




Abstract
Background: Narghile is a resurging smoking device. However, little research has been done to assess passive smoking exposure. The objective of the present study is to evaluate the exposure of pre-school age children in Beirut to parental passive smoking from cigarette and/or narghile. Methods: Data were collected from 1057 pre-school age children attending 16 day cares and 7 nursery schools in the city of Beirut. Results: The overall prevalence of parental smoking (cigarette and/or narghile) was 53.3%. Ten per cent of respondents reported smoking only narghile. Fathers were significantly more likely than mothers to smoke cigarettes. However, there was no significant difference between fathers and mothers with respect to smoking narghile only. Education was a significant predictor for smoking cigarettes but not for smoking narghile. Conclusion: Narghile smoking appears to follow different gender and social patterns than cigarette smoking. Further research is needed to establish the determinants of narghile smoking, in order to develop adequate prevention policies.
Smoking is a major cause of cancer,1 respiratory,2 and circulatory diseases.3,4 Despite various anti-smoking initiatives, estimates point to more than one billion smokers and four million annual deaths from tobacco worldwide.5 Non-smokers are also at risk when they are exposed to tobacco smoke. Passive tobacco smoking represents a main health hazard to children, possibly leading to otitis media, development or exacerbation of asthma, and other respiratory diseases.6
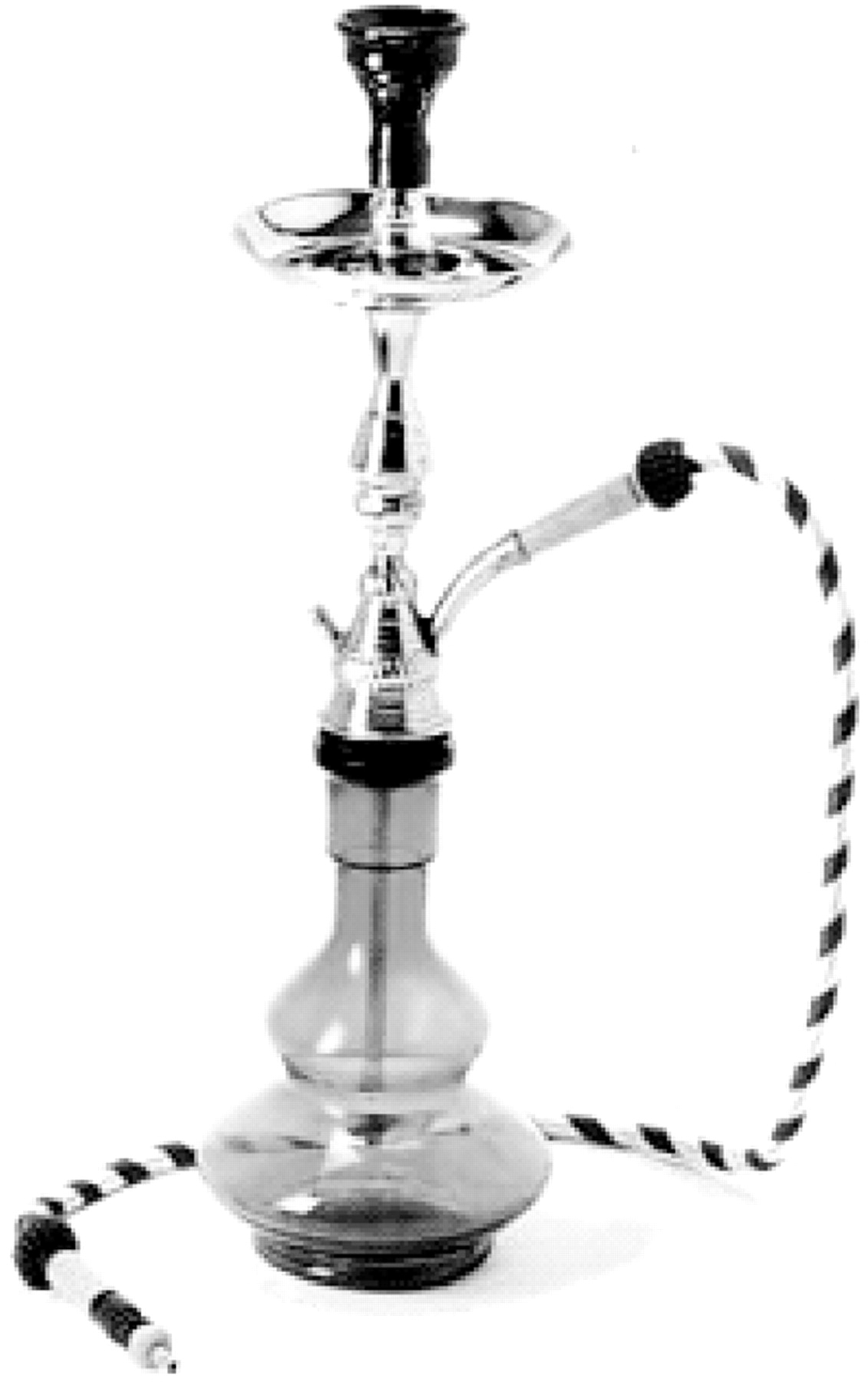
In Lebanon, there has been a revival of narghile smoking over the last decade. Narghile (also known as water-pipe, shisha, hookah, or hubble bubble) has been practiced for centuries in the Middle East. The main ingredient of narghile is the ‘tumbak’, a dark-paste tobacco lit by charcoal embers. The tumbak is piled on a tray atop a pipe connected to a glass bottle that is half-filled with water, and a burning charcoal is placed directly on the tumbak (figure 1). When the smoker sucks on the pipe, emissions from the burning tobacco travel through the water before being inhaled into the lungs. A recent study found that the total particulate matter (TPM) that is inhaled by narghile smokers is 1.10 g/h.7 When compared with a range from 1 to 27 mg of TPM per single cigarette,8 this hourly inhalation of TPM with narghile would equate to a mean of five packs per day of cigarettes. A literature search yields no reports about amounts of passive TPM exposure from narghile.
Whereas many studies have looked at children's exposure to passive cigarette smoking,9,10 no studies, to our knowledge, have investigated the exposure to passive narghile smoking of children less than 5 years of age. The objective of the present study is to evaluate the exposure of pre-school age children in Beirut to parental passive smoking from cigarette and/or narghile, and to identify its distribution between mothers and fathers and across the different education and occupation levels. This will help in assessing the magnitude of the problem so that adequate policies can be developed.
Methods
The study was cross-sectional in design. Pre-school in Lebanon is mandatory from the age of 4 and the proportion of non-attending children is expected to be small. A convenient sample of 23 institutions including 16 day cares and 7 nursery schools were selected based on the phone directory. The schools were selected to include children from both east and west Beirut and from all socio-economic background and the country's two major sects (Christians and Moslems). No institution refused to participate. Consent was sought from the administrative boards of each institution. Questionnaires were sent home with the children for their parents to fill. The questionnaire included information on socio-demographic characteristics, smoking behaviour (including dose and frequency) of each parent at the household level, and type of tobacco smoked (cigarettes or narghile). Response rate of filled questionnaires was above 90%. Collected data were analysed using the Statistical Package for Social Sciences (SPSS) Software version 11. χ2 statistics were calculated to determine the association between the gender and the smoking methods of the parents. The t-test statistics were calculated to determine the relation between the dose of cigarette and the rate of narghile smoking across both genders. Three stepwise logistic regression models were performed separately for mothers and fathers; where the dependent variables were smoking either cigarettes or narghile, smoking cigarettes only, and smoking narghile only. The independent variables were education, occupation, and the smoking status of the spouse. Odds ratios (OR) and 95% confidence intervals (CI) for the variables selected in these models were reported.
Results
The total number of children recruited in the study was 1057, of which 53% were boys and 47% were girls. Their age ranged from a few months to 6.5 years (mean ± SD: 3.97 ± 1.49 years). table 1 shows the overall prevalence of different types of smoking at the household level and among fathers and mothers. The overall prevalence of household smoking (either cigarette and/or narghile) in the sample was 53.3%. Fathers were significantly more likely than mothers to smoke only cigarettes, or both cigarettes and narghile. However, there was no significant difference between fathers and mothers with respect to smoking narghile only. A total of 17.2% of the households had both mothers and fathers smoking cigarette and/or narghile. Fathers were found to be significantly more likely to smoke a higher dose of cigarettes than mothers (respectively, 17.7 versus 15.3 cigarettes per day; P = 0.01) but no similar significance was observed for the difference in rates of narghile between fathers and mothers (respectively, 3.7 versus 3.5 narghile smoking times per week; P = 0.67).
Smoking prevalence (%) by type of smoking and gender
| Totala | Mothers | Fathers | P | |
|---|---|---|---|---|
| n (%)b | n (%)b | n (%)b | ||
| Non-smokers | 494 (46.7) | 778 (73.6) | 607 (57.4) | 1 |
| Cigarette and/or narghile smoking | 563 (53.3) | 279 (26.4) | 450 (42.6) | <0.001 |
| Cigarette smoking only | 380 (36.0) | 175 (16.6) | 334 (31.6) | <0.001 |
| Mean 1c (SD) | 15.3 (10.5) | 17.7 (11.7) | 0.01 | |
| Narghile smoking only | 103 (9.7) | 90 (8.5) | 89 (8.4) | 0.14 |
| Mean 2d (SD) | 3.5 (3.4) | 3.7 (2.9) | 0.67 | |
| Both cigarette and narghile smoking | 34 (3.2) | 14 (1.3) | 27 (2.6) | 0.005 |
| Totala | Mothers | Fathers | P | |
|---|---|---|---|---|
| n (%)b | n (%)b | n (%)b | ||
| Non-smokers | 494 (46.7) | 778 (73.6) | 607 (57.4) | 1 |
| Cigarette and/or narghile smoking | 563 (53.3) | 279 (26.4) | 450 (42.6) | <0.001 |
| Cigarette smoking only | 380 (36.0) | 175 (16.6) | 334 (31.6) | <0.001 |
| Mean 1c (SD) | 15.3 (10.5) | 17.7 (11.7) | 0.01 | |
| Narghile smoking only | 103 (9.7) | 90 (8.5) | 89 (8.4) | 0.14 |
| Mean 2d (SD) | 3.5 (3.4) | 3.7 (2.9) | 0.67 | |
| Both cigarette and narghile smoking | 34 (3.2) | 14 (1.3) | 27 (2.6) | 0.005 |
a: Total refers to smoking at household level, including mothers, fathers, or any other household resident
b: Column percentage
c: Average number of cigarettes smoked daily
d: Average number of times of narghile smoking during 1 week
Smoking prevalence (%) by type of smoking and gender
| Totala | Mothers | Fathers | P | |
|---|---|---|---|---|
| n (%)b | n (%)b | n (%)b | ||
| Non-smokers | 494 (46.7) | 778 (73.6) | 607 (57.4) | 1 |
| Cigarette and/or narghile smoking | 563 (53.3) | 279 (26.4) | 450 (42.6) | <0.001 |
| Cigarette smoking only | 380 (36.0) | 175 (16.6) | 334 (31.6) | <0.001 |
| Mean 1c (SD) | 15.3 (10.5) | 17.7 (11.7) | 0.01 | |
| Narghile smoking only | 103 (9.7) | 90 (8.5) | 89 (8.4) | 0.14 |
| Mean 2d (SD) | 3.5 (3.4) | 3.7 (2.9) | 0.67 | |
| Both cigarette and narghile smoking | 34 (3.2) | 14 (1.3) | 27 (2.6) | 0.005 |
| Totala | Mothers | Fathers | P | |
|---|---|---|---|---|
| n (%)b | n (%)b | n (%)b | ||
| Non-smokers | 494 (46.7) | 778 (73.6) | 607 (57.4) | 1 |
| Cigarette and/or narghile smoking | 563 (53.3) | 279 (26.4) | 450 (42.6) | <0.001 |
| Cigarette smoking only | 380 (36.0) | 175 (16.6) | 334 (31.6) | <0.001 |
| Mean 1c (SD) | 15.3 (10.5) | 17.7 (11.7) | 0.01 | |
| Narghile smoking only | 103 (9.7) | 90 (8.5) | 89 (8.4) | 0.14 |
| Mean 2d (SD) | 3.5 (3.4) | 3.7 (2.9) | 0.67 | |
| Both cigarette and narghile smoking | 34 (3.2) | 14 (1.3) | 27 (2.6) | 0.005 |
a: Total refers to smoking at household level, including mothers, fathers, or any other household resident
b: Column percentage
c: Average number of cigarettes smoked daily
d: Average number of times of narghile smoking during 1 week
Stepwise regression analyses revealed a significant inverse relationship between both father and mother educational level and smoking cigarette but not narghile (table 2). Adjusting for the education, the parent (mother or father) was three times at higher odds of smoking cigarettes if his (her) spouse smoked cigarettes, whereas the parent was 20 times at higher odds of smoking narghile if his (her) spouse smoked narghile; OR = 19.7, 95% CI = 10.8–35.9.
Results of stepwise logistic regression by gender, education, occupation, and status of smoking of the spouse
| Smoking cigarette and/or narghile | Smoking cigarettes only | Smoking narghile only | ||||
|---|---|---|---|---|---|---|
| ORa (95% CIb) | ORa (95% CIb) | ORa (95% CIb) | ||||
| Mothers | ||||||
| Mother's education | ||||||
| Primary | 2.3 (1.3–3.9) | 3.2 (1.7–5.6) | – | |||
| Intermediate | 2.0 (1.3–3.0) | 2.5 (1.6–4.0) | – | |||
| Secondary | 1.6 (1.1–2.3) | 1.7 (1.1–2.6) | – | |||
| University | 1 | 1 | – | |||
| Mother's occupation | ||||||
| Housewife | – | – | – | |||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Smoking status of father | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.8 (2.0–3.8) | 2.9 (2.1–4.2) | 2.6 (1.5–4.7) | |||
| Narghile only | 5.9 (3.6–9.5) | 1.2 (0.6–2.8) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.5 (1.1–5.7) | 0.3 (0.04–2.6) | 2.5 (0.5–11.4) | |||
| Fathers | ||||||
| Father's education | ||||||
| Primary | 3.0 (1.9–4.7) | 3.3 (2.1–5.4) | – | |||
| Intermediate | 2.1 (1.5–3.1) | 2.1 (1.4–3.2) | – | |||
| Secondary | 1.4 (1.0–1.9) | 1.3 (0.9–1.8) | – | |||
| University | 1 | 1 | – | |||
| Father's occupation | ||||||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Administrative | – | – | – | |||
| Smoking status of mother | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.6 (1.9–3.7) | 3.2 (2.2–4.4) | 1.4 (0.6–3.2) | |||
| Narghile only | 5.3 (3.2–8.7) | 2.7 (1.5–4.9) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.9 (0.9–8.9) | – | 4.9 (0.9–26.4) | |||
| Smoking cigarette and/or narghile | Smoking cigarettes only | Smoking narghile only | ||||
|---|---|---|---|---|---|---|
| ORa (95% CIb) | ORa (95% CIb) | ORa (95% CIb) | ||||
| Mothers | ||||||
| Mother's education | ||||||
| Primary | 2.3 (1.3–3.9) | 3.2 (1.7–5.6) | – | |||
| Intermediate | 2.0 (1.3–3.0) | 2.5 (1.6–4.0) | – | |||
| Secondary | 1.6 (1.1–2.3) | 1.7 (1.1–2.6) | – | |||
| University | 1 | 1 | – | |||
| Mother's occupation | ||||||
| Housewife | – | – | – | |||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Smoking status of father | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.8 (2.0–3.8) | 2.9 (2.1–4.2) | 2.6 (1.5–4.7) | |||
| Narghile only | 5.9 (3.6–9.5) | 1.2 (0.6–2.8) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.5 (1.1–5.7) | 0.3 (0.04–2.6) | 2.5 (0.5–11.4) | |||
| Fathers | ||||||
| Father's education | ||||||
| Primary | 3.0 (1.9–4.7) | 3.3 (2.1–5.4) | – | |||
| Intermediate | 2.1 (1.5–3.1) | 2.1 (1.4–3.2) | – | |||
| Secondary | 1.4 (1.0–1.9) | 1.3 (0.9–1.8) | – | |||
| University | 1 | 1 | – | |||
| Father's occupation | ||||||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Administrative | – | – | – | |||
| Smoking status of mother | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.6 (1.9–3.7) | 3.2 (2.2–4.4) | 1.4 (0.6–3.2) | |||
| Narghile only | 5.3 (3.2–8.7) | 2.7 (1.5–4.9) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.9 (0.9–8.9) | – | 4.9 (0.9–26.4) | |||
a: Odds ratio
b: Confidence interval
Results of stepwise logistic regression by gender, education, occupation, and status of smoking of the spouse
| Smoking cigarette and/or narghile | Smoking cigarettes only | Smoking narghile only | ||||
|---|---|---|---|---|---|---|
| ORa (95% CIb) | ORa (95% CIb) | ORa (95% CIb) | ||||
| Mothers | ||||||
| Mother's education | ||||||
| Primary | 2.3 (1.3–3.9) | 3.2 (1.7–5.6) | – | |||
| Intermediate | 2.0 (1.3–3.0) | 2.5 (1.6–4.0) | – | |||
| Secondary | 1.6 (1.1–2.3) | 1.7 (1.1–2.6) | – | |||
| University | 1 | 1 | – | |||
| Mother's occupation | ||||||
| Housewife | – | – | – | |||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Smoking status of father | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.8 (2.0–3.8) | 2.9 (2.1–4.2) | 2.6 (1.5–4.7) | |||
| Narghile only | 5.9 (3.6–9.5) | 1.2 (0.6–2.8) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.5 (1.1–5.7) | 0.3 (0.04–2.6) | 2.5 (0.5–11.4) | |||
| Fathers | ||||||
| Father's education | ||||||
| Primary | 3.0 (1.9–4.7) | 3.3 (2.1–5.4) | – | |||
| Intermediate | 2.1 (1.5–3.1) | 2.1 (1.4–3.2) | – | |||
| Secondary | 1.4 (1.0–1.9) | 1.3 (0.9–1.8) | – | |||
| University | 1 | 1 | – | |||
| Father's occupation | ||||||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Administrative | – | – | – | |||
| Smoking status of mother | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.6 (1.9–3.7) | 3.2 (2.2–4.4) | 1.4 (0.6–3.2) | |||
| Narghile only | 5.3 (3.2–8.7) | 2.7 (1.5–4.9) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.9 (0.9–8.9) | – | 4.9 (0.9–26.4) | |||
| Smoking cigarette and/or narghile | Smoking cigarettes only | Smoking narghile only | ||||
|---|---|---|---|---|---|---|
| ORa (95% CIb) | ORa (95% CIb) | ORa (95% CIb) | ||||
| Mothers | ||||||
| Mother's education | ||||||
| Primary | 2.3 (1.3–3.9) | 3.2 (1.7–5.6) | – | |||
| Intermediate | 2.0 (1.3–3.0) | 2.5 (1.6–4.0) | – | |||
| Secondary | 1.6 (1.1–2.3) | 1.7 (1.1–2.6) | – | |||
| University | 1 | 1 | – | |||
| Mother's occupation | ||||||
| Housewife | – | – | – | |||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Smoking status of father | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.8 (2.0–3.8) | 2.9 (2.1–4.2) | 2.6 (1.5–4.7) | |||
| Narghile only | 5.9 (3.6–9.5) | 1.2 (0.6–2.8) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.5 (1.1–5.7) | 0.3 (0.04–2.6) | 2.5 (0.5–11.4) | |||
| Fathers | ||||||
| Father's education | ||||||
| Primary | 3.0 (1.9–4.7) | 3.3 (2.1–5.4) | – | |||
| Intermediate | 2.1 (1.5–3.1) | 2.1 (1.4–3.2) | – | |||
| Secondary | 1.4 (1.0–1.9) | 1.3 (0.9–1.8) | – | |||
| University | 1 | 1 | – | |||
| Father's occupation | ||||||
| Skilled/unskilled | – | – | – | |||
| Technical | – | – | – | |||
| Professional | – | – | – | |||
| Administrative | – | – | – | |||
| Smoking status of mother | ||||||
| None | 1 | 1 | 1 | |||
| Cigarette only | 2.6 (1.9–3.7) | 3.2 (2.2–4.4) | 1.4 (0.6–3.2) | |||
| Narghile only | 5.3 (3.2–8.7) | 2.7 (1.5–4.9) | 19.7 (10.8–35.9) | |||
| Cigarette and/or narghile | 2.9 (0.9–8.9) | – | 4.9 (0.9–26.4) | |||
a: Odds ratio
b: Confidence interval
Discussion
More than 53% of the pre-school age children in this study are exposed to parental passive smoking of either cigarette and/or narghile. To our knowledge this is the first study to address the issue of exposure of children less than 6 years of age to passive smoking of narghile, hence making comparison with other countries difficult. The study does not address exposure of children from other sources and at other locations, including smoking household members other than parents, cigarette smoking at school and in school buses, cigarette and narghile smoking in public places, and so on. Therefore, the figures reported here must be viewed as a minimum estimate of exposure of pre-school children to passive smoking.
The prevalence of passive exposure to cigarettes among pre-school children in the present study (36%) is markedly higher than that reported by the National Health Interview Survey in the United States in 2000, which estimates that children's passive smoking exposure at homes declined from 36% to 25% between 1992 and 2000.10 One study form Iran looks specifically at cigarette-smoking fathers and finds that 41% of 622 children aged 6 months to 5 years live in houses where fathers smoke, compared to 31.6% of smoking fathers in our study.9
Male gender is positively associated with parental cigarette smoking. This is consistent with other surveys conducted in Syria which report a smoking rate of 48% among adult males, compared to 9% among adult females.11 The gender difference in parental cigarette smoking rates in Lebanon (31.6% versus 16.6%) is not as pronounced. Maziak11 attributes the rate of female smoking in Syria to conservative social attitudes and a low level of social liberalization. Accordingly, a higher degree of Westernization in Beirut, compared to other cities in the Arab world, could also explain the higher rates of parental female smoking. On the other hand, narghile smoking does not seem to follow a gendered pattern. Even the rates of narghile smoking among both sexes are very close: 3.5 times/week for mothers and 3.7 for fathers. This may be due to the fact that, despite relaxed attitudes to female cigarette smoking, female narghile smoking is still more socially acceptable.
In line with other reports we found that educational level of parents was significantly related to cigarette smoking.12 However, this relationship was not present for narghile smoking. The strong relationship between smoking narghile of both parents observed in the study suggests the socially encouraged habit practiced by different family members.
Narghile smoking is a culturally-specific practice that is intimately linked to social patterns of sociability and hospitality. Therefore, socio-cultural dimensions, such as age, religious beliefs, and cultural affiliations, must be explored to develop a better understanding of the determinants of prevalence. Most importantly, the gendered patterns of cigarette smoking cannot be extrapolated to narghile unless empirical evidence to the contrary is established.
Objective is to determine the prevalence of passive exposure to cigarettes and/or narghile smoke among pre-school children.
Results showed that narghile smoking follows different gender and social patterns than cigarette smoking.
Need to establish the determinants of narghile smoking in order to develop adequate prevention policies.
This work was carried out with the aid of a grant from Research for International Tobacco Control (RITC), an international secretariat housed at the International Development Research Center (IDRC), in Ottawa.
References
Burns DM. Epidemiology of smoking-induced cardiovascular disease.
Bonita R, Duncan J, Truelsen T, et al. Passive smoking as well as active smoking increases the risk of acute stroke.
WHO. World Health Organization, 2006. Tobacco Free Initiative: Why is tabacco health a public health priority. Available at http://www.who.int/tobacco/en/ Last accessed March 15, 2006.
Tamim H, Musharrafieh U, El Roueiheb Z, et al. Exposure of children to environmental tobacco smoke (ETS) and its association with respiratory ailments.
Shihadeh A, Azar S, Antonios C, Haddad A. Towards a topographical model of narghile water-pipe cafe smoking: a pilot study in a high socioeconomic status neighborhood of Beirut, Lebanon.
Shihadeh A, Saleh R. Polycyclic aromatic hydrocarbons, carbon monoxide, “tar”, and nicotine in the mainstream smoke aerosol of the narghile water pipe.
Shiva F, Nasiri M, Sadeghi B, Padyab M. Effects of passive smoking on common respiratory symptoms in young children.
Soliman S, Pollack HA, Warner KE. Decrease in the prevalence of environmental tobacco smoke exposure in the home during the 1990s in families with children.
Maziak W. Smoking in Syria: profile of a developing Arab country.

{kind=link}
{kind=link}
Comments
Measuring Real Exposure to Narghile (Hookah, Shisha) Smoke
and Other Concerns Related to Public Health
ÂÂ
Below are comments on the new study published by AUB (American University of Beirut) researchers:
Tamim H, Akkary G, El-Zein A, El-Roueiheb Z, El-Chemaly S. Exposure of pre-school children to passive cigarette and narghile smoke in Beirut. European Journal of Public Health 2006 (May 4): 4 pages.
ÂÂ
KEYPOINTS :
1-     Measuring Real Exposure to Narghile (Hookah, Shisha) Smoke
2-     Nature of Narghile Environmental Smoke
3-     Confusion about Smoked Products
4-     Does 1 Narghile Equal 100 Cigarettes or only 1 Cigarette ?
5-     Gender Differences
6-     Containing Growing Confusion
ÂÂ
1- Measuring Real Exposure to Narghile (Hookah, Shisha) Smoke
The aim of the study was to focus on narghile passive smoking but we are afraid the objective was missed for obvious methodological reasons. Certainly all the provided figures are useful for passive cigarette smoking in Beirut and this is because cigarettes can unfortunately be used in any room of the apartment or house the parents are living in with their children. This notwithstanding, we must point out here, for those who do not know the Oriental way of life, that narghile (hookah, shisha) is generally and preferably smoked outside: on the balcony, in the garden, on the roof terrace, etc. In these conditions, we are afraid no conclusion can be drawn from the figures given in the table as they not reflect the real exposure of children to narghile smoke. We regret that this fact was glossed over when the questionnaire was designed. We have repeatedly been warning over the past years against the misuse of questionnaires in surveys about narghile smoking (1, 2). Indeed, there are similarities and dissimilarities between cigarette and narghile smoking and these must be clearly identified (3).
Besides, The nature of smoke is highly different from that produced by cigarettes, particularly regarding the so-called environmental one at the heart of the a.m. study. This is because water is very efficient in this respect. As Deckers and her team rightly note: “One of the only articulated benefits to this tobacco alternative is the minimal release of sidestream smoke, which would ultimately place by-standers at risk for ETS exposure” (4).
2-Nature of Narghile Environmental Smoke
Smoke constituents in the case of the hookah are filtered out in three different ways and to varying degrees. Firstly, inside the water vessel; secondly during the long run of the smoke, from the bowl at the top to the nozzle at the end of the long suction hose, a distance of about two meters on average that may however reach much longer figures. Thirdly, during the production of smoke itself because the temperatures are extremely low in comparison with that at the burning tip of a cigarette. From a chemical point of view, this has great consequences. For instance, not only there is a “minimal release of sidestream smoke” (4) but even the mainstream smoke is freed, to a great proportion, from famous irritants like acrolein, acetaldehyd, formaldehyd, and other elements (5). This is why the resulting corresponding smoke is felt as “milder” than the harsh one produced by cigarette, even for non-smokers. Indeed, in our endeavour to develop a nationwide plan for hookah use prevention in France relying on human non-machine narghile smoking, we are taking this fact into consideration. This intelligent approach will allow us to gain credibility among smokers who may oppose our arguments. We only mentioned irritants but a series of studies, including unpublished ones, suggests that other dangerous elements are actually filtered out. In any case, exposure to tobacco smoke is not beneficial for health although we must keep objective in each of our statements.
3-Confusion about Smoked Products
Tamim et al. state: “ In Lebanon, there has been a revival of narghile smoking over the last decade. Narghile (also known as water-pipe, shisha, hookah, or hubble bubble) has been practiced for centuries in the Middle East. The main ingredient of narghile is the ‘tumbak’, a dark-paste tobacco lit by charcoal embers. The tumbak is piled on a tray atop a pipe connected to a glass bottle that is half-filled with water, and a burning charcoal is placed directly on the tumbak (figure 1) […]”
1-We are afraid tumbak is not a “dark-paste” tobacco. For a detailed and discussed typology of the different kinds of tobacco and tobacco-based smoking mixtures, please refer to our previous work which is, indeed, more then a mere ethnographic classification exercise (2, 5). For having not paid the required attention in this field, the authors of recent and widely advertised studies, misled by the “jurâk” misnomer, used by local scientists in Turkey, actually mistook one type for another (6). In any case, the Middle East revival and the world craze for hookah smoking is in direct relation with the use of another product: tobamel (mel is for honey in Latin), the flavoured tobacco-molasses based mixture (called mu‘assel in Arabic which literally means “honeyed”). It is absolutely not tumbak which is plain raw tobacco. Presuming that the authors actually meant tobamel, in which case the description was wrong, it is incorrect to state that it is burned (5).
Finally, by openly citing (figure 1) the name and the full address of a commercial company selling narghiles, Tamim and her team failed –by mistake, we hope- to comply with a key deontological principle of tobacco research.
4-Does 1 Narghile Equal 100 Cigarettes or only 1 Cigarette ?
Tamim et al. state: “A recent study found that the total particulate matter (TPM) that is inhaled by narghile smokers is 1.10 g/h. When compared with a range from 1 to 27 mg of TPM per single cigarette, this hourly inhalation of TPM with narghile would equate to a mean of five packs per day of cigarettes”.
Firstly, the authors should know that the study they refer to did not deal with tumbak but with tobamel (7). Secondly, although we do not know where the above figures precisely come from, we will take them as granted. Interestingly enough, while all authors of recent studies on narghile focussed on nicotine or tar (the nicotine free dry particulate matter), Tamim and her colleagues insist on TPM and on making comparisons with cigarette smoking on this basis.
From the outset, let us say that the referred to study (7) did not at all establish the TPM “inhaled by narghile smokers” for the very reason that it was based on a smoking machine set with parameters and under conditions that have no relation with the reality of the human smoking behaviour, despite the underlying topography and the integral related calculus done to obtain the final mean figures used as parameters for setting the smoking machine. We would like to draw the attention of many researchers, unfamiliar with the Middle East and narghile smoking, to just one among the many details they may ignore of the complex context. The charcoal used in the corresponding experiment was of the quick-lighting type, i.e. not the natural charcoal traditionally used in the Middle East, and still it is, to a very great extent. Besides, this charcoal was kept in the same position during almost one entire hour of continuous strain smoke pumping. Obviously, such a process helped in actually charring the smoking mixture and eventually  allowed the delivery of high quantities of tar.
In any case, as we recalled recently (8), the most renown specialists, like Kozlowski for instance, actually warned against the use of smoking machines in the field of cigarettes, where, however, the smoking session (c. 5 minutes) is extremely short in comparison with the hookah (30-60 minutes)(9).
We also remind that the use of smoking machines in this field is not so recent as some people believe. Early famous studies on the chemistry of narghile smoke (10, 11) are there on the shelves of libraries. If we are to consider TPM as Tamim did, Hoffmann and his team found that, for 100g of tobacco products: a 85mm plain US cigarette would yield 6.2g of particulate materials vs. 0.74 for a narghile (a Syrian one by the way). He also found that in “1.0 g of particulate material for mainstream smoke of tobacco products”, a 85mm plain US cigarette would yield 77.4 mg of nicotine vs. 51.4 mg for the narghile. Certainly the world has changed and cigarettes changed (12) but did the chemical processes also changed so dramatically with time ?
Further to a comprehensive critical review of the related literature in this field, we conclude that the study by Rakower and Fatal (10) might be the most objective and the closest to the real world (for the given product). Unfortunately, here, we cannot go too much into the details. We just wanted to show that relativism, at the heart of the anthropology discipline, should also be placed at the centre of biomedical sciences, shouldn’t it ?
Indeed, what is the point of this global mystification with arithmetic equations like 1 narghile=200, 100, 50, 40, 10, 5, 1, 1/2 cigarette(s) as if we, ignorant customers, were attending a permanent auction sale of smoking items ? Indeed, is this a good method to design best prevention practices or the right way to discredit our work among the growing dozens of millions of users around the world ?
5-Gender Differences
Tamim et al. state: “The gender difference in parental cigarette smoking rates in Lebanon (31.6% versus 16.6%) is not as pronounced. Maziak attributes the rate of female smoking in Syria to conservative social attitudes and a low level of social liberalization. Accordingly, a higher degree of Westernization in Beirut, compared to other cities in the Arab world, could also explain the higher rates of parental female smoking. On the other hand, narghile smoking does not seem to follow a gendered pattern. Even the rates of narghile smoking among both sexes are very close: 3.5 times/week for mothers and 3.7 for fathers.”
We fear this question of “social liberalization“ and “westernisation” may reflect orientalist views even when they are put forward by “Orientals” themselves (13, 14). Contrary to all expectations and quick analysis, the revival of narghile in the Middle East, and its craze in the Arab World as a whole, show that shisha smoking is actually a strategic “liberation” instrument (we are sorry to use the same phraseology) used by women. Early pre-world craze field based socio-anthropological work established this unexpected finding (5). A similar error can be found in the first report on “Waterpipe” smoking ever published by the World Health Organisation (15). This also happened with a famous newspaper featuring a supposedly Muslim woman smoking a cigarette, breaking free from tradition and “asserting” her freedom this way (16). This last example was found to be extremely shocking for many tobacco control activists in the West who considered it was a blatant form of glamorising the use of cigarettes, particularly among non regular smoking populations.
As for the so-called “Westernization in Beirut compared to other cities in the Arab world”, this is not in agreement with our findings on smoking in the Arab world (5). One counter-example will be enough in this respect: that of Tunis, a not less “westernised” city of the Mediterranean where female parental smoking is substantial though much lower than in the Lebanese capital. There are obviously other factors at stake.
In a global world that offers only but an extremely negative, gloomy and hostile environment for new generations, we have to take care with the words we use and not mistake “westernisation” or “social liberalisation” for true individual freedom. In Syria, the female adult literacy rate reaches 74% which should be considered as a good point. Wherever neo-liberal economies of the G8 type prevail, women are necessarily victims of male exploitation, everywhere in the world and not only in countries of the so-called “developing world”. Therefore, the direct relation between cigarette smoking and “social liberalisation is certainly not a good equation.
6- Containing Growing Confusion
3 years after the World Congress on Tobacco (Helsinki, 2003), research on the hoookah is reaching unexpected levels of global confusion. Tumbak is taken for tobamel (mu‘assel)(17), jurâk for tobamel (6), a smoking machine for a narghile user (7), female users for prisoners of tradition, etc. Perhaps 30 or 40 new studies were published over the past three years and we are afraid the best work in this field still remains that of researchers from the South as we emphasized most recently (8).
Arabs would call “fawda” this kind of situation and God knows the heavy meaning of this word in their language. A famous, and very often cited though erroneous, paper, largely infused the idea that shisha smoking was keeping its users, in the Arab world, far away from reality (18). Now, In view of the growing confusion, certainly there would be some truth in adapting and rewording it title by putting: Narghile Smoking Keeps Researchers in Wonderland …
Given this situation, what can we do to help our colleagues in rationally considering the objective facts related to the growing epidemic ? Indeed, for how long again will researchers be repeating, as in this new study by Tamim et al., that more research is needed to establish the “determinants” of narghile smoking ? Certainly, the scenario proposed for Syria, a country with a similar narghile smoking profile as Lebanon, missed the point (8, 19). However, how many more studies will we need in order to begin to be able to understand what is happening in the street ? The answer to this huge question, elaborated over several years of research, is there and was published a long time ago (5). Most recently, we clearly set out, both in the Courrier des Addictions , a research journal supported by the Francophone Society of  Addictology , and in the first issue of Tabaccologia , the guidelines and principles for any work in this field (1, 2). We do refer to publications in French and Italian journals –with English abstracts- as we are commenting on a paper of the European Journal of Public Health . Moreover, it is clear that many researchers in a francophone country like Lebanon can read French, can’t they?
Has not the time come to serenely work and reflect on narghile (hookah, shisha) smoking? Has not the time come for our colleagues and officials in charge of public health, apparently very concerned by the new world “epidemic”, to sit at a table and share with us the Middle East Peace Pipe and pay attention to what we have been saying for years now (8) in highly relevant publications (1, 2, 5, 20) ? For instance, the “new” quantitative findings that “narghile smoking follows different gender and social patterns than cigarette smoking” (17) are actually supported by previous qualitative work carried on 10 years ago (21). If, in the future, Tamim and hers colleagues envisage to lead more studies on this sensitive and complex field, we strongly invite them to participate in the novel cooperation project we are launching for researchers in this field (8).
ÂÂ
Kamal Chaouachi (kamcha[A]gmail.com)
Researcher in Socio-Anthropology and Tobaccology
Consultant in Tobacco Control (Paris)
ÂÂ
REFERENCES
(1) CHAOUACHI Kamal. Shisha, hookah. Le narguilé au XXIe siècle. Bref état des connaissances scientifiques. [Eng.: Narghile, Hookah in the 21st Century: An Overview of the Scientific Knowledge]. Le Courrier des Addictions 2004 (Oct) ; 6 (4) : 150-2. Full English version available .
(2) CHAOUACHI K. A 60 page Tetralogy on Narghile (Hookah, Shisha) Smoking and Health published in Tabaccologia , the official Journal of the Italian Society of Tobaccology : Introduction (Tabaccologia 2005; 1: 39-47); Pharmacology ( 2005 ; 3: 27-33 ); Health Aspects ( 2006;1:27-34 ); Prevention (forthcoming). Includes English abstracts. www.tabaccologia.org/archivio.htm
(3) CHAOUACHI K. Letter to the Editor: The Social Context of Individual and Collective Smoking: Similarities and Differences. Tobacco Control 2006 (1 April). A critical analysis of Poland’ study. http://tc.bmjjournals.com/cgi/eletters/15/1/59
(4) DECKERS SK, FARLEY J, HEATH J. Tobacco and its trendy alternatives: implications for pediatric nurses. Crit Care Nurs Clin North Am. 2006 Mar;18(1):95-104.
(5) CHAOUACHI K. Le narguilé : analyse socio-anthropologique. Culture, convivialité, histoire et tabacologie d’un mode d’usage populaire du tabac . Transdisciplinary doctoral thesis, Université Paris X (France), 420 pages. [Engl.: "Narghile (hookah): a Socio-Anthropological Analysis. Culture, Conviviality, History and Tobaccology  of a Popular Tobacco Use Mode”] .
(6) NATTO  S, BALJOON M, BERGSTROM J. Tobacco Smoking and Periodontal Health in a Saudi Arabian Population . Journal of Periodontology 2005; 76 (11): 1919-26.
(7) SHIHADEH A,  SALEH R. Food and Chemical Toxicology : Polycyclic aromatic hydrocarbons, carbon monoxide, “tar”, and nicotine in the mainstream smoke aerosol of the narghile water pipe. Food and Chemical Toxicology 2005; 43(5): 655-661.
(8) CHAOUACHI K. eLetter to the Editor: Syria, Lebanon, Tobacco Research in General and Narghile (Hookah, Shisha) Smoking in Particular . Tobacco Control 2006 (8 June). A critical analysis of the following study: Ward KD, Eissenberg T, Rastam S, Asfar T,Mzayek F, Fouad MF, Hammal F,Mock J, Maziak W. The tobacco epidemic in Syria . Tobacco Control 2006;15;24-29.
http://tc.bmjjournals.com/cgi/eletters/15/suppl_1/i24
(9) ZIELINSKI S. Smoking Machine Test Inadequate and Confusing, But No Replacement a Decade Later . Journal of the National Cancer Institute 2005 (Jan 5); 97 (1): 10-1.
(10) RAKOWER J, FATAL B (1962 Mar) . Study of Narghile Smoking in Relation to Cancer of the Lung .Br J Cancer; 16:1-6.
(11) HOFFMAN D., RATHKAMP G., WYNDER EL (1963) . Comparison of the yields of several selected components in the smoke from different tobacco products. Journal of the National Cancer Institute; 31:627-635.
(12) HOFFMANN D, DJORDJEVIC MV, HOFFMANN I. The changing cigarette. Prev Med 1997 (Jul-Aug);26(4):427-34.
(13) SAID Edward (book). Orientalism. Routledge & Kegan Paul 1978 (London).
(14) CHAOUACHI K. Culture matérielle et orientalisme. L’exemple d’une recherche socio-anthropologique sur le narguilé . Arabica, tome LIII,2, 177-209. Koninklijke Brill NV (Leiden) 2006. [Engl.: Material Culture and Orientalism. The Example of a Socio-Anthropological Research on Narghile ]( www.brill.nl )(available here or contact author)
(15) WORLD HEALTH ORGANISATION. Advisory Note: Waterpipe Tobacco Smoking: Health Effects, Research Needs and Recommended Actions by Regulators . Tobacco Free Initiative 2005. Retrieved 15 Dec. 2005 from: www.who.int/tobacco/global_interaction/tobreg/en/  Full critique available.
(16) COURRIER INTERNATIONAL 2003 (6 Nov.); 679. « Monde musulman : les femmes s’affirment »[ Engl. : Moslem World : How Women Do Assert Themselves ]
www.courrierinternational.com/hebdo/sommaire.asp?obj_id=159
(17) TAMIM H, AKKARY G, EL-ZEIN A, EL-ROUEIHEB Z, EL-CHEMALY S. Exposure of pre-school children to passive cigarette and narghile smoke in Beirut. European Journal of Public Health 2006 (May 4): 4 pages.
http://eurpub.oxfordjournals.org/cgi/content/abstract/ckl043v1  ÂÂ
(18) KANDELA P. Nargile smoking keeps Arabs in Wonderland . The Lancet 2000; 356 (9236): 1175.
(19) RASTAM S, WARD KD, EISSENBERG T, MAZIAK W. Estimating the beginning of the waterpipe epidemic in Syria. BMC Public Health 2004; 4:32.
(20) CHAOUACHI K. Tabacologie du narguilé [Eng.: Tobaccology of Narghile ]. Alcoologie . 1999; 21 (1/83):88-9.
(21) CHAOUACHI K. Le narguilé. Anthropologie d’un mode d’usage de drogues douces [Eng.: An Anthropology of Narghile: its Use and Soft Drugs ], Paris, L'Harmattan, 262 pages.
ÂÂ
Conflict of Interest:
None declared