delayed until ILR-documentation of the apparent basis of syncope is safe and can be used to guide effective therapy in patients with recurrent suspected NMS. Previous studies evaluated the diagnostic value of ILR in patients with unexplained or tilt-induced syncope.3,8–10 This study demonstrates that the use of the ILR can guide effective specific therapy.
In conventional practice, an ECG documentation of syncope being absent, therapy of NMS has been principally empirical or guided by the results of tilt-table testing. Controlled trials of tilt-guided therapy, however, have often failed to show a benefit and the evidence of efficacy for empirical therapy of NMS is weak.1,2,11 Specifically, the efficacy of pacemaker therapy was questioned after two recent controlled trials failed to prove superiority of cardiac pacing over placebo of unselected patients with positive tilt testing.12,13 This is not surprising if we consider that, in this as well as in previous ILR studies,3,8–10 the mechanism of syncope was heterogeneous with bradycardia or asystole accounting only approximately one-half of the syncope events. Although this study showed that pacing is effective when an asystole is documented at the time of syncope, there is no rationale for the use of pacing in patients without documented bradyarrhythmias. In contrast, the observation that a minority of patients had documentation of a primary atrial or ventricular tachyarrhythmia at the time of syncopal relapse, a mechanism that is probably inconsistent with the initial neurally mediated diagnosis, suggests that a primary cardiac aetiology was responsible and that a specific anti-arrhythmic therapy strategy was needed. Thus, the present study demonstrates that improved patient selection methods lead to significantly better therapy outcomes.
Only a minority of the patients ultimately received ILR-based specific therapy; however, these were about one-half of those individuals who had both recurrences and a severe clinical presentation requiring treatment. A high mean age, a history of recurrent syncope beginning in middle or older ages, and frequent injuries probably due to presentation without warning characterized the ISSUE-2 population. These findings also partially differentiated our patient population from the general population of patients affected by NMS and from the population of previous randomized controlled trials.12–15 The natural history of NMS shows that even severely symptomatic patients remain asymptomatic for long periods due to an unpredictable recurrence rate. The 33% recurrence rate at 1 year observed in Phase I and the 41% rate observed in the non-specific therapy group is consistent with that, around 30% per year, observed in most studies that evaluated the natural history of severe recurrent neurally mediated or unexplained syncope.4,16–21
Limitations
Despite the absence of a blinded control group in this study, the beneficial effect of ILR-directed therapy in terms of dramatically reducing the syncope recurrence rate compared with total population of Phase I and with non-specific therapy group is supported by the following observations. First, there is a strong arrhythmic background as shown above. Secondly, the patients who received ILR-based specific therapy had baseline clinical characteristics similar to those of the overall population and of the non-specific therapy group and had a syncopal recurrence rate before treatment (Phase I) similar to that of the non-specific treatment group, thus making the groups comparable (Table 1) (Figure 2). Thirdly, ILR-directed pacemaker therapy was the strongest independent factor that was able to explain the observed reduction of syncopal recurrences (Table 2). Finally, the recurrence rate in the ILR-based specific therapy group in the present study was lower than the 24 and 46% rate observed in the placebo arms of two randomized placebo-controlled drug trials14,15 and the 38 and 40% rate observed in the placebo arms (pacemaker switched off) of two randomized placebo-controlled dual-chamber pacemaker trials12,13; moreover, in this study, the placebo effect of active therapy is hampered by the fact that ILR device itself may have acted as placebo in Phase I and in the non-specific treatment group. However, although some placebo effect is unlikely to have substantially affected the results, the results of the present study need to be confirmed by a formal randomized placebo-controlled study before the ILR strategy becomes completely established.
Conclusion
A strategy based on early application of the ILR with therapy delayed until documentation of syncope allows a safe, specific, and effective therapy for patients with recurrent suspected NMS. Further, based on the findings reported here, it seems reasonable to recommend that early ILR use become standard practice for management (diagnosis and treatment) of patients with severe recurrent suspected NMS.
Acknowledgements
This study was officially endorsed by the European Heart Rhythm Association and supported by a grant from Medtronic Europe.
Conflict of interest: R.S. reports having served as a consultant for Medtronic Inc. during the period of this investigation. D.G.B. reports having served as a consultant for Medtronic Inc., St Jude Medical Inc. and Cardionet Inc. during the period of this investigation.
Appendix
The following persons participated in the ISSUE-2 study.
Steering Committee: M. Brignole (Chair), R. Sutton, C. Menozzi, A. Moya, R. Garcia-Civera, D.G. Benditt, P. Vardas, W. Wieling, D. Andresen, R. Migliorini, D. Hollinworth; End-Points Committee: M. Brignole, C. Menozzi, R. Sutton, A. Moya; Database Electronic Management: RDES SL, Barcelona, Spain; Study Management: M. Brignole, N. Grovale, F. Zanna; Clinical Monitors: N. Grovale (Chair), F. Zanna, M.P. Lopez; S. Mohammad, A. Guthmann, M. Manders, D. Van Aggel, D. Erckens, V. Andersen, E. Sousani, C. Eppacher, J. St Ores; Statistical Analysis: T. De Santo.
Centres and investigators (in order of number of patients recruited)
Italy (total 214 patients): Arcispedale S. Maria Nuova, Reggio Emilia: C. Menozzi, N. Bottoni; Ospedale S. Filippo Neri, Roma: F. Ammirati, M. Santini; Ospedali del Tigullio, Lavagna: M. Brignole, P. Donateo; Ospedale Umberto I, Mestre: A. Raviere, F. Giada; Ospedale S. Camillo De Lellis, Rieti; S. Orazi; Ospedale Civile, Cento: P. Alboni, M. Dinelli; Ospedale San Luca, Milano: G. Perego, R. Brambilla; Ospedale San Pietro Igneo, Fucecchio: A. Del Rosso; Ospedale S. Gerardo dei Tintori, Monza: A. Vincenti, S. De Ceglia; Ospedale Civile, Bentivoglio: B. Sassone; Ospedale di Versilia, Lido di Camaiore: M.T. Baratto; Ospedale Pontenuovo, Firenze; A. Ungar; Ospedale S. Luigi–S. Currò, Catania: M. Gulizia; M. Francese; Ospedale S. Spirito in Sassia, Roma: L. Pandolfo; M. Burattini; Ospedale per gli Infermi, Faenza: D. Cornacchia; Policlinico di Modena, Modena: E. Casali; Ospedale Bolognini, Seriate: P. Giani; Policlinico Seconda Università degli studi, Napoli; L. Santangelo, S. Panico; Ospedale San Antonio e Biagio, Alessandria: G. De Marchi; Ospedale S. Orsola Fatebenefratelli, Brescia: A. Marchetti; Clinica Cardiologica dell'Università di Padova, Padova: G. Buja; F. Folino; Clinica Villa Tiberia, Roma: A. Spampinato; G. Bruni; Ospedale Riguarda, Milano: M. Lunati; Clinica Noto Pasqualino, Palermo: G.Buttera.
Spain (total 109 patients): Hospital Clínico, Valencia: R. García-Civera, S. Morell, R. Ruiz, R. Sanjuan; Hospital General de Albacete, Albacete: J.F. García-Sacristán; Hospital Xeral de Vigo, Vigo: X. Beiras, E. García; Hospital Vall d'Hebrón, Barcelona: A. Moya, C. Alonso; Hospital Virgen de la Arrixaca, Murcia: A. García-Alberola, J. Lacunza; Hospital Clínico San Carlos, Madrid: J. Villacastín, N. Pérez-Castellano; Hospital General de Valencia, Valencia: J. Roda, V. Palanca; Hospital del Mar, Barcelona: J. Martí, J. Delclós; Hospital Virgen de las Nieves, Granada: M. Alvarez, L. Tercedor; Hospital Virgen de la Salud, Toledo: E. Castellanos; Hospital de Santa María, Lleida: J. Tomás-Mauri; Hospital Puerta de Hierro, Madrid: I. Fernández-Lozano, J. Toquero; Hospital de Alarcos, Ciudad Real: J. Bènèzet; Hospital Complejo Hospitalario, León: M.L. Fidalgo; Hospital General de Alicante, Alicante: J.G. Martinez; Hospital Río Hortega, Valladolid: B. Herreros, F. Muñoz.
The Netherlands (total 31 patients): Atrium Medisch Centrum, Heerlen: A.J.J. Aerts; St Antonius Ziekenhuis–Nieuwegein: L.V.A. Boersma; Academisch Medisch Centrum, Amsterdam: W. Wieling; Lucas/Andreas Ziekenhuis, Amsterdam: J.M. Schroeder-Tanka; St Franciscus Gasthuis, Rotterdam: R. Van Mechelen; Medisch Centrum Alkmaar, Alkmaar: J.H. Ruiter.
Germany (total 30 patients): Krankenhaus Am Urban, Berlin: D. Andresen; University Klinikum Hamburg-Eppendorf, Hamburg: T. Meinerts; A. Schuchert; Klinikum Chemnitz, Chemnitz: T. Vieth; Klinikum Großhadern der L-M Universität, München: C. Reithmann; Evangelisches Krankenhaus, Holzminden: P. Von Lowis of Menar.
UK (total 26 patients): Bristol Royal Infirmary, Bristol: T. Cripps; Eastbourne DGH, Eastbourne: N. Sulke; Royal Brompton Hospital, London: R. Sutton; Newcastle General Hospital, University of Newcastle, Newcastle: R.A. Kenny; Glenfield Hospital, Glenfield: J.D. Skehan; St Peter's Hospital, Chertsey: V. Paul; M. Wrigley.
USA (total 14 patients): University of Minnesota, Minneapolis: D.G. Benditt.
Greece (total 13 patients): University Hospital of Crete, Herakleion: P. Vardas; AHEPA, Thesaloniki: G.E. Louridas; V. Vasilikos.
Denmark (total 3 patients): HS Bispebjerg Hospital, København: T.N. Jakobsen; University Hospital, Odense: E.H. Simonsen, J.B. Johansen.
Austria (total 2 patients): Bezirkskrankenhaus Hall, Tirol: W. Grander.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}