




Abstract
Background: The incidence of skin cancer has had a rapid increase in Sweden during the last 20 years. Sun exposure is an important preventable risk factor for skin cancer. It is essential to develop interventions to change people's exposure to the sun. The perception of own susceptibility to harm is essential in theories about self-protective behaviour. The aim of the present paper was to examine the associations between different risk perceptions, sun-related behaviour, readiness to change, and optimism bias. Method: A total of 722 visitors of a mobile skin cancer screening unit answered a questionnaire in the summer of 2001. The campaign was conducted at five different locations in Sweden. Results: The participants in this study seemed to have realistic believes about the contribution of solar radiation to the risk of developing skin cancer, however, they seriously underestimated skin cancer incidence in the population and the impact of skin cancer on general health. Conclusion: People concerned about skin cancer seem to be aware of the fact that sun exposure is an important risk factor for skin cancer, but they fail to use this information in a consistent way to formulate a judgment of their own vulnerability to harm. People need to be informed about the high incidence of skin cancer, the personal risk factors of skin cancer, and the fact that unintentional as well as intentional sun exposure increases the risk of developing skin cancer.
Introduction
Every year ∼30 000 people in Sweden are diagnosed with skin cancer, the majority of which is non-melanoma skin cancer.1 The incidence of skin cancer has had a rapid increase during the last 20 years.1 Even though the steady increase in skin cancer incidence observed worldwide is most likely a result of several factors, one of the major preventable risk factor for skin cancer is the excessive exposure to the ultraviolet rays in sunlight.2–4 In Sweden the increased incidence of skin cancer might be explained by a change in sunbathing habits in the last 50 years, e.g. increased frequency of vacations to sunny resorts. Above all the risk seem to be associated with intense sun exposure leading to erythema, but the overall cumulative sun exposure dose also seem to be important.5 Other known risk factors for skin cancer are light skin pigmentation, blond or red hair colour, green or blue eye colour, atypical nevi, and a number of common moles.4,6
Most of the studies regarding people's attitudes and knowledge about skin cancer has been conducted in countries with much stronger sunlight than Sweden, e.g. Australia and the USA. There are reasons to believe that people's attitudes towards sunbathing and sun-related behaviour differ between countries with many sunshine hours and countries with a few hours of sun for a short period of the year. In Sweden today, it is generally acceptable to sunbathe, without having concern about the possible negative consequences in the future. Few people in Sweden consider themselves to be at risk for developing melanoma and most of the people have a positive attitude towards sunbathing.7
Beliefs about the outcome of behaviour and perception of individual risk with a behaviour may constitute one major component in predicting behavioural intentions, as suggested by some social-cognition models in health psychology, e.g. the Theory of Planned Behaviour,8 and the Health Belief Model.9 People, who believe that intentional tanning is harmless, are most probably less inclined to decrease their sunbathing. Several health psychological factors associated with health promoting behaviour are related to risk perception. Some of these are judgement of individual susceptibility, the seriousness and treatability of a disease, and the effectiveness of preventive actions.10 Judgements of such factors can be affected by a general tendency called unrealistic optimism or optimistic bias.11 Optimism bias means that people have a tendency to judge their own susceptibility for a disease lower than the susceptibility of others. Different explanations to this phenomenon have been presented. According to one of these, optimism bias reduces the anxiety that would be generated by admitting to personal vulnerability. With this theory, the optimistic bias increases when a disease is considered serious. Another hypothesis is that people judge their own susceptibility for diseases lower than the susceptibility of other people to increase self-esteem. Self-esteem is threatened when a danger is not avoided, especially if it is possible to avoid the problem. A third theory describes optimistic bias as a result of cognitive error. Rare diseases, for example, lead to optimistic bias as people do not consider that the same circumstances (that the disease is unusual) are true for everyone. Finally, people tend to make conclusions about the future on earlier experiences, e.g. ‘I haven't had skin cancer therefore I won't get it in the future either’. In a study by Weinstein et al. comparing 32 different health problems, they found a stronger optimistic bias for problems that were considered preventable, unknown, unusual, or embarrassing.11 A British study examined optimistic bias for five health-related problems: skin cancer, deafness, AIDS, and sunstroke among university students.12 They found an overall optimistic bias for all problems and in particular for AIDS. The optimistic bias was not so apparent for skin cancer. It is still unknown how optimistic bias affects behaviour and the intention to change behaviour, but it is reasonable to expect that more optimistic bias will lead to less intention to change behaviour.
Prochaska and DiClemente have constructed a model of behavioural change and readiness to change, which is called the Transtheoretical model (TTM) of behaviour change. The model has been applied to a wide variety of health-related behaviours.13 The authors identify five stages of change: precontemplation (individuals are not intending to change, at least not in the next 6 months), contemplation (individuals are seriously thinking about changing their behaviour in the next 6 months), preparation (individuals are actively preparing to change their behaviour), action (the 6-month-period following a modification of unhealthy behaviour), and maintenance (in this stage people have sustained their new healthy behaviour for more than 6 months). The TTM could be used to design skin cancer preventive campaigns directed towards groups of people at different motivational stages, with different needs for intervention strategies.
The aim of the present paper was to examine the associations between different risk perceptions, sun-related behaviour, readiness to change, and optimism bias.
Methods
Participants
All visitors to a mobile skin-cancer-screening unit during a skin-cancer prevention campaign in the summer of 2001, conducted by the Swedish Cancer Society, were asked to complete a short questionnaire. The campaign was conducted at five different locations in Sweden. Of the 894 visitors, 722 (81%) agreed to complete the questionnaire. Participants <16 years of age were not included in the study. The mean age was 46 years (min = 16, max = 84, SD = 17.0). Out of them 61% were women and 39% were men.
Measures
The questionnaire contained 16 items that measured the frequency of sunbathing, risk perception, judgement of personal ability to protect oneself from developing skin cancer, and readiness to change sunbathing behaviour. The items used in the present paper were as follows:
Background questions. The respondents were asked to indicate their gender and age.
Frequency of sunbathing. The respondents answered two questions on present sunbathing habits: ‘How often do you spend time in the sun during the summer?’ and ‘How often do you sunbathe during the summer with the intention to get a tan?’. The response alternatives were ‘Very often’ [5], ‘Rather often’ [4], ‘Sometimes’ [3], ‘Seldom’ [2], and ‘Never’ [1].
Beliefs about sunbathing. The subjects were asked to indicate, on a continuous scale from 0 to 100, how much percentage of all skin cancer cases they thought was caused by sunbathing.
Risk perception. Three questions were asked to assess the respondent's perception of risk of developing skin cancer. The first question was regarding the personal risk of developing skin cancer with five response alternatives (‘Very high’ [5], ‘Rather high’ [4], ‘Neither high nor low’ [3], ‘Rather low’ [2], and ‘Very low’ [1]). The second question on risk perception concerned the respondent's beliefs about the incidence of skin cancer. They were asked, ‘How many people in Sweden do you think will get a skin cancer diagnosed during a year?’. The response alternatives were ‘<1000’ [1], ‘1000–2000’ [2], ‘2000–5000’ [3], ‘5000–10 000’ [4], ‘10 000–20 000’ [5], and ‘>20 000’ [6]. The third question concerned own risk compared with other's in the same age as oneself. This question was asked to assess the optimistic bias. The response alternatives on this scale were ‘Much lower than for other people’ [2], ‘Somewhat lower than for other people’ [1], ‘The same as for other people’ [0], ‘Somewhat higher than for other people’ [−1], and ‘Much higher than for other people’ [−2].
Beliefs about skin cancer. The respondents reported their thoughts about skin cancer on the following four 5-point scales: seriousness (very dangerous [5]/not dangerous at all [1]), preventability or ability to protect oneself (very high ability to protect oneself [5]/very low ability to protect oneself [1]), treatability (very easy to treat [5]/very difficult to treat [1]), and the number of times the respondents think about skin cancer (very often [5]/never [1]).
Readiness to change. Readiness to change sun-protection behaviour was measured by assessing the stages of change derived from the TTM of behaviour change.13 The participants were asked to mark the statement that applied the best to them. Three different sun-related behaviours were assessed: giving up sunbathing, reducing sun exposure, and protect the skin from the sun. Those who marked ‘I have never thought of reducing exposure to the sun’ were classified as being in the precontemplation stage [1]. Those who marked ‘I could think of reducing exposure to the sun’ were classified as contemplators [2]. Those who marked the statement ‘I intend to start reducing my exposure to the sun’ were classified as being in the preparation stage [3]. Those who marked ‘I have started to reduce my exposure to the sun’ were classified as being in the action stage [4]. Those who marked ‘I have already reduced my exposure to the sun’ were classified as maintainers [5]. Similar statements were indicated for the other two sun-related behaviours. The questions about readiness to change have sufficient reliability, as suggested by according to a previous study.14
Statistical analyses
Sommer's d analyses were used to test age groups, gender, and skin type differences in current sunbathing behaviour, future sunbathing behaviour, sun protection and knowledge, beliefs, and attitudes.15 Correlations between ordinal variables were made using Spearman's Rho calculations.16 The SPSS statistical package was used.17
Ethical considerations
All participants were informed that taking part in the study was voluntary and that they were free to drop out of the study at any time. Participation in the study was not a prerequisite for receiving a skin check-up. The study was approved by the Ethical Committee of the Karolinska Institutet (No. 01-270).
Results
Frequency of sunbathing, beliefs about skin cancer, and risk perception
About 80% of both men and women often or very often spent time in the sun during the summer. Younger people were somewhat more likely to spend time in the sun (table 1). Women were much more likely than men to sunbathe intentionally, as were younger people (see table 1).
Time spent in the sun and frequency of sunbathing assessed by gender and age
| N | Very often/Often (%) | Sometimes (%) | Seldom/Never (%) | Sommer's d | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| How often do you spend time in the sun? | ||||||||||
| Gender | n.s. | |||||||||
| Males | 263 | 77 | 20 | 3 | ||||||
| Females | 410 | 82 | 15 | 3 | ||||||
| Age | n.s. | |||||||||
| <30 | 146 | 80 | 16 | 3 | ||||||
| 30–60 | 377 | 81 | 17 | 2 | ||||||
| >60 | 165 | 74 | 18 | 8 | ||||||
| How often do you sunbathe? | ||||||||||
| Gender | 0.17*** | |||||||||
| Males | 258 | 38 | 41 | 21 | ||||||
| Females | 410 | 56 | 29 | 16 | ||||||
| Age | 0.18*** | |||||||||
| <30 | 144 | 61 | 27 | 12 | ||||||
| 30–60 | 377 | 48 | 37 | 15 | ||||||
| >60 | 161 | 37 | 31 | 32 | ||||||
| N | Very often/Often (%) | Sometimes (%) | Seldom/Never (%) | Sommer's d | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| How often do you spend time in the sun? | ||||||||||
| Gender | n.s. | |||||||||
| Males | 263 | 77 | 20 | 3 | ||||||
| Females | 410 | 82 | 15 | 3 | ||||||
| Age | n.s. | |||||||||
| <30 | 146 | 80 | 16 | 3 | ||||||
| 30–60 | 377 | 81 | 17 | 2 | ||||||
| >60 | 165 | 74 | 18 | 8 | ||||||
| How often do you sunbathe? | ||||||||||
| Gender | 0.17*** | |||||||||
| Males | 258 | 38 | 41 | 21 | ||||||
| Females | 410 | 56 | 29 | 16 | ||||||
| Age | 0.18*** | |||||||||
| <30 | 144 | 61 | 27 | 12 | ||||||
| 30–60 | 377 | 48 | 37 | 15 | ||||||
| >60 | 161 | 37 | 31 | 32 | ||||||
P < 0.0001; **P < 0.001; *P < 0.005
Time spent in the sun and frequency of sunbathing assessed by gender and age
| N | Very often/Often (%) | Sometimes (%) | Seldom/Never (%) | Sommer's d | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| How often do you spend time in the sun? | ||||||||||
| Gender | n.s. | |||||||||
| Males | 263 | 77 | 20 | 3 | ||||||
| Females | 410 | 82 | 15 | 3 | ||||||
| Age | n.s. | |||||||||
| <30 | 146 | 80 | 16 | 3 | ||||||
| 30–60 | 377 | 81 | 17 | 2 | ||||||
| >60 | 165 | 74 | 18 | 8 | ||||||
| How often do you sunbathe? | ||||||||||
| Gender | 0.17*** | |||||||||
| Males | 258 | 38 | 41 | 21 | ||||||
| Females | 410 | 56 | 29 | 16 | ||||||
| Age | 0.18*** | |||||||||
| <30 | 144 | 61 | 27 | 12 | ||||||
| 30–60 | 377 | 48 | 37 | 15 | ||||||
| >60 | 161 | 37 | 31 | 32 | ||||||
| N | Very often/Often (%) | Sometimes (%) | Seldom/Never (%) | Sommer's d | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| How often do you spend time in the sun? | ||||||||||
| Gender | n.s. | |||||||||
| Males | 263 | 77 | 20 | 3 | ||||||
| Females | 410 | 82 | 15 | 3 | ||||||
| Age | n.s. | |||||||||
| <30 | 146 | 80 | 16 | 3 | ||||||
| 30–60 | 377 | 81 | 17 | 2 | ||||||
| >60 | 165 | 74 | 18 | 8 | ||||||
| How often do you sunbathe? | ||||||||||
| Gender | 0.17*** | |||||||||
| Males | 258 | 38 | 41 | 21 | ||||||
| Females | 410 | 56 | 29 | 16 | ||||||
| Age | 0.18*** | |||||||||
| <30 | 144 | 61 | 27 | 12 | ||||||
| 30–60 | 377 | 48 | 37 | 15 | ||||||
| >60 | 161 | 37 | 31 | 32 | ||||||
P < 0.0001; **P < 0.001; *P < 0.005
About 90% of both men and women of all ages underestimated the incidence of skin cancer in the population. Less than 20% thought that they were at a high risk of developing skin cancer. More women than men thought that they were at a high risk of developing skin cancer (table 2). There was no age difference in the perception of risk.
Responses to three questions regarding the risk of developing skin cancer assessed by gender and age
| Annual incidence of skin cancer in Sweden | N | <1000 (%) | 1000–2000 (%) | 2000–5000 (%) | 5000–10 000 (%) | 10 000–20 000 (%) | >20 000 (%) | Sommer's d |
|---|---|---|---|---|---|---|---|---|
| Gender | n.s. | |||||||
| Males | 247 | 3 | 22 | 28 | 22 | 15 | 10 | |
| Females | 390 | 3 | 20 | 29 | 24 | 15 | 9 | |
| Age | n.s. | |||||||
| <30 | 139 | 4 | 26 | 26 | 19 | 16 | 9 | |
| 30–60 | 362 | 3 | 20 | 31 | 23 | 14 | 9 | |
| >60 | 139 | 1 | 19 | 26 | 24 | 19 | 11 |
| Annual incidence of skin cancer in Sweden | N | <1000 (%) | 1000–2000 (%) | 2000–5000 (%) | 5000–10 000 (%) | 10 000–20 000 (%) | >20 000 (%) | Sommer's d |
|---|---|---|---|---|---|---|---|---|
| Gender | n.s. | |||||||
| Males | 247 | 3 | 22 | 28 | 22 | 15 | 10 | |
| Females | 390 | 3 | 20 | 29 | 24 | 15 | 9 | |
| Age | n.s. | |||||||
| <30 | 139 | 4 | 26 | 26 | 19 | 16 | 9 | |
| 30–60 | 362 | 3 | 20 | 31 | 23 | 14 | 9 | |
| >60 | 139 | 1 | 19 | 26 | 24 | 19 | 11 |
| Personal risk of developing skin cancer | N | Very high/Rather high (%) | Neither high nor low (%) | Rather low/Very low (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | 0.18*** | ||||
| Males | 255 | 14 | 65 | 21 | |
| Females | 407 | 22 | 70 | 8 | |
| Age | n.s. | ||||
| <30 | 145 | 20 | 65 | 15 | |
| 30–60 | 375 | 17 | 70 | 13 | |
| >60 | 155 | 21 | 68 | 12 |
| Personal risk of developing skin cancer | N | Very high/Rather high (%) | Neither high nor low (%) | Rather low/Very low (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | 0.18*** | ||||
| Males | 255 | 14 | 65 | 21 | |
| Females | 407 | 22 | 70 | 8 | |
| Age | n.s. | ||||
| <30 | 145 | 20 | 65 | 15 | |
| 30–60 | 375 | 17 | 70 | 13 | |
| >60 | 155 | 21 | 68 | 12 |
| Own risk of skin cancer compared with others | N | Lower than for other people (%) | Same as for other people (%) | Higher than for other people (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | −0.14*** | ||||
| Males | 254 | 18 | 70 | 12 | |
| Females | 408 | 10 | 70 | 20 | |
| Age | n.s. | ||||
| <30 | 143 | 11 | 71 | 18 | |
| 30–60 | 377 | 13 | 69 | 18 | |
| >60 | 154 | 16 | 73 | 12 |
| Own risk of skin cancer compared with others | N | Lower than for other people (%) | Same as for other people (%) | Higher than for other people (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | −0.14*** | ||||
| Males | 254 | 18 | 70 | 12 | |
| Females | 408 | 10 | 70 | 20 | |
| Age | n.s. | ||||
| <30 | 143 | 11 | 71 | 18 | |
| 30–60 | 377 | 13 | 69 | 18 | |
| >60 | 154 | 16 | 73 | 12 |
***P < 0.0001; **P < 0.001; *P < 0.005
Responses to three questions regarding the risk of developing skin cancer assessed by gender and age
| Annual incidence of skin cancer in Sweden | N | <1000 (%) | 1000–2000 (%) | 2000–5000 (%) | 5000–10 000 (%) | 10 000–20 000 (%) | >20 000 (%) | Sommer's d |
|---|---|---|---|---|---|---|---|---|
| Gender | n.s. | |||||||
| Males | 247 | 3 | 22 | 28 | 22 | 15 | 10 | |
| Females | 390 | 3 | 20 | 29 | 24 | 15 | 9 | |
| Age | n.s. | |||||||
| <30 | 139 | 4 | 26 | 26 | 19 | 16 | 9 | |
| 30–60 | 362 | 3 | 20 | 31 | 23 | 14 | 9 | |
| >60 | 139 | 1 | 19 | 26 | 24 | 19 | 11 |
| Annual incidence of skin cancer in Sweden | N | <1000 (%) | 1000–2000 (%) | 2000–5000 (%) | 5000–10 000 (%) | 10 000–20 000 (%) | >20 000 (%) | Sommer's d |
|---|---|---|---|---|---|---|---|---|
| Gender | n.s. | |||||||
| Males | 247 | 3 | 22 | 28 | 22 | 15 | 10 | |
| Females | 390 | 3 | 20 | 29 | 24 | 15 | 9 | |
| Age | n.s. | |||||||
| <30 | 139 | 4 | 26 | 26 | 19 | 16 | 9 | |
| 30–60 | 362 | 3 | 20 | 31 | 23 | 14 | 9 | |
| >60 | 139 | 1 | 19 | 26 | 24 | 19 | 11 |
| Personal risk of developing skin cancer | N | Very high/Rather high (%) | Neither high nor low (%) | Rather low/Very low (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | 0.18*** | ||||
| Males | 255 | 14 | 65 | 21 | |
| Females | 407 | 22 | 70 | 8 | |
| Age | n.s. | ||||
| <30 | 145 | 20 | 65 | 15 | |
| 30–60 | 375 | 17 | 70 | 13 | |
| >60 | 155 | 21 | 68 | 12 |
| Personal risk of developing skin cancer | N | Very high/Rather high (%) | Neither high nor low (%) | Rather low/Very low (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | 0.18*** | ||||
| Males | 255 | 14 | 65 | 21 | |
| Females | 407 | 22 | 70 | 8 | |
| Age | n.s. | ||||
| <30 | 145 | 20 | 65 | 15 | |
| 30–60 | 375 | 17 | 70 | 13 | |
| >60 | 155 | 21 | 68 | 12 |
| Own risk of skin cancer compared with others | N | Lower than for other people (%) | Same as for other people (%) | Higher than for other people (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | −0.14*** | ||||
| Males | 254 | 18 | 70 | 12 | |
| Females | 408 | 10 | 70 | 20 | |
| Age | n.s. | ||||
| <30 | 143 | 11 | 71 | 18 | |
| 30–60 | 377 | 13 | 69 | 18 | |
| >60 | 154 | 16 | 73 | 12 |
| Own risk of skin cancer compared with others | N | Lower than for other people (%) | Same as for other people (%) | Higher than for other people (%) | Sommer's d |
|---|---|---|---|---|---|
| Gender | −0.14*** | ||||
| Males | 254 | 18 | 70 | 12 | |
| Females | 408 | 10 | 70 | 20 | |
| Age | n.s. | ||||
| <30 | 143 | 11 | 71 | 18 | |
| 30–60 | 377 | 13 | 69 | 18 | |
| >60 | 154 | 16 | 73 | 12 |
***P < 0.0001; **P < 0.001; *P < 0.005
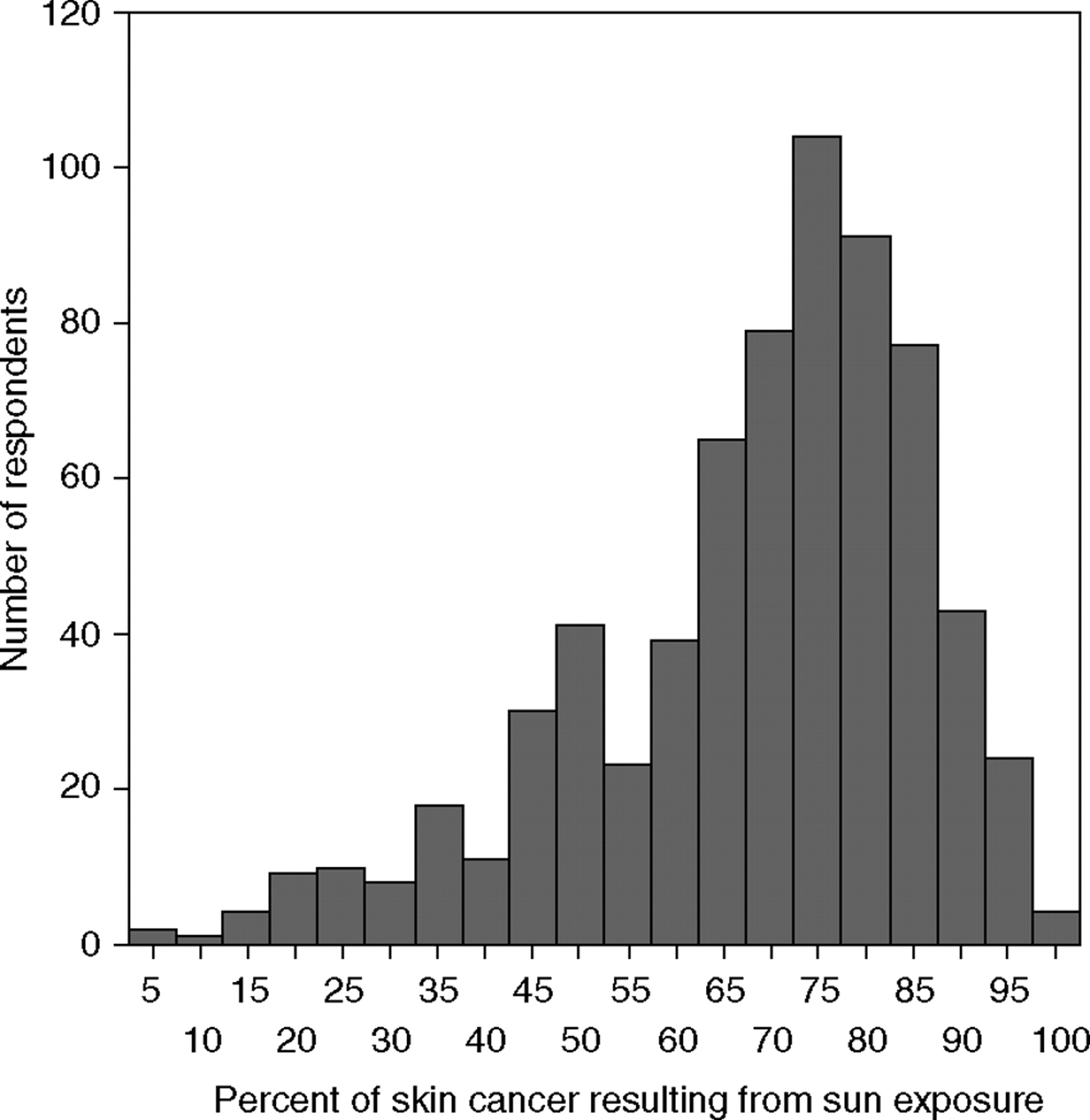
The respondents were asked a question regarding how much percentage of all skin cancer cases that they thought was a consequence of sun exposure. The mean percentage was 68% and the standard deviation was 17.8%, the response frequency is shown in figure 1.
Respondents answer to a question regarding the percentage of skin cancer cases that they thought was a consequence of sun exposure (N = 660)
Optimistic bias
About 17% of the men and 9% of the women thought that they had lower than average risk of developing skin cancer compared with people of their own age (see table 2). Thus, women were less optimistically biased than men. There was no statistical difference in age and optimistic bias.
Readiness to change sun-related behaviours
Most people did not intend to stop sunbathing. Approximately 85% could be attributed to the precontemplation or contemplation stages of change (table 3). Older persons were more inclined to change than younger persons.
Readiness to change sun-related behaviours assessed by gender and age
| Readiness to stop sunbathing | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | n.s. | ||||||||||
| Males | 252 | 42 | 44 | 2 | 6 | 6 | |||||
| Females | 394 | 38 | 47 | 2 | 8 | 5 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 144 | 46 | 47 | 1 | 4 | 1 | |||||
| 30–60 | 370 | 43 | 44 | 1 | 6 | 5 | |||||
| >60 | 146 | 25 | 47 | 4 | 13 | 10 | |||||
| Readiness to stop sunbathing | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | n.s. | ||||||||||
| Males | 252 | 42 | 44 | 2 | 6 | 6 | |||||
| Females | 394 | 38 | 47 | 2 | 8 | 5 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 144 | 46 | 47 | 1 | 4 | 1 | |||||
| 30–60 | 370 | 43 | 44 | 1 | 6 | 5 | |||||
| >60 | 146 | 25 | 47 | 4 | 13 | 10 | |||||
| Readiness to decrease sun exposure | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | −0.13** | ||||||||||
| Males | 255 | 14 | 54 | 6 | 13 | 12 | |||||
| Females | 399 | 11 | 44 | 6 | 28 | 11 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 145 | 14 | 59 | 6 | 15 | 6 | |||||
| 30–60 | 374 | 12 | 47 | 6 | 23 | 11 | |||||
| >60 | 149 | 9 | 37 | 9 | 26 | 19 | |||||
| Readiness to decrease sun exposure | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | −0.13** | ||||||||||
| Males | 255 | 14 | 54 | 6 | 13 | 12 | |||||
| Females | 399 | 11 | 44 | 6 | 28 | 11 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 145 | 14 | 59 | 6 | 15 | 6 | |||||
| 30–60 | 374 | 12 | 47 | 6 | 23 | 11 | |||||
| >60 | 149 | 9 | 37 | 9 | 26 | 19 | |||||
| Readiness to increase sun protective behaviour | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | 0.17*** | ||||||||||
| Males | 252 | 5 | 32 | 4 | 33 | 26 | |||||
| Females | 398 | 2 | 18 | 1 | 39 | 40 | |||||
| Age | −0.22*** | ||||||||||
| <30 | 178 | 1 | 14 | 3 | 36 | 47 | |||||
| 30–60 | 348 | 3 | 23 | 2 | 37 | 35 | |||||
| >60 | 144 | 8 | 32 | 4 | 38 | 19 | |||||
| Readiness to increase sun protective behaviour | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | 0.17*** | ||||||||||
| Males | 252 | 5 | 32 | 4 | 33 | 26 | |||||
| Females | 398 | 2 | 18 | 1 | 39 | 40 | |||||
| Age | −0.22*** | ||||||||||
| <30 | 178 | 1 | 14 | 3 | 36 | 47 | |||||
| 30–60 | 348 | 3 | 23 | 2 | 37 | 35 | |||||
| >60 | 144 | 8 | 32 | 4 | 38 | 19 | |||||
P < 0.001; **P < 0.01; *P < 0.05
Readiness to change sun-related behaviours assessed by gender and age
| Readiness to stop sunbathing | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | n.s. | ||||||||||
| Males | 252 | 42 | 44 | 2 | 6 | 6 | |||||
| Females | 394 | 38 | 47 | 2 | 8 | 5 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 144 | 46 | 47 | 1 | 4 | 1 | |||||
| 30–60 | 370 | 43 | 44 | 1 | 6 | 5 | |||||
| >60 | 146 | 25 | 47 | 4 | 13 | 10 | |||||
| Readiness to stop sunbathing | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | n.s. | ||||||||||
| Males | 252 | 42 | 44 | 2 | 6 | 6 | |||||
| Females | 394 | 38 | 47 | 2 | 8 | 5 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 144 | 46 | 47 | 1 | 4 | 1 | |||||
| 30–60 | 370 | 43 | 44 | 1 | 6 | 5 | |||||
| >60 | 146 | 25 | 47 | 4 | 13 | 10 | |||||
| Readiness to decrease sun exposure | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | −0.13** | ||||||||||
| Males | 255 | 14 | 54 | 6 | 13 | 12 | |||||
| Females | 399 | 11 | 44 | 6 | 28 | 11 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 145 | 14 | 59 | 6 | 15 | 6 | |||||
| 30–60 | 374 | 12 | 47 | 6 | 23 | 11 | |||||
| >60 | 149 | 9 | 37 | 9 | 26 | 19 | |||||
| Readiness to decrease sun exposure | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | −0.13** | ||||||||||
| Males | 255 | 14 | 54 | 6 | 13 | 12 | |||||
| Females | 399 | 11 | 44 | 6 | 28 | 11 | |||||
| Age | 0.17*** | ||||||||||
| <30 | 145 | 14 | 59 | 6 | 15 | 6 | |||||
| 30–60 | 374 | 12 | 47 | 6 | 23 | 11 | |||||
| >60 | 149 | 9 | 37 | 9 | 26 | 19 | |||||
| Readiness to increase sun protective behaviour | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | 0.17*** | ||||||||||
| Males | 252 | 5 | 32 | 4 | 33 | 26 | |||||
| Females | 398 | 2 | 18 | 1 | 39 | 40 | |||||
| Age | −0.22*** | ||||||||||
| <30 | 178 | 1 | 14 | 3 | 36 | 47 | |||||
| 30–60 | 348 | 3 | 23 | 2 | 37 | 35 | |||||
| >60 | 144 | 8 | 32 | 4 | 38 | 19 | |||||
| Readiness to increase sun protective behaviour | N | Stage of change | Sommer's d | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Precontemplation (%) | Contemplation (%) | Preparation (%) | Action (%) | Maintenance (%) | |||||||
| Gender | 0.17*** | ||||||||||
| Males | 252 | 5 | 32 | 4 | 33 | 26 | |||||
| Females | 398 | 2 | 18 | 1 | 39 | 40 | |||||
| Age | −0.22*** | ||||||||||
| <30 | 178 | 1 | 14 | 3 | 36 | 47 | |||||
| 30–60 | 348 | 3 | 23 | 2 | 37 | 35 | |||||
| >60 | 144 | 8 | 32 | 4 | 38 | 19 | |||||
P < 0.001; **P < 0.01; *P < 0.05
Women intended more often to decrease their sunbathing and to protect themselves from the sun than men. Older persons were more likely than younger ones to intend to decrease their sunbathing. However, younger persons were more likely to protect themselves from the sun. Approximately 80% of people <30 years of age responded that they tried to protect themselves from the sun.
Associations between optimism and other variables
To explore the variables that are related to optimistic bias, correlations were calculated between frequency of sun exposure, perceptions of risk, and seriousness of skin cancer, treatability, etc. and optimism. The results are shown in table 4. The strongest correlation was a negative association found between optimistic bias and perception of likelihood of developing skin cancer. Believing to have an increased risk of developing skin cancer and worry about developing skin cancer along with a readiness to change sunbathing behaviours were related to low degree of optimistic bias. The only factor positively associated with optimistic bias was a perceived ability to protect oneself from the damaging rays of the sun.
Bivariate correlations between optimism and other variables using Spearman's rho correlation coefficient
| Spearman's Rho | |
|---|---|
| Time spent in the sun | 0.057 |
| Frequency of sunbathing | 0.054 |
| Seriousness | 0.02 |
| Preventability | 0.11* |
| Treatability | 0.01 |
| How often one worries of getting skin cancer | −0.28** |
| Likeliness of developing skin cancer | −0.40** |
| Annual incidence of skin cancer | −0.06 |
| Impact of sun exposure on skin-cancer incidence | −0.05 |
| Readiness to change sunbathing behaviour | −0.20** |
| Intention to stop sunbathing | −0.15** |
| Intention to decrease sunbathing | −0.16** |
| Intention to increase use of sun protection | −0.15** |
| Spearman's Rho | |
|---|---|
| Time spent in the sun | 0.057 |
| Frequency of sunbathing | 0.054 |
| Seriousness | 0.02 |
| Preventability | 0.11* |
| Treatability | 0.01 |
| How often one worries of getting skin cancer | −0.28** |
| Likeliness of developing skin cancer | −0.40** |
| Annual incidence of skin cancer | −0.06 |
| Impact of sun exposure on skin-cancer incidence | −0.05 |
| Readiness to change sunbathing behaviour | −0.20** |
| Intention to stop sunbathing | −0.15** |
| Intention to decrease sunbathing | −0.16** |
| Intention to increase use of sun protection | −0.15** |
P < 0.01; *P < 0.05
Bivariate correlations between optimism and other variables using Spearman's rho correlation coefficient
| Spearman's Rho | |
|---|---|
| Time spent in the sun | 0.057 |
| Frequency of sunbathing | 0.054 |
| Seriousness | 0.02 |
| Preventability | 0.11* |
| Treatability | 0.01 |
| How often one worries of getting skin cancer | −0.28** |
| Likeliness of developing skin cancer | −0.40** |
| Annual incidence of skin cancer | −0.06 |
| Impact of sun exposure on skin-cancer incidence | −0.05 |
| Readiness to change sunbathing behaviour | −0.20** |
| Intention to stop sunbathing | −0.15** |
| Intention to decrease sunbathing | −0.16** |
| Intention to increase use of sun protection | −0.15** |
| Spearman's Rho | |
|---|---|
| Time spent in the sun | 0.057 |
| Frequency of sunbathing | 0.054 |
| Seriousness | 0.02 |
| Preventability | 0.11* |
| Treatability | 0.01 |
| How often one worries of getting skin cancer | −0.28** |
| Likeliness of developing skin cancer | −0.40** |
| Annual incidence of skin cancer | −0.06 |
| Impact of sun exposure on skin-cancer incidence | −0.05 |
| Readiness to change sunbathing behaviour | −0.20** |
| Intention to stop sunbathing | −0.15** |
| Intention to decrease sunbathing | −0.16** |
| Intention to increase use of sun protection | −0.15** |
P < 0.01; *P < 0.05
Discussion
The perception of own susceptibility to harm is essential in theories regarding self-protective behaviour.18,19 The participants in this study seemed to have realistic believes about the contribution of solar radiation to the risk of developing skin cancer; however, they seriously underestimates skin cancer incidence in the population and the impact of skin cancer on general health. The optimistic bias for developing skin cancer was not extensive. It was positively related to the ability to protect and negatively to the worry about skin cancer and perception of an elevated risk of developing skin cancer. According to these results people seem to be quite rational in their judgment of risk, and the results correspond well with the earlier studies examining the effect of preventability, worry, and susceptibility on optimistic bias.11 However, men seemed to be more optimistic about their chances of getting skin cancer despite the fact that they are much more likely than women to be diagnosed with a malignant skin tumour. This could be a result of an unclear risk perception concerning sun exposure, and the distinction between intentional and unintentional sun exposure. The results in this study indicate that women sunbathe intentional to a much higher degree than men. This has been shown in several other studies in Sweden.20–22 But as shown in this study, men seem to stay in the sun almost equally long as women, probably resulting in equal amount of ultraviolet exposure and an equal increase in the risk of developing skin cancer. The optimism among men could be due to a belief that sunbathing is a risk factor for skin cancer but sun exposure during other activities is not.
To date, most skin cancer preventive interventions have been concerned with information about proper ways of protection from the sun and reducing sunburn, and informing people to be cautious in the sun especially in the beginning of summer. Campaigns informing people about skin cancer and the harmful effect of sun exposure have been avoided for the reason that they would scare the people. The results from this study indicate that a potential effective strategy to alter people's sun exposure could be to induce a more realistic risk perception. There were positive correlations between optimism and all measures of readiness to change behaviour in the sun. A more realistic perception of risk could thus lead to decreased sunbathing and an increased use of sun protection. People seem to be aware of the fact that sun exposure is important, but they fail to use this information in a consistent way to formulate a judgment of their own vulnerability to harm. There seem to be a need for information about the high incidence of skin cancer, the personal risk factors, and the fact that unintentional as well as intentional sun exposures are risk factors for skin cancer. Finally, people need not only have a realistic perception of their own risk but also to have a realistic perception of what they have to gain by protective behaviour and avoiding the sun, and should be properly informed about the benefits along with preventive action.
A limitation in this study was the selective population. Those included in this study were self-selected individuals who had taken action to have their skin screened for skin cancer, and thus, they are likely to be more interested in skin cancer and about their health that population in general. The relatively low degree of optimistic bias observed in this study, could either be a result of the selective population that this study was conducted in, or a result of the fact that skin cancer is not included in the types of health hazards that are subject to unrealistic bias. The former could be supported by the fact that all participants was recruited at a skin check-up facility, and thus the participants could be at higher risk of actually having skin cancer or they might be more health concerned and generally more knowledgeable about skin cancer. The latter is supported by other studies of the phenomena in relation to different health behaviours.12 There are also difficulties in assessing the degree of optimism. Generally, in survey studies, optimistic bias can be measured either with comparative or with absolute measurement. When optimism is measured as an absolute measure the interviewees are asked to judge their own vulnerability and other people's vulnerability separately, and the bias is calculated afterwards by the researcher. With comparative measure of optimism the interviewee is asked to make the comparison themselves and respond to what degree their own vulnerability differs from that of other people. In this study we used one item to assess the comparative measure of optimistic bias. Larger degrees of bias could possibly have been found using an absolute measurement of degree of optimistic bias. It was, however, essential in this study to keep the number of items low as the respondents were recruited while they were waiting for a medical skin check-up in a campaign area.
Conclusion
People concerned about skin cancer seem to be aware of the fact that sun exposure is an important risk factor for skin cancer, but they fail to use this information in a consistent way to formulate a judgment of their own vulnerability to harm. People need to be informed about the high incidence of skin cancer, the personal risk factors of skin cancer, and the fact that unintentional as well as intentional sun exposure increases the risk of developing skin cancer.
This research was funded by the Swedish Cancer Society and the Stockholm County Council.
The paper examines the associations between risk perceptions, sun-related behaviour, readiness to change, and optimism bias.
People seem to be aware of the fact that sun exposure is an important risk factor for skin cancer.
People fail to formulate a judgment of their own vulnerability to harm.
People need to be informed about the high incidence of skin cancer and the personal risk factors of skin cancer.
References
Weinstock MA, Colditz GA, Willett WC, et al. Nonfamilial cutaneous melanoma incidence in women associated with sun exposure before 20 years of age.
Westerdahl J, Olsson H, Ingvar C. At what age do sunburn episodes play a crucial role for the development of malignant melanoma [published erratum appears in Eur J Cancer
Armstrong BK, Kricker A. The epidemiology of UV induced skin cancer.
Augustsson A, Stierner U, Rosdahl I, Suurkula M. Regional distribution of melanocytic naevi in relation to sun exposure, and site-specific counts predicting total number of naevi [see comments].
Bränström R, Brandberg Y. Behavioural aspects on prevention of malignant skin tumors. Stockholm: Swedish Radiation Protection Authority,
Weinstein ND. Unrealistic optimism about susceptibility to health problems: conclusions from a community-wide sample.
Eiser JR. Skin cancer: assessing perceived risk and behavioural attitudes.
Prochaska JO, Velicer WF, Rossi JS, et al. Stages of change and decisional balance for 12 problem behaviors.
Bränström R, Kristjansson S, Ullén H, Brandberg Y. Stability of questionnaire items measuring behaviors, attitudes, and stages of change related to sun exposure.
Siegel S. Nonparametric statistics for the behavioural sciences. Tokyo: McGraw-Hill Kogakusha,
Glanz K, Lewis FM, Rimer BK. Health Behaviour and Health Education. 3rd Edn. San Francisco: Jossey-Bass,
Brandberg Y, Ullén H, Sjöberg L, Holm LE. Sunbathing and sunbed use related to self-image in a randomized sample of Swedish adolescents.
Bränström R, Ullén H, Brandberg Y. A randomized population-based intervention to examine the effect of the UV index on tanning behavior.

{kind=link}
{kind=link}
Comments