Article Text

Abstract
Background/aim Keratoconus (KC) is a ectatic corneal disorder with marked progression during childhood and puberty that may lead to severe visual loss. In addition to KC prevalence, estimate shows major geographical variations; recent studies using Scheimpflug technology are in contrast to the 1980s and 1990s literature. The present study aims to determine the prevalence of KC in paediatric patients in Riyadh, Saudi Arabia (KSA).
Methods This prospective, cross-sectional, observational, multicentre study collected data from paediatric patients from 6 years and 21 years of age who were seen at multiple non-ophthalmic emergency departments within KSA. Bilateral corneal measurements were performed using a rotational Scheimpflug corneal tomography system. Two masked examiners established the diagnosis of KC using both objective and subjective screening criteria. Cohen’s kappa coefficient (κ) was used to qualitatively analyse the interexaminer agreement.
Results There were 522 patients (1044 eyes) evaluated, with an average age of 16.8±4.2 years (range 6–21 years). KC prevalence was 5.56% for examiner 1 and 3.83% for examiner 2. The κ was 0.81 (almost perfect agreement), with discrepancy in nine cases, which were jointly evaluated and consensus obtained. Final KC prevalence was 4.79% (95% CI 2.96 to 6.62) or 1:21 patients.
Conclusions The prevalence of KC among paediatric patients in the KSA is considerably higher than numbers reported from earlier studies and from similar studies in other countries. This increase might be due to geographical variations in disease prevalence or due to the ability of screening technology to detect undiagnosed KC with greater accuracy.
- cornea
- epidemiology
- imaging
Statistics from Altmetric.com
Introduction
Keratoconus (KC) is a progressive ectatic corneal disorder characterised by corneal thinning, irregular astigmatism and protrusion of the cornea that may lead to severe visual loss. Both eyes are usually affected, frequently in an asymmetric manner.1 2 Epidemiological studies show that KC affects both sexes and that the disease is more severe in younger patients with marked progression during puberty.1 3 4
KC prevalence estimates show major geographical variations.5 It is still unclear to what extent these variations are due to differences in genetic, environmental or geographic factors. Moreover, different diagnostic tools and age groups used in the various studies probably contribute to this variation. In a study conducted over 48 years, Kennedy et al 4 found a prevalence of 54.5 per 100.000 individuals (0.05%) in a population of the USA. Although performed with limited examination techniques (irregular light reflexes or irregular keratometry mires) that would only identify advanced disease, this study still remains one of the most cited studies. More recently, a number of studies have found a higher prevalence and incidence of KC, especially in the Middle East4 6–12 and Asia13–15 (range 0.76%–3.30%), probably also due to the increased ability to diagnose KC with the improvement of modern corneal imaging.
Determining true KC is critical for several reasons. Public health programmes, campaigns for screening and predicting treatment costs are usually based on the prevalence of a disease in a given population. Moreover, early diagnosis brings the possibility of providing optimal treatment by reducing progression to more advanced stages of vision loss. Procedures such as corneal cross-linking are performed worldwide and have already reduced progressive visual loss and the need for corneal transplantation based on early population-based data.16 Therefore, early diagnosis of KC would allow a better understanding of the population, but more importantly, it could allow appropriate treatment in time for visual acuity not to be greatly impaired.17
The purpose of this study was to evaluate the prevalence of KC identified using Scheimpflug imaging in a paediatric population in Riyadh, Saudi Arabia (KSA).
Materials and methods
This prospective, cross-sectional, observational, multicentre study collected data from subjects between 6 and 21 years of age who were seen at emergency rooms for non-ophthalmic appointments at four different locations in the KSA. After individual confirmation of ancestry through a brief question, only patients of Saudi descent were included. All patients with pre-existing ocular disease other than corneal ectasia or history of ocular surgery were excluded. While not excluded, no patients had a known diagnosis of KC or any related ectatic corneal disorder at the time of their evaluation in this study. For the purposes of this study, we did not attempt to differentiate between KC and other related corneal ectatic disorders such as pellucid marginal degeneration.
All subjects had bilateral corneal evaluations performed using a rotational Scheimpflug system (Pentacam HR, Oculus, Wetzlar, Germany) by the same well-trained individual (WMA). The Pentacam HR is an anterior segment tomography device that allows 3three-dimensional image acquisition. Standard resolution was used to capture images (25 images per scan). Patients were instructed to fix a central red dot and remain with both eyes open in order to maintain correct alignment. If the automated display of quality specification (QS) was not satisfied, the test was repeated until acceptable quality was obtained. Only measurements that had ‘OK’ as QS were used for our analysis.
Regarding the upper age limit of inclusion, some studies consider paediatric patients up to 21 years of age and others stop at 18 years, and multiple definitions are available concerning the age range of a paediatric population. For example, the Centers for Disease Control and Prevention in the USA defines the paediatric population up to 21 years of age.
The study was conducted at multiple sites to be representative of the general population in Riyadh City. It was conducted in accordance with the tenets of the Declaration of Helsinki regarding research involving human subjects. Each subject signed an informed consent form before entering the study and after receiving information on the objective of the research. At the conclusion of testing, patients with suspicious corneal findings as determined by the examiner were provided with contact information to facilitate consultation with cornea specialists from Prince Sultan Military Medical City, King Saud Medical City or King Faisal Specialist Hospital & Research Center.
Data and statistical analysis
The sample size was based on a power calculation with an assumed prevalence of 1% and an error margin of 0.8%. Two masked, experienced ophthalmologists subspecialised in cornea and refractive surgery (JBR and EATN) at different institutions rated all corneal images using subjective pattern analysis combined with objective metrics (maximum keratometry, regional corneal thickness values and Belin/Ambrósio Total D value (BAD-D) scores, among others) and categorised the eyes into three categories: normal, suspect or KC. To avoid characterisation of borderline cases or those without clear established diagnostic criteria as KC and thereby unduly inflate prevalence estimates, we relied on distinct (although subjective) focal abnormality of anterior corneal curvature with concomitant corneal thinning for KC diagnosis. For the present study, only the eyes referred as KC were used for prevalence data. The prevalence was provided in terms of patients and not eyes, so if one eye graded KC, then the patient was considered to have KC.
Descriptive statistics were used for basic demographic data and prevalence reporting. Cohen’s kappa coefficient (κ) was used as a means to qualitatively analyse the inter-rater agreement between the examiners.18 Cohen’s κ is considered a more robust statistical method than the sole calculation of the percentage, since it measures the randomly corrected proportion of matching scores.18
There are several guidelines for interpreting the kappa coefficient. Landis and Koch established the following: values <0 as indicating no agreement and 0–0.20 as slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial and 0.81–1 as almost perfect agreement.18 19 Another approach was made by Fleiss, who considered kappa over 0.75 to be excellent agreement among examiners, 0.40–0.75 as fair to good and below 0.40 as poor.20
In order to obtain the overall prevalence of the sample, we defined that in cases where there is a certain degree of discrepancy between the examiners, there would be a new, unmasked evaluation of the disputed scans performed by both examiners in order to obtain a consensus. If there was no consensus, a third arbitrator examiner (ophthalmologist, specialised in cornea and refractive surgery) would make an assessment. The overall prevalence was reported as a percentage, with a 95% CI.
Results
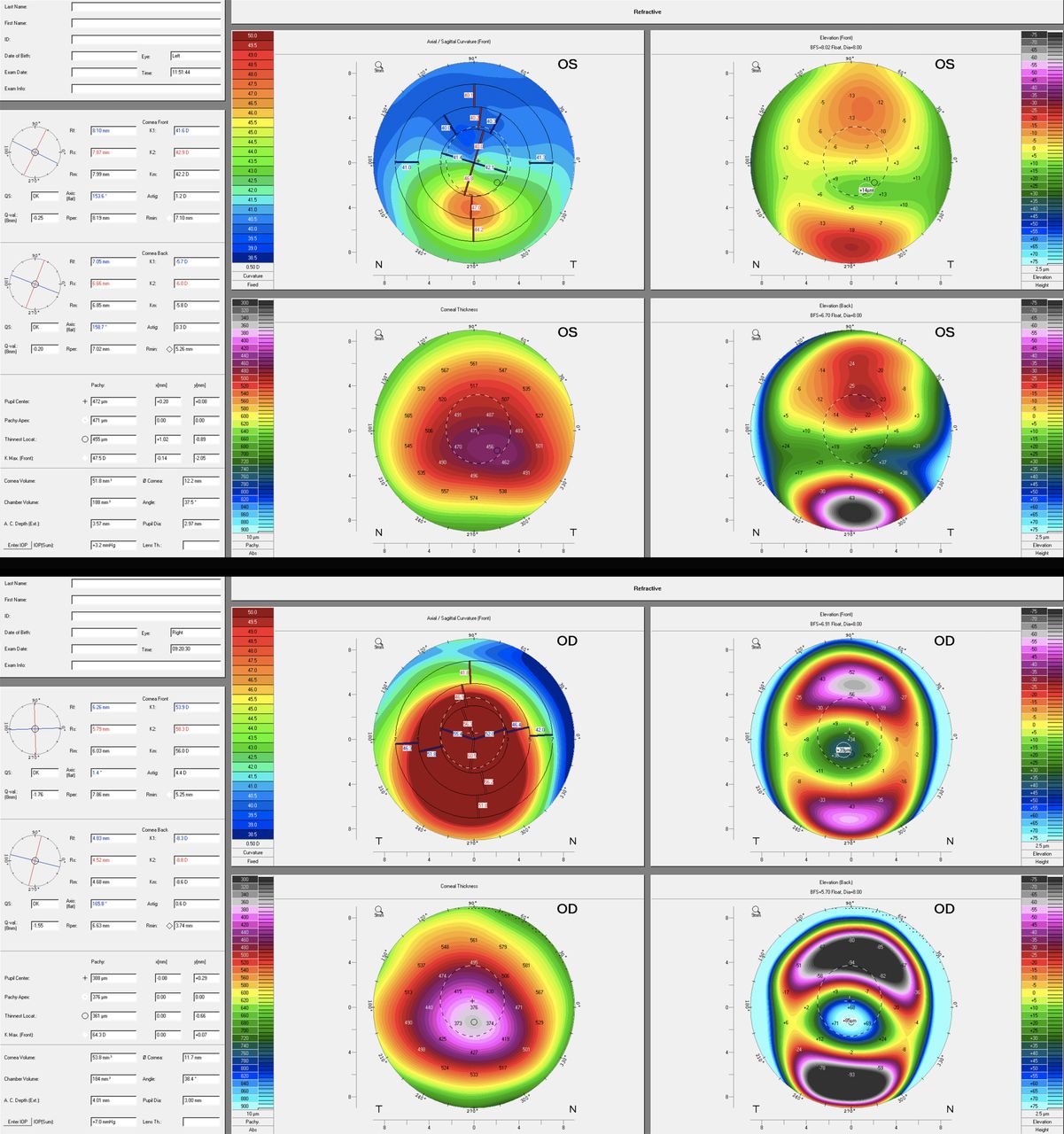
There were 522 patients (1044 eyes) evaluated, with a mean age of 16.8±4.2 years (range 6–21 years) (table 1). Individual prevalence values were 5.56% (approximately 1 in 18 patients) for examiner 1% and 3.83% (approximately 1 in 26 patients) for examiner 2. Figures 1 and 2 show representative images from eyes considered normal (figure 1, left), suspect (figure 1, right) and KC (figure 2, left/right). While rating was based in part on subjective pattern analysis, all eyes classified as KC had focal corneal steepening >3D with coincident focal paracentral corneal thinning and BAD-D scores >2.0.
Patient demographics

(Upper) Representative image from eye considered normal. The subjective anterior curvature pattern was determined to be a regular, with a symmetric bowtie. Kmax is 43.2D; there is 2.1D of anterior astigmatism, pachymetry at the apex is 549 µm with the thinnest point of 540 µm located +0.49/–1.20 mm (x/y axis). BAD-D (not shown) was 0.49. (Lower) Representative image from eye considered suspicious. The subjective anterior curvature pattern was determined to be irregular, with an asymmetric bowtie and skewed axis. Kmax is 45.1D; there is 1.9D of anterior astigmatism; pachymetry at the apex is 515 µm with the thinnest point of 492 µm located +0.63/–1.18 mm (x/y axis). BAD-D (not shown) was 3.58.
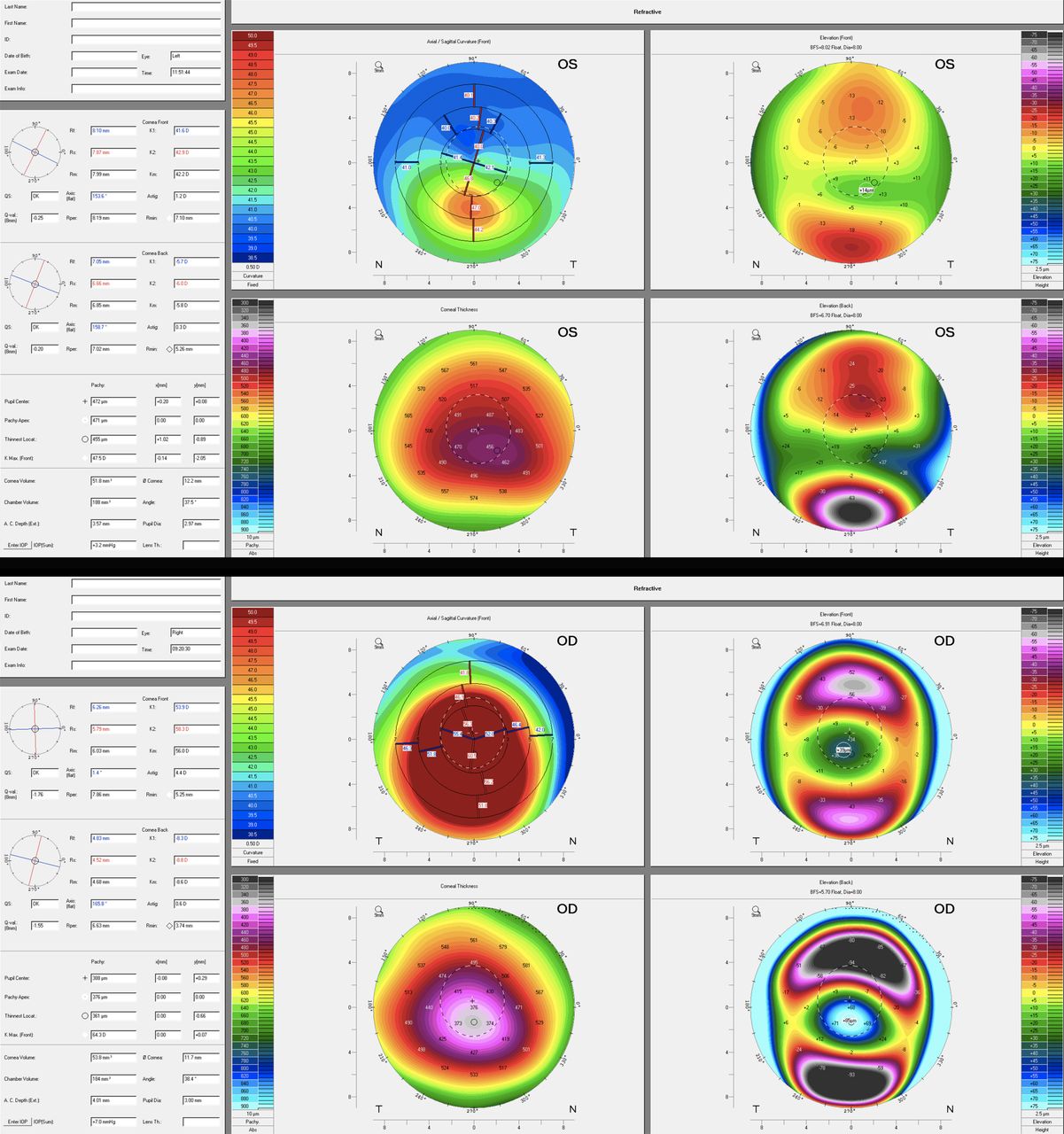
(Upper) Representative image from eye considered mild keratoconus. The subjective anterior curvature pattern was determined to be irregular, with focal inferior paracentral steepening up to 7D. Kmax is 47.5D; there is 1.2D of anterior astigmatism, pachymetry at the apex is 471 µm with the thinnest point of 455 µm located +1.02/–0.89 mm (x/y axis). BAD-D (not shown) was 4.75. (Lower) Representative image from eye considered severe keratoconus. The subjective anterior curvature pattern was determined to be irregular, with generalised severe steepening. Kmax is 64.3D; there is 4.4D of anterior astigmatism; pachymetry at the apex is 376 µm with the thinnest point of 361 µm located +0.00/–0.66 mm (x/y axis). BAD-D (not shown) was 16.21.
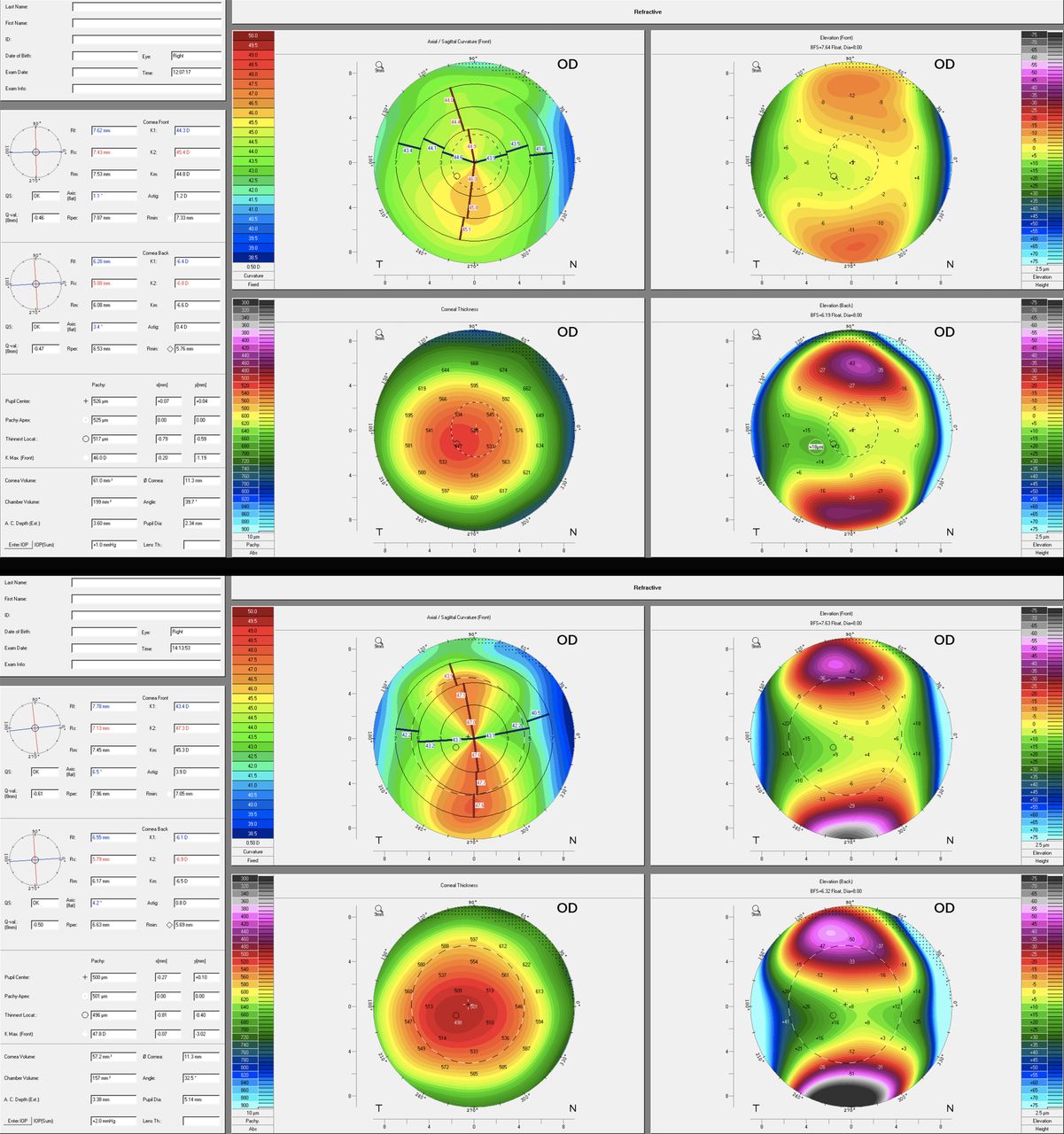
There was discrepancy in diagnosis between the examiners in 9/522 patients (1.7%). Cohen’ s κ of agreement was 0.81, indicating ‘near perfect’18 19 or ‘excellent’20 agreement. The nine disputed cases were then jointly evaluated in order to reach a consensus. Figure 3 (left/right) shows representative images of disputed cases. All exams are presented on a fixed scale. Finally, a concordance between examiners was obtained in all cases. The final prevalence was 4.79% (1 in 21 patients) (table 2). The 95% CI of this sample was 2.96% to 6.62%.
Keratoconus prevalence by age category
{kind=link}
{kind=link}
{kind=link}
(Upper) Representative image of disputed case, ultimately considered suspicious. The subjective anterior curvature pattern was determined to be irregular, with an asymmetric bowtie bordering on focal steepening and mild skewing of the axis. Kmax is 46.0D; there is 1.2D of anterior astigmatism, pachymetry at the apex is 525 µm with the thinnest point of 517 µm located −0.79/–0.59 mm (x/y axis). BAD-D (not shown) was 2.74. (Lower) Representative image of disputed case, ultimately considered keratoconus. The subjective anterior curvature pattern was determined to be irregular, with a skewed axis of nearly 60° in the periphery. Kmax is 47.8D; there is 3.9D of anterior astigmatism; pachymetry at the apex is 501 µm with the thinnest point of 496 µm located −0.81/–0.40 mm (x/y axis). BAD-D (not shown) was 2.72.
Discussion
The purpose of this study was to determine the prevalence of KC in Saudi children and adolescents between 6 years and 21 years of age in the region of KSA, based on Scheimpflug corneal tomographic imaging. The prevalence was 4.79%, which represented 1:21 subjects. This prevalence is significantly higher than in all previous reports on KC prevalence.4 7–15 21 22
In 1986, Kennedy et al 4 published their landmark paper on the epidemiology of KC. Based on the examiner’s description of irregular light retinoscopic reflexes and irregular mires detected with keratometry over a span of 48 years, the prevalence of KC was estimated in the population of Minnesota, USA. The overall prevalence of KC was 0.05%, which corresponds to approximately 1:2000 patients, and so far, this study is the most cited reference on the subject. In 2000, Pearson et al 13 were the first to suggest that ethnicity may influence the incidence and severity of KC. In their study, a fourfold increased incidence was found in patients of Asian descent (0.23%) when compared with Caucasian patients (0.05%).13 More recently, a large-scale evaluation from the Netherlands’ mandatory health insurance database showed prevalence approximately fivefold higher than previous reports, around 0.27%, or 1:375 patients.22 The prevalence estimate was derived from database review searching for KC diagnosis rather than corneal imaging analysis, and the mean KC diagnosis age was 28.3 years; thus, it is simultaneously uncertain that all patients identified actually had true KC and yet still likely that this rate represents an underestimation of disease as this strategy would not identify milder KC cases.
In contrast to other manuscripts in which database from medical records or diagnostic codes were evaluated,13 21 22 our study determined the diagnosis of KC based solely on masked examiners analysing corneal imaging from modern screening technology. In addition, our study evaluated a representative young population who underwent medical consultation without any ophthalmological complaint or previous diagnosis. With a prevalence of 4.79%, our results show a drastic difference (95-fold increase) in the prevalence of KC when compared with earlier studies, which represents the highest rate reported to date.
Little is known about the occurrence of KC in the KSA. Previous studies have shown that the prevalence of KC in the Middle East is considerably higher than in other areas of the world.7–12 To date, the highest prevalence reported was 3.30% (approximately 1:30 patients) from a population of medical students from Lebanon using Placido-based imaging (TMS-4, Tomey) to establish the diagnosis.8 Another study conducted in Israel found a KC prevalence of 3.18% when analysing 314 students with a mean age of 25 years.11 It is worth noting that such studies7–12 were performed with corneal topography or tomography, which are more sensitive tests than those described during the 1980s.4 23 Just as in our study, screening with modern technology is certainly a determining factor23 and may be partially responsible for the increase in the estimated prevalence of the latest studies. Consanguinity may also represent a confounding risk factor for KC.24
There remain no absolute objective criteria for differentiating between the suspect and mildest KC and related ectatic disorders stages. Some variability exists in repeat measurements in keratoconic eyes using the same imaging device,25 and mild variability exists when imaging both keratoconic and normal corneas when using different devices.26 For these reasons, we cannot completely extrapolate our findings to other studies using different imaging technology, and we chose to report the CIs specifically to provide some sense of the possible variability that could exist.
There are some limitations to acknowledge. The first one is the general limitation every study faces that uses a ‘human interface’ to assess clinical outcomes: we report a minor discrepancy between the two examiners in a total of nine patients or 1% of the study population. Those patients were borderline cases between non-manifest KC suspect and early manifest KC. However, even when analysing the extremes (ie, considering all nine borderline cases to be non-manifest KC vs considering all of them to be manifest KC), the change in prevalence would only be minimal, from 1:26 to 1:18. In both cases, this study would report the highest prevalence in the normal population described to date. The second limitation is the cut-off point for KC-suspected cases, which is not well defined in the literature. However, because the vast majority of cases diagnosed had distinct KC, the range of these cut-off points would be of lesser importance to the prevalence reported here. Third, and most importantly, this study relied solely on corneal tomographic imaging without clinical patient examination. While this could be considered a limitation, we feel the addition of a slit lamp examination would add very little to the diagnosis of earlier KC cases, and these would in fact be specifically identified using corneal tomography in the absence of clinical signs. Furthermore, we were unable to evaluate the visual impact of various presentations of KC in this population. Such data would be highly informative but was beyond the scope of this study. Also due to the lack of clinical examination, it is possible that a small number of these eyes could have had a disease process other than a corneal ectasia. However, given the consistency of KC patterns combined with the lack of specific ocular history for all patients, it is unlikely that another corneal disorder was present but misclassified as KC. Lastly, this might not be a true population-based study once it was conducted on patients seen at emergency departments at a few medical centres in Riyadh. We can therefore not exclude that the prevalence rates would be different if the study was performed at schools. However, since patients were not presenting with any eye-specific complaints, we feel this sample is reasonably representative of the population. Given the significant prevalence of KC in this population, it seems warranted to consider a school-based screening protocol.
In conclusion, the prevalence of KC among children and adolescents of Saudi origin in the KSA is considerably higher than numbers reported from similar studies. This discrepancy might be due to geographical variations in disease prevalence and also to the use of modern large-scale corneal imaging in a paediatric population. Moreover, it raises the imminent question of a KC screening programme in schools to improve the early detection and early adequate intervention.
References
Footnotes
Contributors Research design: WMA-O, NLH and FH; data acquisition and/or research execution: EATN and WMA-O; data analysis and/or interpretation: EATN, SK, JBR and FH; and manuscript preparation: all authors.
Funding Light for Sight Foundation, Zurich, Switzerland. Deanship of Scientific Research, King Saud University, Saudi Arabia.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The was approved by the ethical committee at Prince Sultan Military Medical City (PSMMC), King Saud Medical City (KSMC) and King Faisal Specialist Hospital & Research Center (KFSH & RC) in Riyadh, Saudi Arabia.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance