Article Text

Abstract
Background Non-invasive ventilation is sometimes unable to provide the respiratory needs of very premature infants in the delivery room. While airway obstruction is thought to be the main problem, the site of obstruction is unknown. We investigated whether closure of the larynx and epiglottis is a major site of airway obstruction.
Methods We used phase contrast X-ray imaging to visualise laryngeal function in spontaneously breathing premature rabbits immediately after birth and at approximately 1 hour after birth. Non-invasive respiratory support was applied via a facemask and images were analysed to determine the percentage of the time the glottis and the epiglottis were open.
Hypothesis Immediately after birth, the larynx is predominantly closed, only opening briefly during a breath, making non-invasive intermittent positive pressure ventilation (iPPV) ineffective, whereas after lung aeration, the larynx is predominantly open allowing non-invasive iPPV to ventilate the lung.
Results The larynx and epiglottis were predominantly closed (open 25.5%±1.1% and 17.1%±1.6% of the time, respectively) in pups with unaerated lungs and unstable breathing patterns immediately after birth. In contrast, the larynx and the epiglottis were mostly open (90.5%±1.9% and 72.3%±2.3% of the time, respectively) in pups with aerated lungs and stable breathing patterns irrespective of time after birth.
Conclusion Laryngeal closure impedes non-invasive iPPV at birth and may reduce the effectiveness of non-invasive respiratory support in premature infants immediately after birth.
- larynx
- preterm newborn
- Non-invasive ventilation
- apnoea
- glottis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Non-invasive ventilation often fails to provide adequate respiratory support to premature newborns at birth; however, the reason for this is unknown.
Little is known about laryngeal function at birth in term or preterm newborns.
What this study adds?
We have used phase contrast X-ray imaging to show that the glottis and epiglottis are predominantly closed immediately after birth in apnoeic premature rabbits.
When the glottis and epiglottis were closed, non-invasive iPPV was ineffective, unless the pup took a breath.
The glottis and epiglottis were predominantly open following lung aeration and the establishment of stable breathing pattern, allowing for successful non-invasive ventilation.
Introduction
Until recently, most very premature infants requiring respiratory support at birth were intubated and mechanically ventilated. However, as mechanical ventilation increases the risk of lung injury,1 clinical practice has shifted towards non-invasive respiratory support2 usually administered via a facemask.3 4 However, little information is available on how non-invasive respiratory support interacts with the infant’s changing physiology at birth and as such, it is unclear why it is sometimes ineffective at birth.4–6
Airway obstruction and mask leak are common reasons why non-invasive intermittent positive pressure ventilation (iPPV) is sometimes unsuccessful. While mask leak is more common (51%), airway obstruction (26%) increases the rate of clinical deterioration and need for intubation.7 8 Although the mechanisms and site of airway obstruction are unclear, incorrect facemask or head positioning are thought to be major causes.7 8 However, when preterm infants are given a sustained inflation at birth, air only enters the lung if the infant takes a breath, indicating that the larynx maybe involved.9
In the fetus, tonic laryngeal adductor muscle activity closes the glottis during apnoea to seal the airway,10 whereas during fetal breathing movements (FBM), this activity is absent and dilator activity occurs in phase with diaphragmatic contractions.10 In the fetus, as laryngeal adduction restricts liquid efflux during apnoea, it helps to maintain lung expansion, which is the primary stimulus for lung growth.11 12 We propose that laryngeal adduction in apnoeic very preterm infants persists after birth and will prevent non-invasive iPPV from ventilating the lung unless the infant takes a breath. Furthermore, as the lung aerates and regular breathing commences, we propose that the larynx will remain open, allowing non-invasive iPPV to ventilate the lung.
We examined laryngeal activity in premature rabbits immediately after birth using phase-contrast (PC) X-ray imaging.13 Using this technique, closure or patency of the airway within the larynx is visible (figure 1), allowing determination of whether it is open or closed. During the analysis, we found that we were also able to visualise the epiglottis, allowing us to measure opening times for the epiglottis as well. We hypothesised that, immediately after birth, the larynx would be predominately closed, only opening during spontaneous breaths, which prevents non-invasive iPPV from inflating the lung. We also hypothesised that the larynx would be predominantly open following the onset of stable breathing, allowing the lung to be ventilated non-invasively.

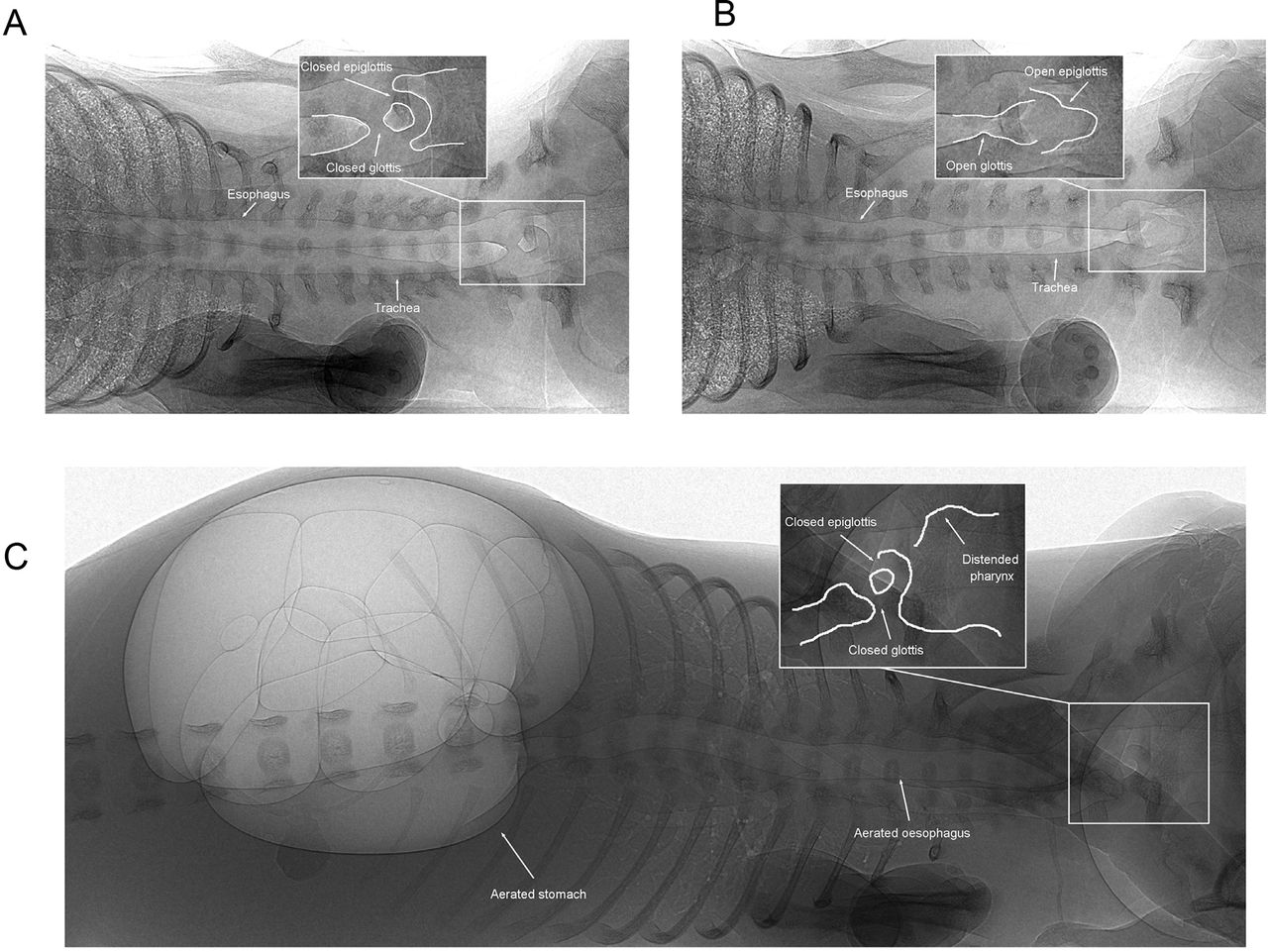
Phase-contrast X-ray images of a spontaneously breathing newborn preterm rabbit pup with (A) a closed glottis and epiglottis and (B) an open glottis and epiglottis; the inserts are magnifications of the regions shown within the white boxes. (C) Air accumulation in the stomach of a rabbit pup that did not have an oesophageal tube and received CPAP levels >7 cmH2O while the larynx was closed. CPAP, continuous positive airway pressure.
Methods
Experimental procedure
All experimental procedures received approval from SPring-8 Animal Care and Monash University’s School of Biomedical Science’s Animal Ethics Committees. Experiments were conducted at the SPring-8 synchrotron in Japan.
At 29-day gestational age (GA) (term=32 days), pregnant New Zealand white rabbits (n=21) were anaesthetised (Rapinovet; intravenous; 12 mg/kg bolus), intubated and anaesthesia sustained with isoflurane inhalation (1.5%–3.0%). Pups were exteriorised by caesarean section and a custom-made facemask was placed over the pup’s head and attached using tissue glue. An oesophageal tube was inserted to measure intrathoracic pressure and caffeine was administered (20 mg/kg base; intraperitoneal). Pups were delivered, transferred into the imaging hutch and placed on a heating pad and ECG leads attached. The facemask was connected to a ventilator14 to give 5–7 cmH2O of continuous positive airway pressure (CPAP). Pups were physically stimulated to encourage spontaneous breathing and were imaged for approximately 15 min. Facemask and oesophageal pressures were recorded (Powerlab; ADInstruments, Sydney, Australia). If the pup was apnoeic and heart rates were <100 beats per minute, the hutch was entered to deliver tactile stimulation; this was common as most pups had unstable breathing patterns immediately after birth. To determine whether non-invasive iPPV could inflate the lung, a peak inflation pressure (PIP) of 25 cmH2O and a positive end-expiratory pressure (PEEP) of 5 cmH2O were used.14 Following imaging, pups were removed from the hutch, placed on a heat pad and received constant tactile stimulation to sustain spontaneous breathing. If pups were unable to sustain a stable respiratory pattern they were killed with sodium pentobarbitone (intraperitoneal 100 mg/kg; Somnopentyl, Kyoritsu Seiyaku Co., Tokyo, Japan). At approximately 1 hour after birth, viable pups were re-imaged and during this second sequence, each pup received a brief period of iPPV (PIP 25 cmH2O and PEEP 5 cmH2O) and stepwise increases in CPAP between 0 and 15 cmH2O.
PC X-ray imaging
High-resolution PC X-ray imaging was used to visualise the larynx15 using an ORCA Flash 4.0 Hamamatsu C11440-22C (effective pixel size 15.3 µm, 2048×2048 pixels) located 2 m downstream of the pups.16 17
Data analysis
Imaging was used to determine whether the glottis and epiglottis were open or closed immediately after birth and at approximately 1 hour after birth. Data are expressed as the percentage of time the glottis and epiglottis were open over consecutive 30 s periods. The ability of iPPV to ventilate the lung was assessed using images of the lung and intrathoracic oesophageal pressures, before and after lung aeration and establishment of a stable breathing pattern. The effect of increasing mask pressure on spontaneous breathing was assessed using respiratory rates from oesophageal pressure recordings (figure 3,4). The effect of airway pressures on distension of the pharynx was measured from the images using ImageJ (National Institute of Health, Bethesda, Maryland, USA) and expressed as a percentage of the initial pharyngeal dimension prior to iPPV. As the entire pharynx was not included in the image field of view, we were unable to assess pharyngeal dimensions in detail.
Statistical analysis
All data are presented as the mean ± SEM. Data were compared for significance over time using a two-way repeated-measures analysis of variance. An unpaired t-test with a Welch’s correction was used to test significance between the sequences for both the glottis and the epiglottis. p Values <0.05 were considered statistically significant.
Results
Seventy-one premature pups were delivered from 21 does; 38 were delivered at 29-day GA and 33 at 30-day GA; term is 32-day GA in rabbits. Immediately after birth, 62 pups were imaged, with only 36 (of 62) attaining a sustainable breathing pattern and heart rates >100 beats per minute; 9 pups were non-viable at delivery and were not imaged. Of the 36 pups with a stable breathing pattern, 17 pups remained viable for reimaging at approximately 1 hour after birth. Images of the same pup, initially with a closed glottis and epiglottis (figure 1A) and then with an open glottis and epiglottis (figure 1B) are shown in figure 2. Eleven of the 36 pups were breathing vigorously and were very active after delivery resulting in lung aeration before imaging could commence (figure 1B). These 11 pups were initially analysed separately from pups with unaerated lungs, unstable respiratory activity, apnoeic periods and bradycardias (figure 1A); thereafter all pups were analysed together.

Flow diagram describing the outcome of the preterm rabbit pups with respect to developing a stable or unstable breathing pattern immediately after birth and at approximately 1 hour after birth.
Interpretation of PC X-ray movie sequences
Immediately after birth
Most (51/62) preterm pups had unaerated distal airways (aeration restricted to larger airways; figure 2) and unstable respiratory patterns interspersed with apnoeic periods (figure 3). During these apnoeic periods, the glottis was predominantly closed (online supplementary movie 1) only opening briefly during spontaneous breaths before closing again between breaths. During a breath, the glottis and epiglottis opened and the pharyngeal wall partially collapsed as air flowed into the lungs. This implies that, despite CPAP, upper airway resistance restricted airflow into the pharynx, which acted as a partial reservoir for low resistance gas flow into the lungs during inspiration. Expiration was short in duration and there was no evidence of laryngeal mediated expiratory braking at this stage. Between breaths, the glottis and epiglottis remained mostly closed, but on occasion the glottis was open, while the epiglottis remained closed. At these times, the glottis appeared relaxed and not actively abducted as occurred during inspiration. Between breaths, the pharynx was usually distended due to CPAP, while the glottis and/or epiglottis were closed; this distension mostly increased with increasing CPAP. As the oesophageal tube restricted air entry into the stomach, if it was not present, increasing CPAP and pressurisation of the pharynx caused air to enter the stomach (figure 1C).
Supplementary movie

Intrathoracic oesophageal pressure recordings from preterm rabbit pups displaying (A) an unstable breathing pattern or (B) a stable continuous breathing pattern. Each reduction in pressure represents a breath. Both recordings were obtained within a few minutes of birth. The unstable breathing pattern was characterised by breaths that differed in amplitude, varied in rate and were interspersed with apnoeic periods; these profiles were accompanied with a bradycardia of <100 beats per minute. In contrast, the stable breathing pattern was characterised by regular, continuous breathing that was relatively consistent in amplitude.
After lung aeration
In pups with a stable breathing pattern (figure 3B), the glottis and epiglottis remained predominantly open and did not open and close in phase with respiratory movements (online Supplementary movie 2), although dilation was enhanced during inspiration. The glottis usually narrowed during expiration, perhaps due to a reduction in abductor muscle activity, but remained open throughout the respiratory cycle. Active transient closure of the glottis was commonly seen during expiration (online Supplementary movie 2). These expiratory braking manoeuvres were characterised by rapid expansion of the sub-glottic, upper trachea indicating pressurisation of the airways (online Supplementary movie 2). In the absence of expiratory braking, the pharynx appeared to expand during expiration.
Supplemental material
Non-invasive iPPV
In pups that were apnoeic or had unstable breathing patterns, non-invasive iPPV was unable to ventilate the lung (see below) due to closure of the glottis and/or epiglottis. This prevented air from entering the trachea, causing the pharynx to expand and deflate in phase with the ventilator (figure 4) (online Supplementary movie 3). In contrast, in pups with a stable respiratory pattern, the glottis and epiglottis remained mostly open, allowing non-invasive iPPV to ventilate the lung in 78% of attempts (17 of 22 attempts in 13 pups; figure 5; online Supplementary movie 4). In a small number of pups (4 of 13 pups), non-invasive iPPV caused the glottis and/or epiglottis to close, which only opened briefly during a spontaneous breath out of synchrony with the ventilator (5 of 22 or 22% of iPPV attempts).
Supplemental material
Supplemental material

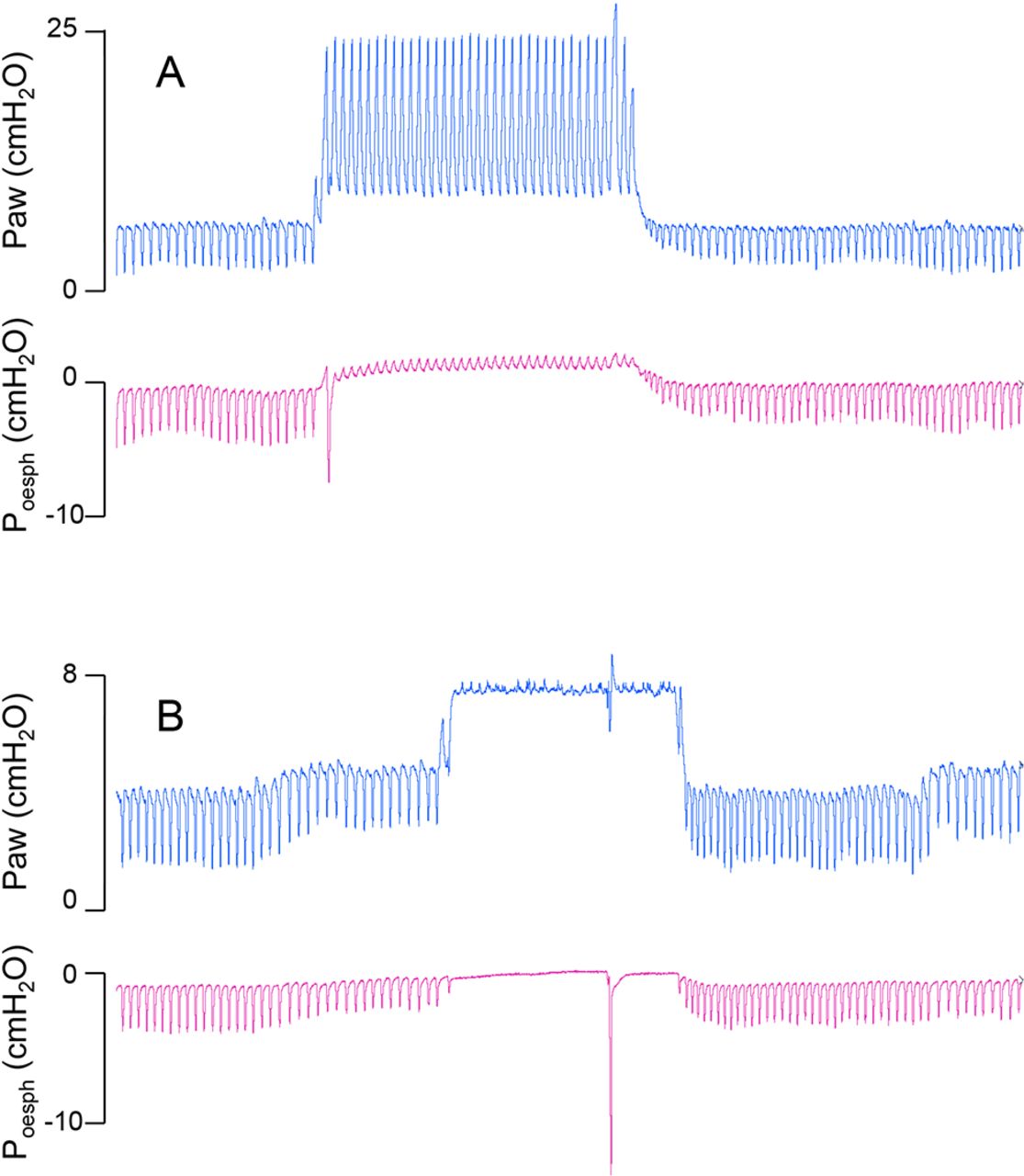
Physiological recordings of airway pressures (P aw) and oesophageal pressures (P oesoph) in preterm rabbit pups that initially had a stable spontaneous breathing pattern. (A) The pup received iPPV using a peak inspiratory pressure of 25 cmH2O and an end-expiratory pressure of 5 cmH2O. Note that the iPPV resulted in positive pressure fluctuations in oesophageal pressure, demonstrating transmission of ventilation pressure into the chest that resulted in lung inflations; lung inflation was confirmed from X-ray imaging. (B) The pup received CPAP that when increased to 8 cmH2O, caused an immediate suppression of spontaneous breathing activity that persisted throughout the elevated CPAP period; only one large deep inspiratory effort was observed. Note that although P aw increased with increased CPAP, oesophageal pressure did not increase, indicating that the pressure was not transmitted into the chest because the larynx was closed. CPAP, continuous positive airway pressure; iPPV, intermittent positive pressure ventilation.

The percentage of time that the glottis (top panel) and epiglottis (bottom panel) were open in preterm rabbit pups measured within minutes of birth (A and C) and at approximately 1 hour after birth (B and D). (A and C) Pups were divided into two groups depending on whether they had a stable (closed circles) or unstable breathing pattern after birth (closed squares; see figure 3).
Image analysis of glottic and epiglottic function
Glottis
In pups (n=51) with unaerated lungs and unstable breathing patterns immediately after birth (figure 3), the glottis was open 25.5%±1.1% of the time (range: 12.0%±3.5%–36.1%±12.5%; figure 6). In contrast, in pups with aerated lungs and a stable respiratory pattern (Figure 3) (n=11), the glottis was open 76.8%±3.7% (range 36.7%±31.8%–99.1%±0.1%; figure 6). After the first hour (second imaging sequence), the glottis was open on average 90.5%±1.9% of the time (range: 80.3%±8.7–99.7%±0.3%, figure 6) and did not significantly vary over time (n=17 pups). Glottic opening times were significantly greater during the second imaging sequence compared with the first imaging sequence in pups with an unstable breathing pattern (p<0.0001), but not in pups with a stable breathing pattern.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
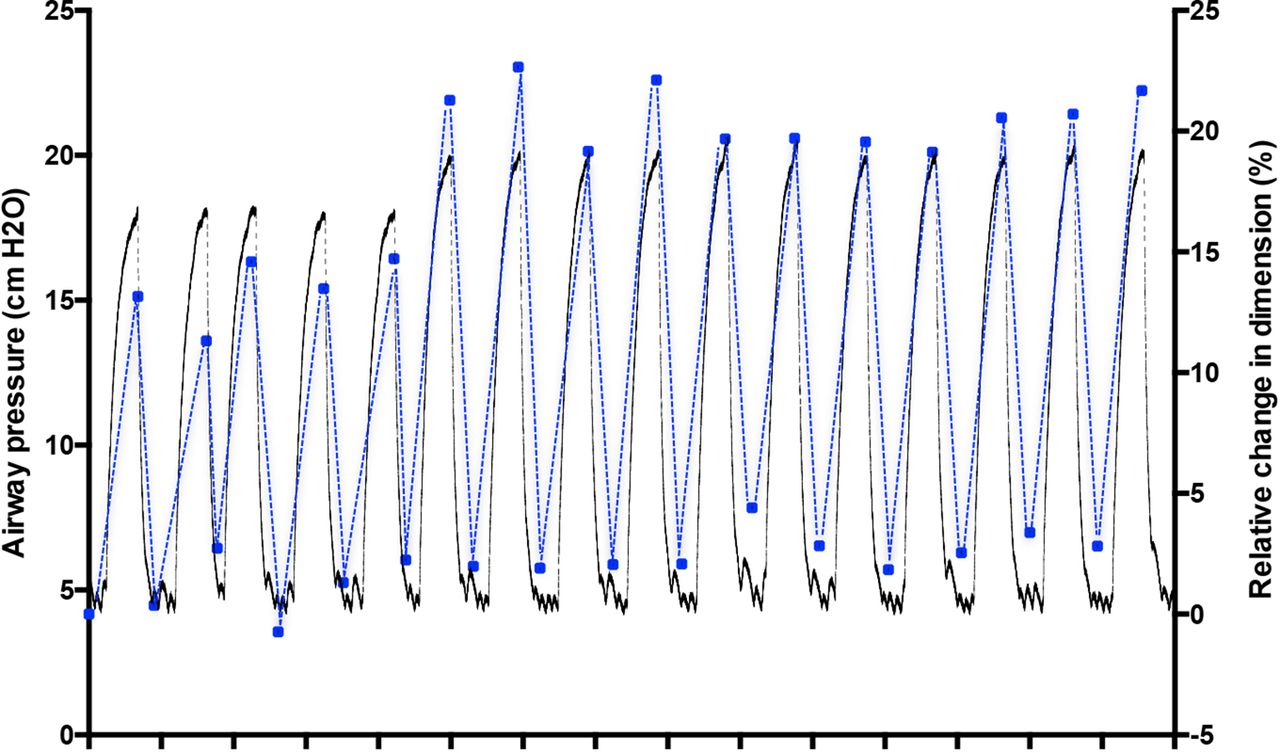
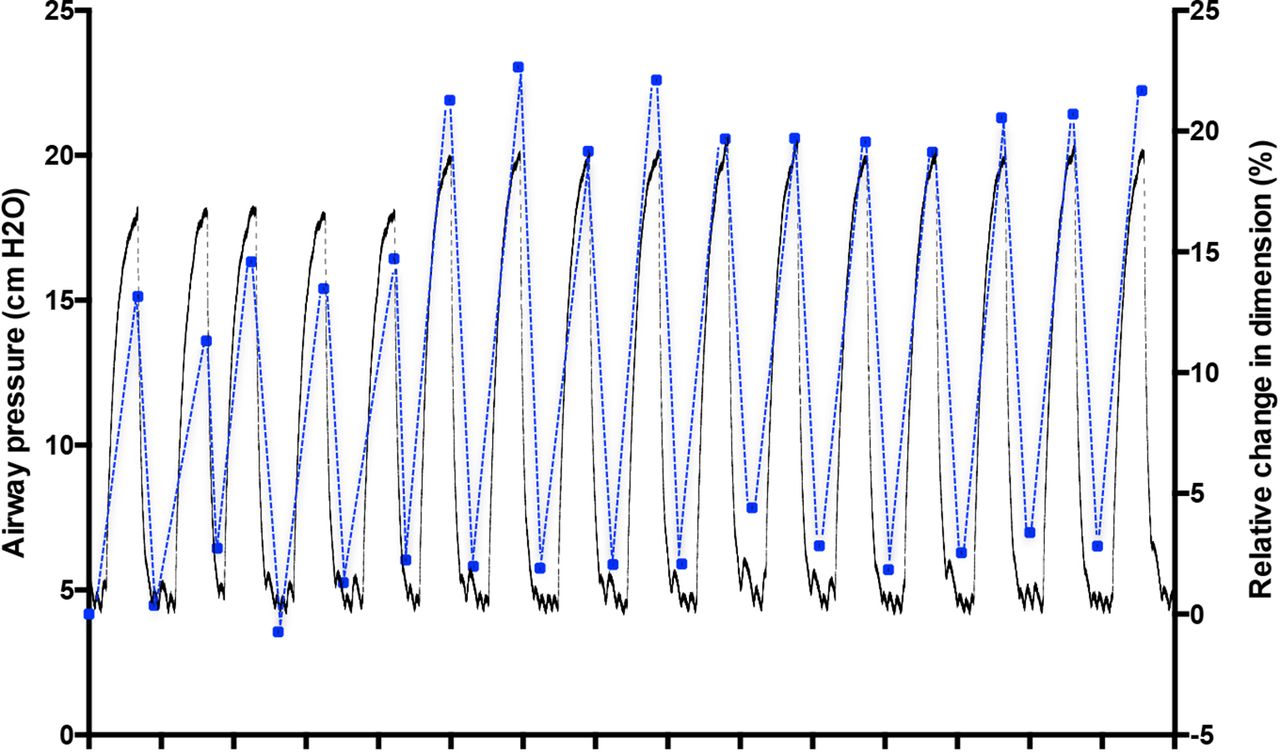
Simultaneous changes in airway pressure (black) and percentage change in pharyngeal diameter (blue) measured during intermittent positive pressure ventilation in a preterm rabbit pup. Measurements of pharyngeal diameter were obtained from consecutive phase-contrast X-ray images and were measured at both peak inflation and near end-expiration at precisely the same point in the pharynx.
Epiglottis
In pups (n=51) with unaerated lungs and unstable breathing patterns immediately after birth (figure 3), the epiglottis was open 17.1%±1.6% of the time (range 6.2±4.7%–51.5±27.5%; figure 6). In contrast, in pups (n=11) with aerated lungs and a stable respiratory pattern (figure 3), the epiglottis was open 72.0%±3.4% of the time (range 36.2±31.8%–96.1±3.9% figure 6). After the first hour (second imaging sequence), the percentage of time the epiglottis was open was 72.3%±2.3% (range 60.3%±14.3%–85.7%±14.3%; n=17, figure 6).
Effect of non-invasive iPPV on pulmonary ventilation
In pups with unaerated lungs and unstable breathing patterns immediately after birth, non-invasive iPPV was unable to ventilate the lung in 16 of 17 attempts (94%; n=12 pups); facemask leak precluded assessment of iPPV in some pups. In the one pup successfully ventilated with non-invasive iPPV, iPPV was initially unsuccessful but after 36 s, the pup took 10–15 breaths in synchrony with the ventilator, which aerated the lungs. After this time, the glottis and epiglottis remained opened, allowing non-invasive iPPV to ventilate the lung.
In pups with a stable respiratory pattern (figure 3), non-invasive iPPV ventilated the lungs in 17 of 22 attempts (77%; n=14). While most (79%) pups became apnoeic during iPPV, allowing the ventilator alone to ventilate the lung, 21% continued spontaneous breathing in phase with the ventilator (figure 4). In the four pups that non-invasive iPPV could not ventilate the lung, spontaneous breathing continued but at a lower rate and the breaths were out of phase with the ventilator.
Effect of CPAP level on spontaneous breathing activity
Sixteen pups had a sufficiently stable respiratory pattern to determine the effects of CPAP on spontaneous breathing rates. Variable facemask leak precluded a systematic assessment of CPAP levels on respiratory function in some pups. As such, CPAP levels >7 cmH2O were compared with CPAP levels <7 cmH2O. CPAP levels >7 cmH2O reduced (p<0.001) respiratory rates from 38.8±3.2 to 12.6±1.8 breaths per minute. The inhibitory effect of CPAP was evident in all pups, causing an almost complete cessation of spontaneous breathing in most pups (figure 4)
Effect of iPPV on pharyngeal dimensions
Non-invasive iPPV caused periodic distension of the pharyngeal wall that was in phase with the change in airway pressure delivered by the ventilator (Figure 5). This periodic pharyngeal distension was evident regardless of whether iPPV occurred when the larynx was closed (lung not ventilated) or open (lung ventilated).
Discussion
While non-invasive ventilation, applied via a facemask, is the preferred mode of respiratory support for very preterm infants, it is unclear how it interacts with the infant’s physiology at birth. As such, it is unclear why non-invasive ventilation is sometimes insufficient, requiring these infants to be intubated immediately after birth.4–6 Our results show that both the glottis (closed 74.5%±1.1%) and epiglottis (closed 82.9%±1.6%) were predominantly closed at birth, opening briefly only during a breath. Thus, non-invasive iPPV was unable to ventilate the lungs unless the preterm pups took a breath, thereby opening their glottis and epiglottis. However, after lung aeration and when a stable breathing pattern was established, both the glottis (open 90.5%±1.9%) and the epiglottis (open 72.3%±2.3%) remained predominantly open. As a result, non-invasive iPPV could ventilate the lungs in most (77%) pups, with the majority (79%) becoming apnoeic during iPPV; the other 21% breathed in synchrony with the ventilator. Pups (23%) that could not be ventilated using iPPV, mostly breathed spontaneously out of synchrony with the ventilator and closed their larynx between breaths. This effect of iPPV on spontaneous breathing has also been observed in preterm human infants immediately after birth.7
During development, glottic adduction during apnoea plays a vital role in fetal lung growth by restricting airway liquid loss.11 12 This helps to maintain a high degree of fetal lung expansion, which is the primary stimulus for fetal lung growth.11 12 As hypoxia suppresses FBMs,18 it also causes glottic adduction19 and this effect of hypoxia persists well into newborn life.20 The hypoxia-induced suppression of FBM contrasts with the increased respiratory drive observed in adults and persists after birth.20 21 As preterm newborns are essentially exteriorised fetuses at birth, it is not surprising that most apnoeic preterm pups had an adducted glottis and could not be ventilated non-invasively. Furthermore, as hypoxia inhibits FBM and causes glottic adduction, one would also expect that hypoxia will suppress breathing activity and stimulate laryngeal adduction in newborns,20 restricting the effectiveness of non-invasive iPPV. While it is unclear whether this occurs in preterm human infants, we would expect the biology to be similar as both preterm rabbits and sheep20 display the same responses and hypoxia is known to inhibit FBM and cause bradycardia in humans.22
In contrast to apnoeic pups, the glottis and epiglottis were predominantly open in pups with aerated lungs and a stable respiratory pattern, allowing most to be ventilated non-invasively. During FBM periods, tonic activity in the glottic adductor muscles cease and the diaphragm and glottic abductor muscles contract in synchrony.10 While it is unclear whether the fetal glottis is ‘predominantly open’ during FBM, it probably is because the resistance to airway liquid efflux through the glottis is greatly reduced during FBM compared with apnoeic periods.23 Furthermore, as preterm pups with aerated lungs and a stable breathing pattern had a ‘predominantly open’ glottis, irrespective of when they were imaged after birth, a ‘predominantly open’ glottis during breathing activity likely occurs both before and after birth and is not a uniquely postnatal event that requires lung aeration. Indeed, it appears to be closely related to a stable breathing pattern, rather than other variables such as the degree of lung aeration.
These findings indicate that establishing a stable respiratory pattern after birth is the greatest priority in assisting very preterm infants to transition to newborn life when using non-invasive iPPV. We found that if preterm pups had a stable respiratory pattern, as the glottis and epiglottis were predominantly open, non-invasive iPPV was able to either augment spontaneous breaths or directly ventilate the lung. As most (~80%) preterm infants display visible breathing efforts at birth,24 one would expect that non-invasive iPPV should be very successful. However, this assumes that the respiratory efforts and/or iPPV are effective at aerating the lung and establishing effective pulmonary gas exchange. All preterm pups imaged in our study displayed visible breathing efforts, but only 17 (out of 62; 27%) pups were able to aerate their lungs and establish a sustained stable respiratory pattern. The majority (73%) of pups had a respiratory rate that varied widely (between 1 and 20 breaths per minute), but these breathing episodes were interspersed with apnoeic periods and were insufficient to aerate their lungs. During apnoea, as the larynx was closed we were unable to ventilate the lung with iPPV and so these pups gradually became more apnoeic and bradycardic and would have required intubation and ventilation if they were not terminated.
As the upper airways of the fetus and newborn are highly compliant,25–28 large pressure gradients generated during spontaneous breathing or iPPV can cause major distortion of the upper airway walls. The pharynx either partially or totally collapsed during inspiration, indicating that resistance within the airways upstream of the pharynx restricted gas flow into the lung, increasing the effort of breathing. It is commonly thought that CPAP reduces the effort of breathing by splinting the upper airways open and preventing pharyngeal collapse during inspiration. We can now confirm that CPAP distends the pharynx, allowing it to act as a reservoir for low resistance gas flow into the lung during inspiration. We also found that during iPPV, irrespective of whether the larynx was open or closed, the pharynx distended in phase with the increase in airway pressure delivered by the ventilator. This is to be expected because, as regardless of the volume of the system, the ventilator will pressurise all open airways to the set PIP value. This will involve pressurisation and distension of just the upper airways when the larynx is closed or both the upper and lower airways when the larynx is open. As the upper airways visibly expand with each inflation, the gas volume entering the lung during non-invasive iPPV is likely to be overestimated. This is consistent with the findings that tidal volumes measured during iPPV in infants and lambs before intubation are significantly higher than tidal volumes measured following intubation, despite the same PIP.29
Hypoxia, resulting from inadequate lung aeration, was probably a major contributor to the apnoea and bradycardia observed and likely dominated the breathing response in our preterm pups.30 Increasing partial pressure of carbon dioxide (PaCO2) levels and reducing core body temperature are thought to play an important role in stimulating continuous breathing at birth.30 31 However, we found that pups with a poor breathing response became increasingly apnoeic despite increasing PaCO2 levels that must have accompanied the hypoventilation. Similarly, while we attempted to keep the preterm pups warm, anecdotally, we found that if pups were cool, they rapidly became apnoeic.
We also found that placement of the facemask (anecdotal finding) and application of facemask pressures >7 cmH2O also inhibited breathing. In apnoeic pups, as the larynx was closed, CPAP simply pressurised the pharynx, which promoted the movement of air into the stomach in pups without an oesophageal tube (figure 1). In pups with a stable breathing pattern, CPAP levels >7 cmH2O greatly reduced respiratory activity, often acting like a switch turning off and on breathing (figure 4). We consider it likely that application of pressure to the face or pressurisation of the pharynx activated receptors that caused reflex laryngeal closure. Indeed, activation of facial receptors that signal via the trigeminal nerve are known to inhibit breathing, including the diving reflex, which is triggered by cold water and is associated with a bradycardia.32
Conclusion
At birth, the glottis and the epiglottis are predominantly closed in preterm pups that have an unstable respiratory pattern, opening only briefly during a breath, making non-invasive iPPV ineffective at ventilating and aerating the lung. However, in pups with a stable breathing pattern, irrespective of when this occurred after birth, the glottis and epiglottis were mostly open, allowing non-invasive iPPV to successfully ventilate the lung. We propose that glottic closure immediately after birth greatly restricts the ability of non-invasive iPPV to aerate and ventilate the lung unless the infant assists by attempting to breathe, which is consistent with observations in humans. These findings underline the importance of stimulating breathing and establishing a stable respiratory pattern at birth when using non-invasive ventilation. Furthermore, to reduce the risk of intubation and mechanical ventilation, factors that inhibit breathing, such as hypoxia, should be avoided as much as possible.
Key points
While airway obstruction restricts non-invasive ventilation in premature newborns at birth, the cause and site of obstruction are unknown.
We have used phase contrast X-ray imaging to show that the glottis and epiglottis are predominantly closed immediately after birth in apnoeic premature rabbits with unaerated lungs opening only briefly during a breath.
When the glottis and epiglottis were closed, non-invasive intermittent positive pressure ventilation (iPPV) was ineffective, unless the pup took a breath.
The glottis and epiglottis were predominantly open in premature pups with aerated lungs and a stable breathing pattern, allowing non-invasive iPPV to successfully inflate the lung, irrespective of time after birth.
Prolonged laryngeal closure at birth may contribute to reduced success rates of non-invasive ventilation in the delivery room for premature newborns.
Acknowledgments
The authors gratefully acknowledge the support provided by the SPring-8 synchrotron facility (Japan), which was granted by the SPring-8 Programme Review Committee, for providing access to the X-ray beamline and associated facilities.
References
Footnotes
Contributors JRC and SBH drafted the work. All authors involved in revising the drafted work critically for important intellectual content; gave final approval of the version published; all are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This research was supported by the Australian Research Council, the Australian National Health and Medical Research Council and the Victorian Government’s Operational Infrastructure Support Program. We acknowledge travel funding provided by the International Synchrotron Access Program (ISAP) managed by the Australian Synchrotron and funded by the Australian Government. C. Binder is supported by the Austrian Science Fund (FWF): J 3595-B19. M. J. Kitchen is the recipient of an ARC Australian Research Fellowship (DP110101941). A. B. te Pas is recipient of a Veni-grant, The Netherlands Organisation for Health Research and Development (ZonMw), part of the Innovational Research Incentives Scheme Veni-Vidi-Vici. S.B. Hooper is a recipient of an Australian National Health and Medical Research Council, Principal Research Fellowship.
Competing interests None declared.
Ethics approval All experimental procedures received approval from SPring-8 Animal Care and Monash University’s School of Biomedical Science’s Animal Ethics Committees
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished work from the study.
Linked Articles
- Fantoms