Article Text

Abstract
Objective To compare the efficacy of oral sweet solutions to water or no treatment in infants aged 1–12 months during immunisation.
Methods Randomised controlled trials (RCTs) were retrieved through internet searches or manual searches of reference lists. Search terms included newborn, infant, pain, sucrose and alternative names for sweet solutions. Summary estimates with 95% CIs were calculated and included relative risk (RR), risk difference (RD) and number needed to treat to benefit (NNTB) for dichotomous outcomes, and weighted mean differences (WMD) for continuous outcomes. Where pooling of results was not possible, a narrative summary of study results is presented.
Results Of the 695 studies identified, 14 RCTs with 1674 injections met the inclusion criteria. Sucrose or glucose, compared to water or no treatment decreased crying during or following immunisation in 13 of the 14 studies. Infants receiving 30% glucose (three trials, 243 infants) had a decreased RR in crying incidence following immunisation (typical RR 0.80, 95% CI 0.69 to 0.93; RD −0.17, 95% CI −0.29 to −0.05; NNTB 6, 95% CI 3 to 20). With sucrose or glucose, there was a 10% WMD reduction in proportion of crying time (95% CI −18 to −2) and a 12 s reduction in crying duration (95% CI −23 to −0.7 s). An optimal dose of sucrose or glucose could not be ascertained due to the varied volumes and concentrations used.
Conclusion Infants aged 1–12 months administered sucrose or glucose before immunisation had moderately reduced incidence and duration of crying. Healthcare professionals should consider using sucrose or glucose before and during immunisation.
Statistics from Altmetric.com
Background
Extensive research shows that oral sucrose, glucose and other sweet tasting solutions are effective analgesics during minor painful procedures in neonates.1 2 The administration of sweet solutions (in particular sucrose and glucose) is now widely recommended for routine use prior to painful procedures in newborn infants.3,–,7 Although the analgesic effect of sucrose and glucose on newborns is well established, little is known about whether these solutions or other sweet tasting solutions are effective in reducing procedural pain in infants beyond the newborn period. This gap in knowledge was the subject of a recent narrative literature review of 10 published randomised controlled trials (RCTs) in which conflicting results across studies were highlighted.8 A systematic review and meta-analyses were recommended to ascertain whether current evidence supports the use of sweet solutions for pain management beyond the neonatal period. Therefore, the aim of our study was to conduct a systematic review and meta-analyses on the effectiveness of sweet solutions during painful procedures for infants beyond the neonatal period up to 12 months of age.
What is already known on this topic
There is abundant high quality evidence of the analgesic efficacy of sucrose and glucose in newborn infants, especially during heel lance and venepuncture.
There are a growing number of studies evaluating the analgesic effects of sweet solutions in infants beyond the newborn period.
What this study adds
Sucrose and glucose also reduce pain during immunisation in infants up to 12 months of age.
The analgesic effects of sweet solutions in older infants are more moderate than those seen in newborn infants.
Methods
Ethics approval
As this was a systematic review of RCTs already completed, with no research activities involving humans, there was no requirement for ethics committee approval.
Sources of data
We followed the methods for conduct of systematic reviews as outlined by the Cochrane Collaboration.9 Electronic databases searched were MEDLINE (1950–March 2009), Embase (1980–March 2009), CINAHL (1982–March 2009), PsycINFO (1967–March 2009) and all EBM Reviews. Search terms were newborn, infant, neonate, sucrose and pain with appropriate truncation symbols. To expand the search to include sugar solutions in addition to sucrose, we also included the following search terms: lactose, glucose, fructose, glycerine, dextrose, aspartame, polycose, saccharose and saccharide. Language restrictions were not imposed. Reference lists from articles retrieved for the review were searched, as were personal files and recent major paediatric or paediatric pain conference proceedings for further relevant trials. For studies including both neonates and infants beyond the neonatal period, we extracted data for the subgroup of infants of interest if possible or we contacted authors for additional information. When means and SDs were not reported, we attempted to obtain information from the authors.
Study selection
RCTs of sucrose, glucose or other sweet solutions administered orally during immunisations in infants beyond the neonatal period (corrected for post menstrual age at birth) to 12 months of age were included.
Critical appraisal technique
Methodological quality was assessed using the standard methods of the Cochrane Collaboration. With a six-point quality rating scale, we evaluated potential biases according to the following criteria: randomisation generation; concealment of allocation; blinding of intervention; incomplete outcome data reported; selective outcome reporting; other sources of bias.9 Two raters (DH, MB) independently assessed the methodological quality of each study and any disagreements were resolved through consensus or arbitration by a third rater (JY).
Methods for synthesising findings
Two authors (DH, MB) independently extracted data on study design, sample, intervention and outcomes (cry behaviours, validated pain scales, physiological indicators) including raw data for the meta-analyses. When appropriate comparable data were available (eg, means, SDs, proportions) from at least two trials, we conducted a meta-analysis.
Statistical analysis
Review Manager 5.0 (RevMan) software was used for the meta-analysis of outcome data.10 When pooling binary outcomes, we used the relative risk ratio (RR) and its 95% CI. If the RR was significant, the risk difference (RD) and number needed to treat to benefit (NNTB) were computed. Weighted mean difference (WMD) and its 95% CI were calculated for continuous outcomes and heterogeneity was measured using the I-squared (I2) test. All data were combined using the random effects model. For studies where pooling of results was not possible, we present a narrative descriptive summary account of study results.
Results
The search yielded 695 citations, of which 14 RCTs, including a total of 1674 injections, met the inclusion criteria.11,–,24 The selection process is summarised in figure 1. Details including the demographic characteristics of the 14 included RCTs are presented in table 1 and a summary of the quality ratings of the studies are presented in table 2. Immunisation and sweet solution details are summarised in online appendix A. Authors of included trials provided additional data for three studies.11 13 20

Flow chart for selection of eligible studies.
Characteristics of randomised controlled trials meeting inclusion criteria
Quality assessment of randomised controlled trials
The 14 studies were all RCTs and generally of high quality. Five studies did not describe the generation of allocation sequence,11,–,13 18 23 but only two studies failed to report concealment of allocation.12 23 Knowledge of allocated intervention was adequately prevented in most studies, with the exception of two RCTs, in which outcome assessments were adequately blinded, but parents as well as the nurses administering injections were not blinded.22 24 The glucose solution could not be concealed in one study that compared two different sucrose concentrations, a 40% glucose solution and water.21 Incomplete outcome data were inadequately addressed in only one longitudinal RCT in which data were missing for five infants at the second data collection point.14 Three studies were considered to have other problems increasing the risk of bias: one had small sample sizes of subgroups of infants included in this review,13 pacifier use differed between the groups in another study,16 and in a third study, insufficient information was given concerning collection of data about infants' like or dislike of the solution, but the outcome suggests a possible lack of blinding23 (table 2).
Characteristics and results of included studies
All identified trials used sucrose or glucose of various concentrations; no studies using other sweet tasting solutions were identified. With the exception of one study,20 sucrose or glucose in different doses and concentrations reduced various behavioural pain indicators, including crying characteristics, and composite pain scores, during or following completion of immunisation compared to either placebo (water) or no treatment. In one of the studies in which a 12% sucrose solution was used, the effects were only evident during a single immunisation, and ineffective for the second and third injections.11 No studies reported adverse events.
Ten studies used sucrose solutions in concentrations ranging from 12% to 75%.11,–,16 19 20 22 23 In three studies, 30% glucose was utilised17 18 24 and in one study, the analgesic effects of two sucrose concentrations (25% and 50%) and 40% glucose were compared with water.21 Volumes of solutions given were mainly 2 ml or less, with the exception of one study where 10 ml of 25% sucrose was administered.22 In one study, a combination of 30% glucose and EMLA was compared to a placebo oral solution and a topical cream, 17 and another study compared non-nutritive sucking (NNS) with glucose.18
A variety of pain outcomes were used as shown in table 1. Various crying characteristics were measured in all but two studies.18 20 Four composite pain assessment tools were used and three studies included four different visual analogue scales.16 17 22 Physiological responses were assessed as outcome measures in three studies,17 19 22 including heart rate, heart rate changes from baseline, or heart rate variability (HRV). Salivary cortisol measurements of both infants and parents were measured in one study.17
Efficacy of sucrose and glucose
Administration of either sucrose or glucose resulted in reduced crying incidence and duration and composite pain scores, compared to either placebo (water) or no treatment in 13 of the 14 studies (table 3). In one study, 2 ml of 12% sucrose had no effect on pain scores,20 and in another, although sucrose was more effective compared to no treatment during a single injection, no differences in crying time between infants receiving 12% sucrose compared to water were demonstrated.11 The more concentrated 50% sucrose solution was more effective than 25% sucrose, 40% glucose and water in reducing crying time following immunisation.21 As these latter results were reported in medians and interquartile ranges (IQRs), we could not combine data from this study using meta-analytic techniques.
Results
Neither sucrose nor glucose, including glucose combined with EMLA, resulted in significant reductions in mean heart rate, mean heart rate change from baseline, or mean HRV.17 19 22 The study measuring salivary cortisol following immunisation showed that infants who received combined glucose and NNS had a 33% mean reduction in salivary cortisol levels from baseline, while infants receiving water with and without pacifier, or oral glucose alone, had an increase in salivary cortisol levels following immunisation.18
Meta-analyses could be performed for three cry outcomes following immunisation: (1) proportion of cry; (2) duration of cry (s) until crying cessation; and (3) incidence of cry. For proportion of crying times following immunisation, data were pooled from three studies and included 150 infants.12 18 19 Barr et al12 used three doses of 0.25 ml of 50% sucrose, Mowery19 used 2 ml of 50% sucrose and Morelius et al25 used 2 ml of 30% glucose. Results showed a 10% mean reduction in proportion of crying time following immunisation in the sweet solutions groups compared to placebo (WMD −10, 95% CI –18 to −2%) (figure 2).

Weighted mean difference for cry proportion following immunisation (%).
Data were pooled for crying duration (s) from six studies (five using sucrose and one using glucose) (N=716 injections).11 13 16 17 19 20 23 Results showed a non-significant mean reduction in crying duration of 16 s in the sweet solutions group (95% CI −32 to 0.08; p=0.05) (figure 3A). Due to a high degree of heterogeneity (I2=88%), we repeated the meta-analysis without the two studies which used a 12% sucrose solution,11 13 as the results of these two studies differed widely. When we removed these two studies from the meta-analysis, the I2 value was reduced from 88% to 72%. The results then showed a statistically significant, but clinically small WMD of –12 s in crying duration (s), favouring sweet solutions (95% CI −23 to −0.78; p=0.04) (four studies, 568 injections) (figure 3B). We performed a subgroup analysis to further explore conflicting results in the two studies which used 12% sucrose. As Dilli et al13 included infants 6–12 months old, and the control group received standard care only with no oral placebo, we included a subgroup of infants in the study by Allen et al11 matched on age and treatment in the meta-analysis. Results showed that 12% sucrose was effective for reducing cry duration (WMD –48, 95% CI –71 to −24; p<0.0001); however, there was significant heterogeneity between these two studies (I2=93%) and the total sample size was only 62 infants (figure 4).

(A) Weighted mean cry duration following immunisation (s). (B) Weighted mean cry duration following immunisation (s) following removal of two randomised controlled trials of 12% sucrose.

Weighted mean differences for cry duration (s) following immunisation. Only the two studies using 12% sucrose versus control (no placebo) are included. The subgroup of infants only included those aged 6–12 months.
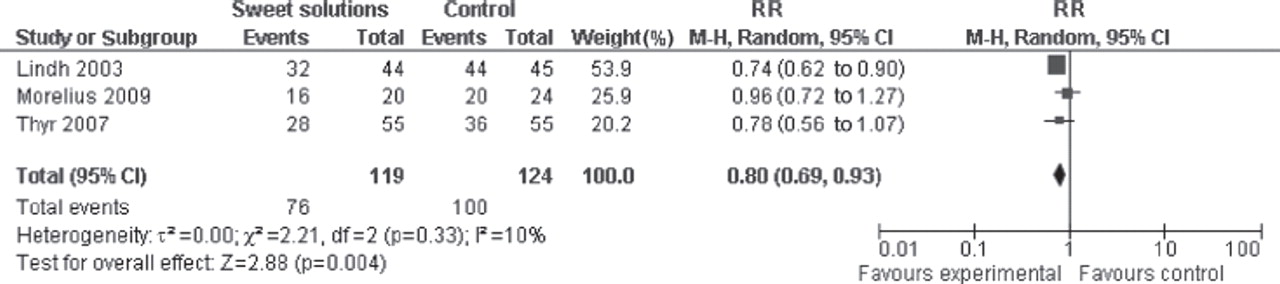
A meta-analysis was conducted with data pooled from three studies reporting incidence of cry following immunisation17 18 24 (N=243 infants). Results showed a 20% reduction in RR for crying for infants when administered 1–2 ml of 30% glucose (RR 0.80, 95% CI 0.69 to 0.93) (figure 5). There was no significant heterogeneity (I2=10%). RD was −0.17 (95% CI −0.29 to −0.05) and NNTB was 6 (95% CI 3 to 20).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Typical relative risks (or risk ratios) (RRs with 95% CIs) for crying incidence following immunisation. All studies used 30% glucose.
Due to inconsistencies in the volumes and concentrations of sucrose and glucose that were reported to be effective, an optimal analgesic dose of either sweet solution to be used in infants beyond the neonatal period during immunisation could not be determined.
Discussion
To our knowledge, this is the first systematic review and meta-analyses conducted to explore the analgesic effects of sweet solutions in infants beyond the newborn period up to 12 months of age. Only studies investigating the effect of sucrose and glucose were identified. In general, the quality of the studies was high. We found that oral administration of either sucrose or glucose was associated with small but statistically significant reductions in crying incidence, crying duration and composite pain scores during and following immunisation. These results extend the findings of the systematic review and meta-analyses of sucrose in newborn infants, which reported that effective doses for neonates ranged between 0.05 ml and 2 ml of 24% sucrose.1
For infants beyond the neonatal period up to 12 months, higher concentrations of either sucrose or glucose seemed to be more effective. This was highlighted in the study by Lewindon et al,16 in which a 75% sucrose solution was used following a pilot study where 50% sucrose was considered ineffective. Conversely, in a recently published study, 12% sucrose significantly reduced pain scores and crying time compared to no treatment, in all groups of infants, including the subgroup of 20 infants aged 6–12 months included in this systematic review.13 Previous to this study, 12% sucrose was considered insufficiently sweet to exert an analgesic effect,11 and more recently, Poulsen also showed no analgesic effect of 12% sucrose during immunisation.20 The reasons for the conflicting results of the studies using 12% sucrose during immunisation are inexplicable; however, they may be related to the additional physical interventions used (ie, maternal holding and distraction offered by the majority of mothers in the study by Dilli et al13) or possibly by unknown cultural or contextual differences. Such differences could potentially be related to different responses to sweet taste. As the procedure of sucrose administration in the Dilli et al study13 was based on that used by Allen et al,11 this cannot explain the different responses.
There are important differences in the efficacy of sweet solutions in older infants compared to newborn infants. In most studies, the analgesic effects were more moderate than previously reported for newborn infants1 and pain reduction was primarily evident in the period immediately following completion of the procedure, rather than during the procedure.12 In addition to the included studies of sucrose or glucose during immunisation, two studies including infants beyond the neonatal period up to 12 months of age were conducted in sick infants presenting to emergency departments.26 27 The analgesic effects of 2 ml of 44% sucrose during venepuncture26 and 2 ml of 24% sucrose during urethral catheterisation were studied.27 In both studies, sucrose was more effective than water in reducing pain scores and crying duration only in the youngest groups of infants. These two studies warrant further discussion. Firstly, these two procedures may be associated with higher pain intensity, cause more stress and require more restraint than intramuscular injections, rendering sucrose, a mild analgesic, insufficient for pain relief. Secondly, in these two RCTs, single doses of 2 ml of 24% sucrose27 and 2 ml of 44% sucrose,26 respectively, were administered 2 min prior to commencement of the procedure. This practice is widely accepted, based on studies conducted by Blass et al, where sweet taste mediated analgesic effects peaked at 2 min and lasted for between 3 and 5 min, an interval considered to coincide with endogenous opioid release.28 29 However, as both urethral catheterisation and venepuncture generally take longer to perform than immunisations, the analgesic effects of sweet solutions may not have been sustained in these studies. A shorter effect time of sweet solutions in older infants was demonstrated in a study where 24% sucrose was effective for 1 min only.30 In both studies conducted in the emergency department, subgroup analyses showed that sucrose was more effective than placebo in the youngest group of infants only.26 27 In a longitudinal study of sucrose effectiveness over the course of a prolonged hospitalisation, sucrose given in aliquots prior to, upon commencement of, and during heel lancing continued to provide analgesia in infants aged 1–5 months throughout the period of hospitalisation.31 Therefore, dividing the dose and administering repeated small volumes throughout the procedure may optimise sustained analgesic effects for those procedures in older infants lasting more than a few minutes.31,–,33 Further studies in infants beyond the neonatal period, comparing a single dose of sweet solution to divided doses given over the duration of a prolonged procedure are needed.
As combined strategies were used in two studies,17 22 the effects of sweet solutions alone could not be isolated. A combination of topical anaesthetic cream and oral glucose was compared to water and topical placebo cream in one study17 and a combination of 10 ml of 25% sucrose, NNS and parental holding was compared to standard care (infants were vaccinated while lying on the examination table with no specific comfort measures provided).22 These combinations of strategies are dissimilar to the administration of small volumes of sweet solutions alone; therefore, results need to be interpreted with caution.
Widely varying concentrations and volumes of sucrose and glucose were used in studies included in this review. Two studies used 2 ml of a 75% sucrose solution,16 23 and a larger volume of 10 ml of 25% sucrose was used in another.22 Both the 10 ml volume of 25% sucrose and the undiluted 75% sucrose concentration exceed the total sucrose dose administered in most other studies and far exceed the 0.24–0.50 g sucrose dose recommended for effective pain management in term newborn infants.1 Although Reis et al22 did not justify using 10 ml of sucrose, Lewindon et al16 reported that a 50% sucrose solution used in a pilot study failed to demonstrate any observable effects, and Soriano and Gomez23 stated they used the same sucrose concentration as Lewindon et al. These results, along with results of animal studies28 and those reported in a study comparing three different concentrations of sweet solutions (25% and 50% sucrose and 40% glucose),34 highlight that, in older infants, there is evidence of a sweet-dose related response, with more concentrated sugar solutions being more effective. However, as previously stated, the results obtained by Dilli et al,13 where 12% sucrose was effective in reducing immunisation pain not only for infants but also for children up to 4 years of age, are contrary to this evidence.
For the four studies which used glucose solutions,17 18 21 24 glucose effectively reduced pain during immunisation compared to water, highlighting that non-sucrose sweet solutions of sufficient concentration are analgesic. Administration of 30% oral glucose resulted in an RR for crying following immunisation of 0.80 and an NNTB of six infants (albeit with a wide CI of 3 to 20). However, Ramenghi et al21 demonstrated that a sweetness dose response exists in this age group as the concentrated 50% sucrose solution was more effective than both 40% glucose and 25% sucrose. Although sucrose is the sweetest of the sugars (sucrose>fructose>glucose>lactose),35 either sucrose or glucose could be used depending on availability and organisational preference as long as the solutions are sufficiently sweet (ie, at least 30% glucose or 24% sucrose1).
Limitations
The wide variety of concentrations of sucrose or glucose solutions used, outcome measures and differences in the timing of outcome assessments precluded inclusion of most studies in meta-analyses. Four different composite pain assessment tools were used, three of which have undergone various degrees of validity and reliability testing in infants,36,–,39 with the exception of the Oucher, which has only been validated for use in children aged 3–7 years.40 41 The four pain assessment tools have varied scales and maximum scores of 5,37 7,36 10 and 100.40 Such variations in scales pose difficulties in conducting appropriate meta-analyses.
In addition, in this review, we did not consider varying pain responses to the type of immunisation administered, the order of immunisations performed or injection techniques, all of which have been shown to impact on pain during immunisation.42 43
Implications for practice
Based on extensive evidence of the efficacy of sweet solutions in neonates1 and the evidence from this systematic review, sucrose or glucose along with other recommended physical or psychological pain reduction strategies, such as NNS, breast feeding or effective means of distraction,44 should be consistently utilised for immunisation. For multiple immunisations, the total dose of sweet solution should be given prior to and throughout the procedure to ensure sustained effects of sweet tasting analgesia. Further studies are warranted comparing different concentrations of sucrose and glucose and the use of single dosing 2 min prior to painful procedures to multiple dosing over the course of procedures. In addition, sucrose or glucose, depending on the availability of solutions, should be considered for other painful procedures for infants up to 12 months of age. This information is important for healthcare professionals working with infants in both inpatient and outpatient settings, as sweet solutions are readily available, have a very short onset of time to analgesia, are inexpensive and are easy to administer.
Conclusion
Sucrose and glucose of various doses and concentrations moderately reduces crying incidence, crying duration and pain scores during or following immunisation, beyond the neonatal period up to 12 months of age. Healthcare professionals responsible for administering immunisations should consider using sucrose or glucose during painful procedures.
Acknowledgments
We thank all members of the CIHR Systematic Review of Sweet Solutions for Acute Pain Relief in Infants, Knowledge Synthesis Team. Also, Dr Keith Allen, Dr Dilek Dilli and Ms Poulsen are acknowledged for providing additional unpublished data. We also thank Sobia Khan for her assistance with the review.
References
Footnotes
-
Funding The first author, Denise Harrison was supported by The Pain in Child Health Strategic Training Initiative (STP53885) and CIHR Team Grant in Children's Pain (CTP-79854 and MOP-86605) while undertaking this review. Canadian Institutes of Health Research (CIHR) Knowledge Synthesis Grant Funding (reference number: KRS91774) financially supported this review.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.