Article Text

Abstract
Aim To investigate the relationship between active inflammatory lesions on whole-body MRI (wb-MRI) and new development of chronic lesions on T1 MRI in patients with early axial spondyloarthritis (SpA) treated either with etanercept (ETA) or sulfasalazine (SSZ).
Methods Wb-MRIs of 65 patients treated either with ETA (n=35) or SSZ (n=30) over 1 year were scored for active inflammation, fatty lesions, erosions and ankylosis in the 23 vertebral units (VUs) of the spine and in the sacroiliac joints (SI joints). Scoring was performed by two blinded radiologists.
Results If there was no previous inflammation in the bone no new fatty lesions occurred in SI joint quadrants and only a few (0.6%) in spine VUs. There was a significant relationship between disappearance of inflammation and the appearance of fatty lesions: if baseline inflammation resolved fatty lesions occurred in 10.5% of SI joint quadrants and 17.9% of VUs. If inflammation did not resolve over 1 year, fatty lesions occurred less frequently: 2.4% (SI joint quadrants) and 7.2% (VUs). There was a significantly higher increase of the mean fatty lesion score between baseline and week 48 in the ETA (4.0 vs 4.8 for the SI joints and 1.9 vs 2.7 for the spine) compared to the SSZ (3.0 vs 3.2 for the SI joints and 1.1 vs 1.2 for the spine, respectively) group (p=0.001 and p=0.020 for the differences). No significant changes in the erosion or ankylosis score were observed in any of the two groups during this time.
Conclusions These data indicate that there is a close interaction between inflammation, tumour necrosis factor blockade and the development of fatty lesions in subchondral bone marrow of patients with axial SpA.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Treatment of patients with active ankylosing spondylitis (AS) with tumour necrosis factor α (TNFα)-blocking agents has been proven to be highly effective for signs and symptoms1,–,3 and also for the suppression of active inflammation of sacroiliac joints (SI joints) and/or spine on MRI.4 5 Against this background, the failure to retard the growth of syndesmophytes as shown on x-rays over a treatment period of 2 years was at first glance a surprise,6,–,8 and has stimulated an intense discussion about the interaction between inflammation and new bone formation in general and especially in the context of AS.9,–,11 Indeed, it has been shown that TNFα blocks the activity of osteoblasts and inhibition of TNFα stimulates osteoblast activity in a TNF transgenic mouse model of arthritis.10 12 Thus, it has been postulated that TNF inhibits and TNF blockade stimulates new bone formation.9 11 13 In several investigations the question was addressed as to whether inflammation is essential for the development of syndesmophytes or whether new bone formation occurs independently from previous inflammation.11 14 15 Although a correlation between inflammation of vertebral corners at baseline with the growth of syndesmophytes at the same site 2 years later was found in these analyses, new bone formation also occurred at sites with no inflammation at baseline.
Inflammation of subchondral bone marrow (bone marrow oedema) can be demonstrated by the short tau inversion recovery (STIR) sequence of MRI, while chronic changes are seen better or are only visible on MRI T1 sequence.16 17 The MRI T1 sequence is unique among imaging techniques for the detection of fatty lesions of the bone marrow, which is probably the earliest sign of chronic changes as a consequence of inflammation.16 17 A correlation between the presence of active spondylitis on MRI and the subsequent occurrence of fatty lesions at the same sites on MRI T1 has been reported recently in a preliminary study.18 Furthermore, a correlation between fatty lesions and the growth of syndesmophytes has been found19 indicating that fatty infiltration might be a necessary step between inflammation and new bone formation.
In a recent study we reported a good efficacy of etanercept (ETA) treatment over 1 year in patients with early (symptom duration less than 5 years) axial spondyloarthritis (SpA) on active inflammation of SI joints and the spine as shown by MRI and on clinical parameters, in comparison to treatment over the same period with sulfasalazine (SSZ).20 In this prospective study patients were randomised to one of the two treatment arms and whole-body MRI (wb-MRI) was read by two scorers blinded for treatment and time points.
In the present study we analysed the development of chronic changes in the bone on T1 MRI such as fatty lesions, erosions and ankylosis over 1 year, the effect of inflammation at baseline on the development of chronic lesions and the effect of treatment on the development of chronic lesions in patients from this trial.
Methods
Study design
Patients with axial SpA enrolled in a prospective randomised controlled trial were treated with ETA (n=40) versus SSZ (n=36) over 48 weeks.20 All patients showed active inflammatory lesions (bone marrow oedema) on wb-MRI in either the SI joints and/or the spine at baseline (BL).20
For this analysis we included the 65 completers (35 patients on ETA and 30 on SSZ) in whom wb-MRI sets at baseline and week 48 were available. Patient characteristics are shown in table 1.
Baseline characteristics
MRI
Wb-MRIs were performed at weeks 0, 24 and 48 on a 1.5 T scanner (Avanto TIM, Siemens, Erlangen, Germany) according to a previously described protocol.20,–,22 The STIR images were acquired using the following parameters: repetition time (TR) 1660–4590, time to echo (TE) 25–83 and inversion time (TI) 150. The acquired T1 turbo spin-echo (TSE) images comprised a TR of 642–790 and a TE of 10.
Wb-MRIs were scored for active inflammation according to a recently described protocol20 using the STIR sequences. Chronic changes were scored using the T1 sequences in the 23 vertebral units (VUs) of the spine and the 4 quadrants of each SI joint in case of fatty lesions; erosions and ankylosis were only scored for each SI joint as shown in detail in table 2. Scoring was performed by two radiologists, blinded for treatment arm and MRI time point. T1 and STIR images were scored at the same time.
Scores for chronic inflammatory changes on MRI
At baseline, the agreement between both readers (KGH, CA) was high for osteitis and fatty lesions with intraclass correlation coefficients (ICCs) of 0.93 in the spine (SI joints 0.96) for osteitis and 0.97 (0.90) for fatty lesions. ICCs were lower for erosions: 0.82 (0.80) and ankylosis 0.75 (0.96).
Statistics
Main outcome parameters were changes in chronic lesions (fatty lesions, erosions, ankylosis) assessed by MRI T1 sequence and associations between the changes in chronic lesions and changes in active inflammation scores assessed by STIR sequences. To be able to investigate these associations the statistical analysis was restricted to n=65 completers (as described above). The non-parametric analysis of covariance (non-parametric ANCOVA) was used to compare the outcome of the treatment groups by taking the baseline status as covariable into account and the non-parametric Mann–Whitney test was applied to compare treatment groups at baseline. These analyses were based on means of the MRI scores of both readers (KGH, CA) on the patient level. Missing values at week 24 (n=3) were replaced by a so-called expectation maximization algorithm (replacement with an individual mean value from baseline and week 48 adjusted for the overall trend).23
To evaluate the associations between the changes in chronic lesions and changes in active inflammation scores in a very specific manner these possible associations were investigated in the spine on the VU level and in the SI joints on the level of four quadrants per SI joint in case of fatty lesions and per SI joints for erosions and ankylosis. Regarding changes in osteitis scores, three groups (VUs, or quadrants) were analysed separately; group A: both readers agree on no signs of osteitis in the STIR sequence in this unit at baseline and at week 48, group B: both readers agree regarding a resolution of inflammation in this unit, group C: units not assigned to A or B but inflammation present at week 48 according to at least one reader (group C was not further stratified because of insufficient sample size). Regarding the outcome, the development of a new chronic lesion between baseline and week 48, an agreement between both readers was required. Generalised estimation equation (GEE) models with a logit link function were applied to investigate the associations between changes in the MRI scores for fatty lesions and active inflammation. By means of these GEE models groups A, B and C were compared and the percentage of new chronic lesions and their corresponding 95% CIs were estimated by taking possible correlations between chronic and active changes in single VUs (or quadrants) within individual patients into account.24 SAS software (PROC GLIMMIX; SAS, Cary, North Carolina, USA) was used for calculations. p Values <0.05 were considered statistically significant.
Results
Baseline characteristics
The inclusion criteria and the patients' characteristics for this trial have been described recently in detail.20 Patients' characteristics including chronic MRI lesions at baseline are shown in table 1. In the whole group (n=65) fatty lesions were found in 4.5% of VUs (in 26.2% of patients) and in 38.8% of SI joint quadrants (in 69.2% of patients). Erosions were found in only 0.4% of VUs but in 73.1% of SI joints. Ankylosis of VUs occurred in 0.7% in contrast to 6.9% of SI joints.
Occurrence of fatty lesions over 1 year in relation to inflammation
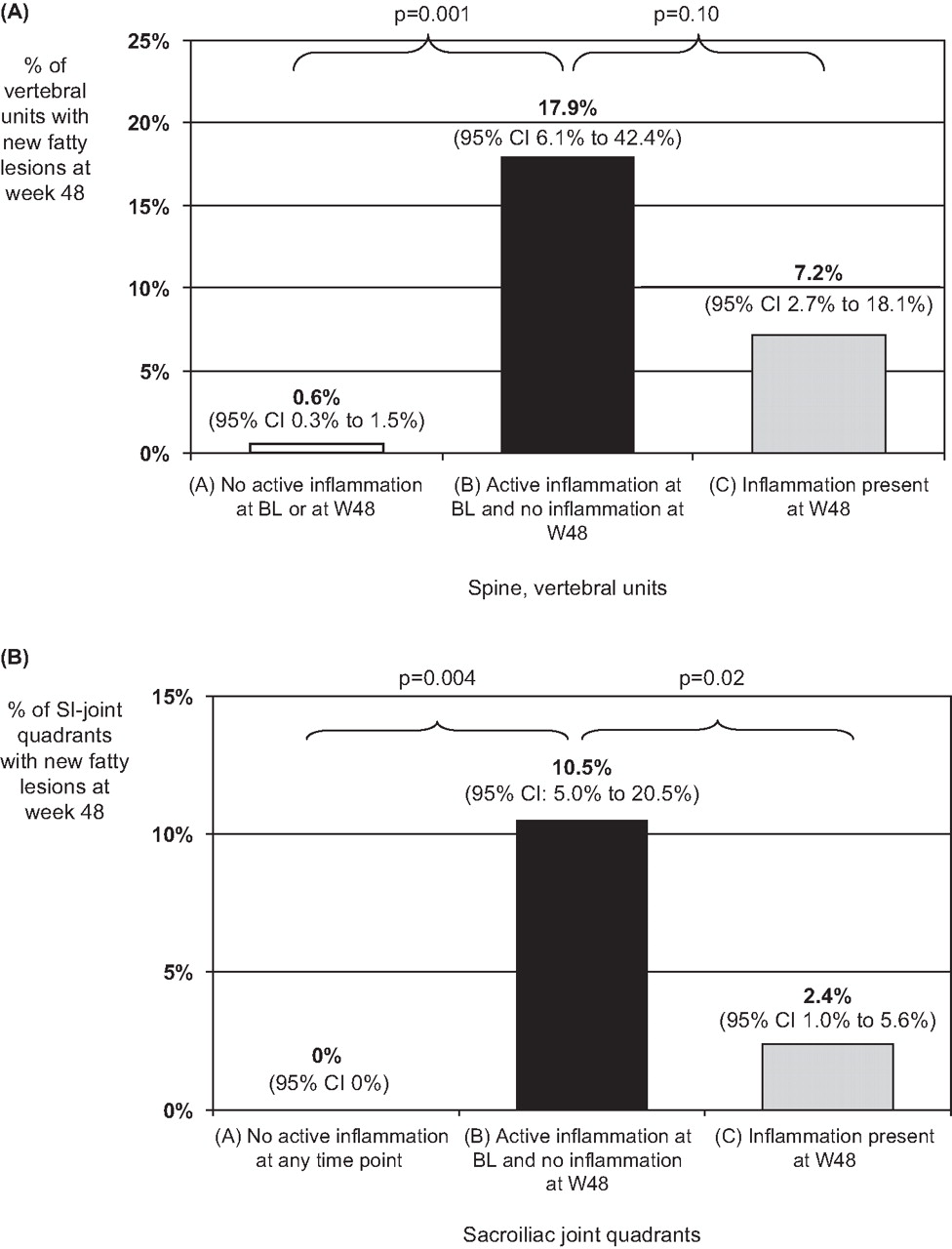
New fatty lesions at week 48 developed in 23 VUs and in 17 SI joint quadrants in all patients. There was a very low rate of new fatty lesions of <1% (0.6% for VUs and 0% for SI joint quadrants) if there was no previous inflammation in the bone (figure 1A for spine VUs and figure 1B for SI joint quadrants). In the presence of baseline inflammation and disappearance of inflammation at all subsequent time points fatty lesions occurred in 17.9% (VUs) and 10.5% (SI joint quadrants), while fatty lesions occurred much less frequently if inflammation was present at week 48: 7.2% in VUs and 2.4% in SI joint quadrants (figure 1A,B). Appearance of new fatty lesions in the SI joints and the spine did not correlate with a change in C reactive protein (SI joints: correlation coefficient=0.018, p=0.34; spine: correlation coefficient=0.055, p=0.95).

Frequency of newly developed fatty lesions at the vertebral units of (A) the spine and (B) the sacroiliac joint quadrants at week 48 in relation to active inflammatory lesions. Percentages shown in the three groups in which (A) there was no active inflammation at baseline (BL) and no inflammation at week 48 (W48) vs (B) there was active inflammation at baseline but no inflammation at week 48 (disappearance of active inflammation) vs (C) there was inflammation present at week 48.
Fatty lesions present at baseline did not disappear over 48 weeks: 0 out of 67 (0%) at VUs and 2 out of 202 (1%) at SI joint quadrants.
When the change of active inflammation was plotted against the change of the fatty lesion score also on a patient level the correlation between reduction of active inflammation and increase of fatty lesions can be seen (see supplementary figure S1). There was a significant correlation between reduction of active inflammation and increase of fatty lesions in the spine (correlation coefficient=−0.39, p=0.001) as well as in the SI joints (correlation coefficient=−0.76, p=0.0015).
Occurrence of fatty lesions compared between the two treatment groups
There was a significantly higher increase of the mean fatty lesion score in the ETA group (4.0 at baseline vs 4.8 at week 48 for the SI joints and 1.9 vs 2.7 for the spine) compared to the SSZ group (3.0 at baseline vs 3.2 at week 48 for the SI joints and 1.1 vs 1.2 for the spine, respectively) (p=0.001 and p=0.020 for the differences between the treatment groups) (table 3). The increase in the fatty lesion score in the ETA group was already visible after 24 weeks (table 3).
Mean MRI SI joint and spine scores for fatty lesions, erosions and ankylosis at baseline, week 24 and week 48 in patients with axial spondyloarthritis treated with etanercept (ETA) or sulfasalazine (SSZ)
The corresponding increase of the fatty lesion score on the patient level is shown in the probability plots in figure 2A (for the spine) and figure 2B (for the SI joints).

Cumulative probability of changes in MRI fatty lesion scores of (A) the spine and (B) the sacroiliac joints from baseline to week 48 in the etanercept and sulfasalazine treatment groups at the patient level. Each data point in figure 2A,B represents an individual patient.
When the nine patients who already had a maximal fatty lesion score of 8 in the SI joints at baseline were excluded from this analysis, the mean baseline values were the same (mean value 2.8) and again the increase in the mean fatty lesion score between baseline and week 48 was significantly (p=0.001) higher in the ETA (from 2.8 to 3.9) as compared to the SSZ group (from 2.8 to 3.0).
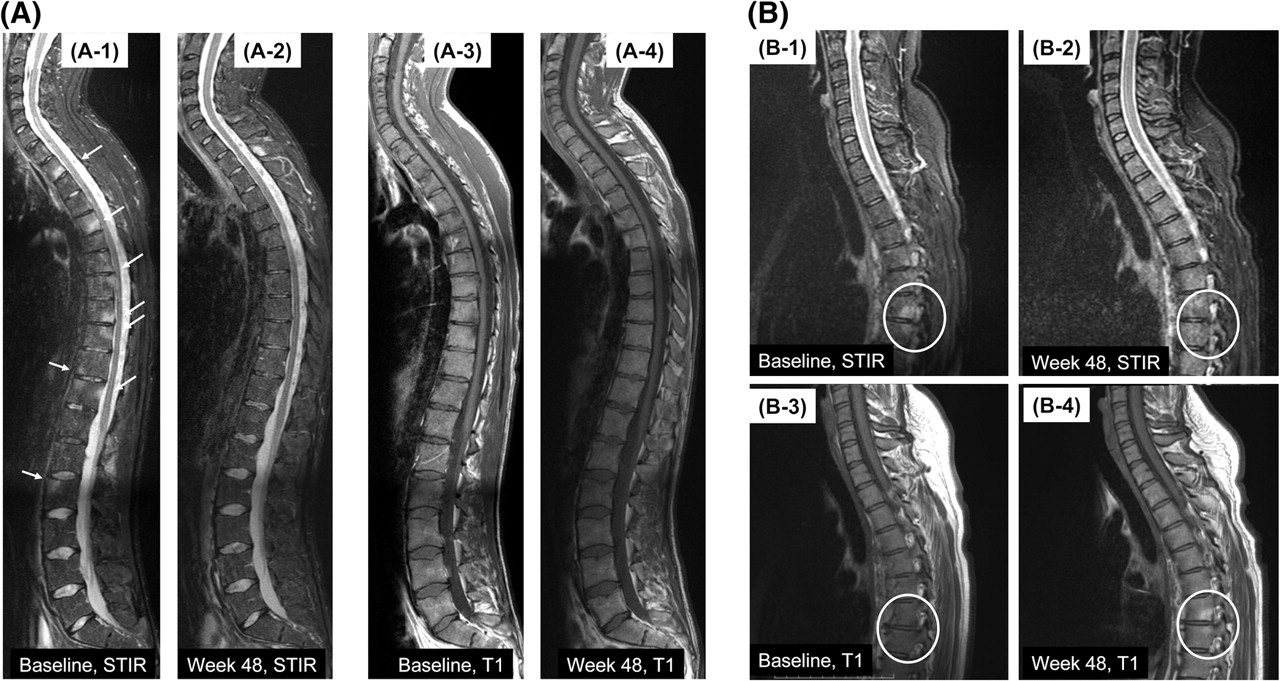
Figure 3 shows MRI examples without (figure 3A) and with (figure 3B) development of fatty lesions in the spine after suppression of active inflammation.

{kind=link}
{kind=link}
{kind=link}
Illustration of spine MRI of two patients treated with etanercept. (A) In patient A active inflammation (as shown by hyperintense signals in short tau inversion recovery sequence) in the spine decreased between (A-1) baseline and (A-2) week 48 but no new fatty lesions developed between (A-3) baseline and (A-4) week 48. (B) Patient B: active inflammatory lesions also decreased between (B-1) baseline and (B-2) week 48 and fatty lesions (as shown by hyperintense sequence in T1 sequence) newly occurred between (B-3) baseline and (B-4) week 48.
Development of erosions and ankylosis over 1 year
As shown in table 3 there was no change in the mean erosion score in the whole group and also no change in the two subgroups (ETA vs SSZ), either in the spine or in the SI joints. The same was true for the mean ankylosis score.
Furthermore, none of the six erosions present in all VUs disappeared (0%). Also, there was no change in the ankylosis score in any of the two groups.
Discussion
In this study we have clearly shown that significant changes of fatty lesions in the SI joints and the spine can be observed over 1 year, but not other changes on T1 MRI: (1) fatty lesions did not occur without previous inflammation in the subchondral bone marrow, (2) the score for fatty lesions increased in patients treated with the TNF blocker ETA but not in patients in the control group treated with SSZ and (3) significant changes in the fatty lesion score could already be seen after 6 months. Finally, (4) no changes in the erosion and ankylosis score were seen over 1 year in any of the two treatment groups. These findings might cast some new light on the interaction between inflammation, chronic bony changes and the development of new bone formation in AS.
Fatty lesions seem to be the first sign of chronic damage in the bone after previous inflammation. This was clearly demonstrated in the current study because fatty lesions occurred only at sites that showed subchondral bone marrow oedema as a sign of active osteitis at baseline, confirming previously reported preliminary results.18 Fatty lesions without previous inflammation occurred very rarely. These few cases might be explained by the fact that MRI might have a sensitivity limit in the detection of inflammation, as was shown in a previous study correlating MRI inflammation and histological inflammation.25 Interestingly, fatty lesions occurred less frequently if inflammation persisted, indicating that the presence of inflammation might inhibit the occurrence of ‘fatty lesions’. However, we cannot exclude a technical problem for this part of the analysis because fatty lesions might not be detectable on an MRI T1 sequence (hyperintense signal) if inflammation is still present (hypointense signal).
The histological correlate of the rather imprecise MRI finding of ‘fatty lesions’ is not clear at this moment, but probably reflects replacement of subchondral bone marrow by some repair tissue through expansion and/or activation of mesenchymal cells such as adipocytes, fibroblasts and osteoblasts.26 27
Fatty lesions at vertebral edges on T1 MRI have also recently been described as early chronic bony changes, which are relatively specific for SpA if they occur at several sites though they do not appear to be different from controls if present only as single lesions in the spine.28 29 Thus, although fatty lesions seem to be useful for following up the sequence of events in SpA from inflammation to chronic damage, they are not unique for SpA unless they show a certain pattern.
The significant increase of fatty lesions in the group of patients treated with ETA over 1 year in comparison to the SSZ-treated group is a very interesting result of the current study. Although such a result seems to be a logical consequence, because ETA was very effective in suppressing active bone inflammation on MRI in the SI joints and the spine in comparison to treatment with SSZ, and active suppression of inflammation was strongly associated with the appearance of fatty lesions, this has not been shown before. Most interestingly, such a (significant) difference between two treatment groups was already visible after 6 months of treatment with a further increase of the difference after 12 months. These data suggest that fatty lesions might prove to be an important early outcome parameter to assess whether suppression of inflammation comes early enough to avoid chronic changes. However, fatty lesions occurred only at about 10% to 20% of cleared inflammatory sites, thus in 80% to 90% of inflammatory sites inflammation was cleared without the occurrence of fatty lesions. We did not find an improvement of fatty lesions in the spine in any of the treatment groups which is in contrast to results from the already mentioned preliminary study.19 However it is difficult to envisage by which mechanism TNF blockade would reverse the presence of fatty lesions.
The key data presented here are further supported by the very similar results obtained for the SI joints and spine, both read blinded to time points. Furthermore, the availability of a control treatment group over 1 year, which was prospectively randomised at baseline, made it possible to compare fatty lesion scores between the two groups.
Beside fatty lesions, erosions and ankylosis are other manifestations of chronic damage in AS.16 17 Erosions were observed in 73% of SI joints but only in 0.4% of VUs in this early axial SpA group. After 1 year of follow-up, we could neither find a change in erosions nor in ankylosis in either of the two treatment groups. If these patients treated with ETA are followed up longer than 1 year, an improvement of an erosion score might be detectable.19 There was a low frequency of ankylosis at baseline, and no change was observed over 1 year. Though MRI is not the method of choice for assessing ankylosis it has been used before for this17 30 and for SI joints;16 however the role of MRI for the assessment of ankylosis has to be evaluated in future studies.
Long-term outcome in AS is determined by new bone formation (ankylosis) in the spine. Therefore the question arises as to how the occurrence of fatty lesions might be connected to this. We postulate that fatty lesions are the first chronic changes after inflammation and that they are necessary for the later development of syndesmophytes. Thus, if fatty lesions can be avoided this might be an early (in the first 6–12 months) indicator that new bone formation can also be avoided. Indeed, in one investigation radiographic syndesmophytes after 2 years were present in 12% of the vertebral edges that showed fatty lesions at baseline but only in 2% of patients without fatty lesions at baseline,31 supporting the proposed link between inflammation, occurrence of fatty lesions and new bone formation. The patients in the current study will be treated long term with ETA and followed up yearly by wb-MRI and by x-rays every 2 years, which will allow this question to be addressed in more detail in the future.
The molecular basis for the link between inflammation and new bone formation in AS is still not clear. It has recently been shown that low serum levels of the molecules sclerostin10 and Dickkopf 1 (DKK1),32 which are both important for osteoclast activation and osteoblast inhibition, are associated with the formation of new syndesmophytes in patients with AS. Thus, taking all imaging and molecular data in AS together, inhibition and/or low levels of inflammation are necessary for the development of chronic lesions such as fatty lesions in subchondral bone marrow and the development of syndesmophytes. The results reported here on fatty lesions in axial SpA that might provide a missing link between these events.
With regard to TNF blocker treatment of patients with axial SpA, we propose the following scenario: early treatment might prevent the occurrence of early chronic changes such as fatty lesions, which was the case in about 80% of inflammatory lesions that were successfully cleared by ETA treatment. Whether or not syndesmophytes will develop from these fatty lesions may no longer be dependent on TNF blocker treatment but rather on the genetic background of the patients and on other treatments such as non-steroidal anti-inflammatory drugs, which might have an effect on new bone formation.33,–,35 However, because continuous successful treatment with TNF blockers may avoid or reduce the occurrence of new inflammatory sites20 36 new chronic lesions may not occur or their appearance may be reduced, because chronic lesions depend on inflammation initially, as shown in the current study. Thus, a reduction of syndesmophytes growth should be detectable in patients treated long term with TNF blockers. However, because the development of the events discussed is a slow process it may take several years of follow-up to prove this. Future long-term follow-up of patients with AS treated with TNF blockers are necessary to confirm the here-proposed concept.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Web Only Data
Files in this Data Supplement:
Footnotes
-
Funding This study was supported by an unrestricted grant from Wyeth/Pfizer.
-
Competing interests I-HS: consulting fees or other remuneration from Wyeth/Pfizer Pharmaceuticals, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals. KGH: None. HH: consulting fees or other remuneration from Wyeth/Pfizer, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals. CA: None. DP: consulting fees or other remuneration from Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals. JL: None. AW: None. BF: former employee of Pfizer/Wyeth. MR: consulting fees or other remuneration from Wyeth/Pfizer, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals, UCB. JS: consulting fees or other remuneration from Wyeth/Pfizer, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals, UCB.
-
Ethics approval This study was conducted with the approval of the Local ethics committee: Landesamt für Gesundheit und Soziales, Geschaeftsstelle der Ethik- Kommission des Landes Berlin, Saechsische Straße 28, 10707 Berlin, Germany.
-
Provenance and peer review Not commissioned; externally peer reviewed.