




Sir, Mikulicz's disease (MD) represents a unique condition involving symmetrical enlargement of the lacrimal and salivary glands, the cause of which is unknown. It has been included within the diagnostic criteria for primary Sjögren's syndrome (SS) due to their histological resemblance [1]. However, it is clear that the pathogenesis of MD differs from that of SS because an elevated serum IgG4 concentration and infiltration of abundant plasmacytes with IgG4 into the lacrimal and salivary glands are seen in MD patients [2]. Clinically, MD exhibits good responsiveness to glucocorticoids, showing improvements in not only lacrimal and salivary gland swelling but also secretion. We attempted to objectively document this phenomenon and to serologically evaluate steroid efficacy.
Analyses were performed in eight MD patients (two men, six women) who consulted doctors at Sapporo Medical University between April 1997 and January 2005. MD was diagnosed according to the following criteria: (i) persistent (more than 3 months) symmetrical swelling of more than two lacrimal and major salivary glands; (ii) prominent mononuclear infiltration of lacrimal and salivary glands; and (iii) exclusion of other diseases that exhibit glandular swelling, such as sarcoidosis or lymphoproliferative disease [2]. Lacrimal gland function was evaluated by Schirmer's test, and salivary gland function was examined by Saxon's test. IgG subclass was measured by nephelometry. These tests were performed before and after treatment. Mann–Whitney's U-test was used for data comparison, and values of P<0.05 were considered statistically significant.
After prescription of 30–40 mg prednisolone/day, lacrimal secretion increased from 6.90±0.77 to 15.70±11.56 mm/5 min (P<0.05), and salivary secretion improved from 1.98±1.86 to 3.66±0.77 g/2 min after treatment (P<0.05). Serum IgG concentration decreased from 4270.0±2098.0 to 1440.1±424.7 mg/dl (P<0.005). Serum levels of each IgG subclass decreased as follows: IgG1, from 1632.9±781.1 to 681.0±227.5 mg/dl (P<0.005); IgG4, from 1556.4±937.1 to 234.7±75.3 mg/dl (P<0.005). IgG subclass/total IgG ratio also changed, as follows: IgG1, from 38.26±3.92 to 46.83±3.98% (P<0.01); IgG4, from 34.85±7.87 to 16.67±5.88% (P<0.005) (Fig. 1).
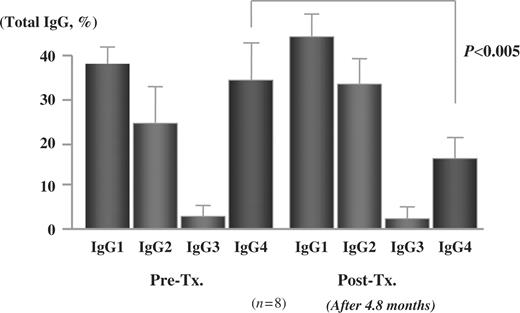
Changes in the ratio of each serum IgG subclass to total IgG after steroid therapy in Mikulicz's disease. Ratio of serum IgG4 was significantly decreased after corticosteroid administration.
Glucocorticoids have long been known to effectively improve lacrimal and salivary gland swelling in MD. However, we noted that sicca symptoms were improved when we followed MD patients being treated with steroids. The present results confirmed a tendency for improvement in lacrimal and salivary secretion 2–3 months from the start of steroid treatment in MD. On the other hand, in SS, steroid therapy makes the lacrimal and salivary glands smaller, but is not able to improve gland secretion. SS is an autoimmune disease that mainly destroys glands. We initially hypothesized that steroids are not effective in SS because it is diagnosed after some degree of progression, while steroids are effective in MD because it is diagnosed earlier (onset of changes in facial appearance). However, our MD cases suffered from dryness for several years, and yet gland function improved after glucocorticoid administration. Tsubota reported fewer apoptotic cells in the lacrimal glands in MD when compared with SS [3], and we observed this phenomenon in salivary glands in MD [4]. The low number of apoptotic cells is thought to be related to the reversibility of gland secretion in MD.
The present analysis proves that different approaches to secretory function are necessary for MD and SS. In SS, cevimeline hydrochloride stimulates the remaining gland function and promotes secretion; however, active steroid treatment is of particular value in MD because glandular destruction has not occurred.
One of the serological characteristics of MD is an elevated concentration of IgG4. In addition, the ratio of serum IgG4 to total IgG is 34.85%, while in healthy controls the ratio is about 4%. It is known that the ratio does not vary with race, sex or age after adulthood. We found that the serum IgG4/total IgG ratio decreased significantly in MD patients after steroid therapy, although it is expected that steroids would decrease IgG4 concentration as a result of immune suppression. This phenomenon may be related to disease activity and the subsequent improvement in symptoms. However, in our MD cases the serum IgG4/total IgG ratio failed to normalize, and increased after tapering or interrupting the steroid dose (<5 mg prednisolone/day). We believe that 5–7.5 mg prednisolone/day is necessary to maintain disease suppression.
The authors have declared no conflicts of interest.
References
Morgan WS, Castleman B. A clinicopathologic study of Mikulicz's disease.
Yamamoto M, Harada S, Ohara M et al. Clinical and pathological differences between Mikulicz's disease and Sjögren's syndrome.
Tsubota K, Fujita H, Tsuzaka K, Takeuchi T. Mikulicz's disease and Sjögren's syndrome.
Author notes
First Department of Internal Medicine, Sapporo Medical University, School of Medicine and 1Sapporo Medical University, Sapporo, Hokkaido, Japan

{kind=link}
Comments